
Abstract
Background and Purpose:
Robot-assisted partial nephrectomy (RAPN) is an emerging technique for minimally invasive nephron-sparing surgery that may facilitate the technical challenges of sutured renorrhaphy. Barbed suture allows for knotless wound closure and improves suturing efficiency. We present the first clinical study of barbed suture for renorrhaphy during RAPN in human patients and compare perioperative outcomes to RAPN with polyglactin suture.
Patients and Methods:
Thirty consecutive patients underwent RAPN by a single surgeon; 15 using polyglactin suture for renorrhaphy followed by 15 using the V-Loc 180™ wound closure device. Renorrhaphy was performed in two layers, with a continuous running closure of deep vessels and the collecting system, followed by a running closure of the renal capsule, using the sliding Hem-o-lok clip technique. Operative characteristics and complications were compared between groups.
Results:
Renorrhaphy was successfully completed in all 30 consecutive RAPN procedures. V-Loc and conventional groups were equivalent in demographic and tumor characteristics. Mean operative and console time were equivalent; warm ischemia time was significantly shorter in the V-Loc group (18.5 vs 24.7 min, P = 0.008). There were no instances of suture slippage or tearing in the barbed suture group. The barbs held the sliding clip renorrhaphy intact without the need for redundant clips to prevent backsliding.
Conclusion:
Use of barbed suture simplifies the renorrhaphy technique during RAPN and improves efficiency, allowing for reduced warm ischemia times. We demonstrate feasibility and safety of this suture technique in human patients undergoing minimally invasive partial nephrectomy.
Introduction
Barbed suture is a technology that has been used for efficient wound closure in plastic surgery and gynecology, 6 –10 but reports are limited regarding potential urologic applications. Our hypothesis was that barbed suture could potentially improve efficiency of renorrhaphy during partial nephrectomy by resisting slippage and precluding the need for constant traction. In this article, we present 30 consecutive transperitoneal robot-assisted partial nephrectomy (RAPN) procedures, 15 using the V-Loc 180™ barbed suture for renorrhaphy and 15 using polyglactin sutures, immediately preceding this change in technique. We describe our initial experience and outcomes.
Patients and Methods
A total of 30 consecutive patients underwent RAPN by a single experienced robotic surgeon (CGR). Written informed consent was obtained in all cases. Renorrhaphy was performed in the first 15 cases using braided polyglactin suture (Vicryl, Ethicon, Johnson & Johnson, Somerville, NJ), after which a change in technique was made to incorporate the use of the V-Loc 180 absorbable wound closure device (Covidien, Mansfield, MA).
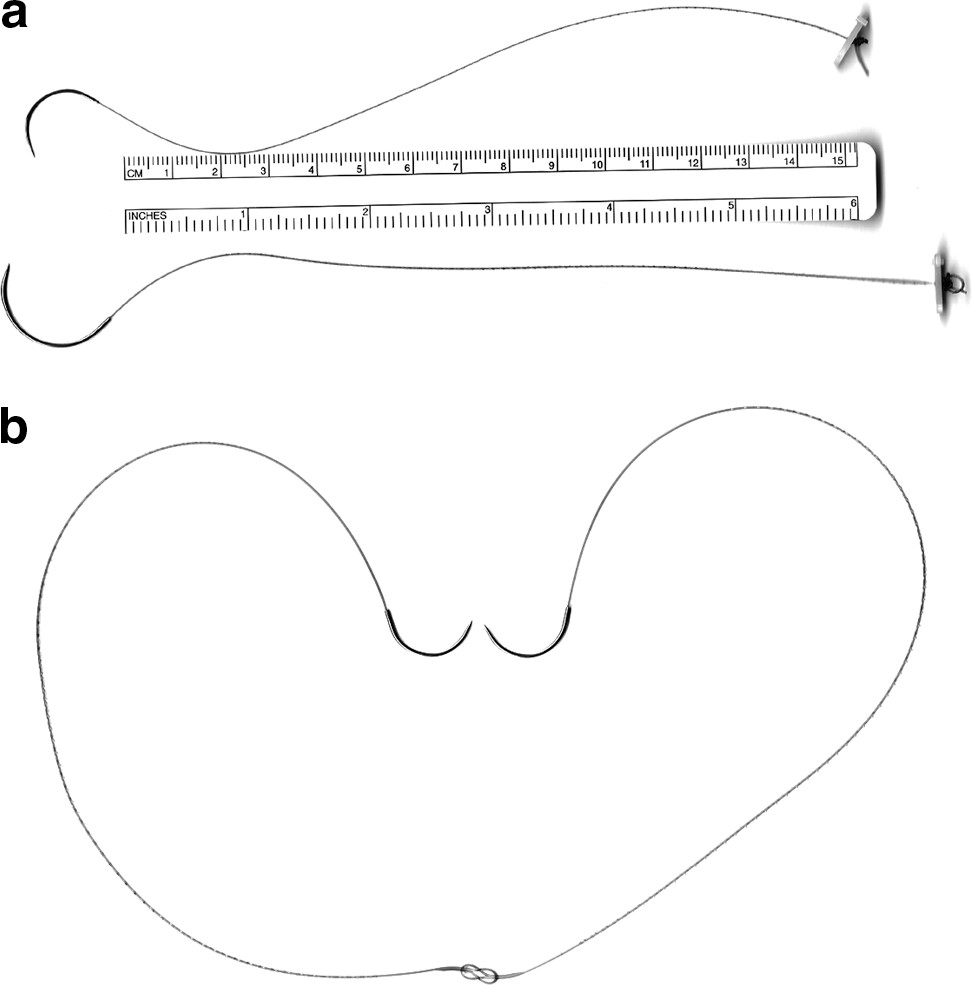
The V-Loc 180 absorbable wound closure device is a unidirectional barbed variant of the absorbable copolymer polyglyconate (Maxon, Covidien). It has the same material and degradation properties as Maxon (monofilament polyglyconate) suture; wound closing strength is approximately 50% at 30 days with complete absorption in 180 days. While etching the barbs reduces the core diameter of these sutures, they have been sized according to their postetching diameter. For example, 2-0 and 3-0 V-Loc sutures have the same tensile strength as 2-0 and 3-0 Maxon, respectively. A loop at the end of the suture can be used for knotless suturing, although we did not use this in our study, and the first 2 cm of the suture are without barbs to allow throws to be readjusted before the barbs are engaged (Fig. 1).

The unique characteristics of the V-Loc 180™: (
Barbed sutures used in the study are depicted in Figure 2. We used 6-inch 3-0 V-Loc sutures on V-20 needles (26 mm tapered, similar to an SH) for the inner renorrhaphy layer. To close the renal capsule, we used 12-inch 2-0 V-Loc sutures on GS-21 needles (36 mm tapered, similar to a CT-1) cut to 7 to 8 inches. A knot was placed at the trailing end of each suture and secured with a large Weck Hem-o-lok® clip (Teleflex Medical, Research Triangle Park, NC), to anchor the first throw. In the first three V-Loc cases, the V-Loc suture was made bidirectional by running the needle of two 6-inch sutures each through the looped end of the opposing suture (Fig. 2b), allowing for a single suture to be used for both renorrhaphy layers. The midpoint knot was anchored with a Surgicel® (Ethicon, Johnson & Johnson, Summerville, NJ) pledget to help prevent tearing of the knot through the renal capsule.
(
Renorrhaphy was performed in two layers, regardless of suture type. There was no substantive difference in suture placement, suture length, or needle size between the barbed suture and standard renorrhaphy techniques. Deep-layer closure was performed in a running baseball stitch fashion, ligating vessels and repairing the collecting system if entered (Fig. 3). The renal capsule was closed with sutures that were placed in an interrupted fashion across the defect, and the sliding Hem-o-lok clip technique was used to tighten and secure the sutures as previously described. 4 Gaps in the rennorhaphy were closed using these same sutures in a running mattress or baseball stitch fashion (Fig. 4). With polyglactin renorrhaphy, additional clips were needed to anchor the clips to prevent them from sliding back. This was not necessary with the barbed suture renorrhaphy. Renorrhaphy was performed under warm ischemia with hilar clamping, using bulldog clamps, in all cases. No formal early unclamping procedures were performed in either group.
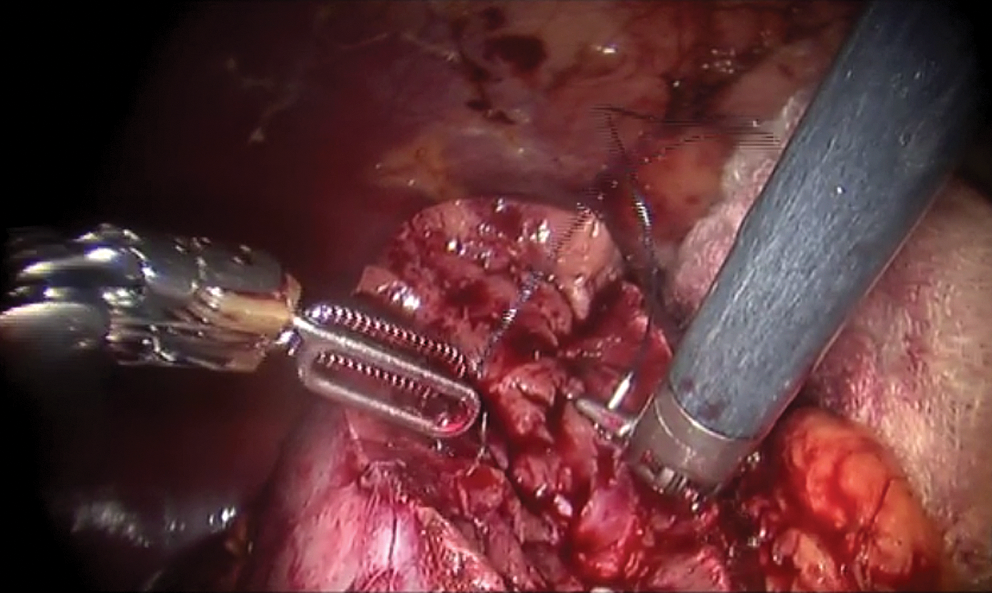
Deep layer renorrhaphy during robot-assisted partial nephrectomy with a 6-inch 3-0 V-Loc 180 on a V-20 needle. The barbs on the suture prevent slippage and allow for efficient two-handed renorrhaphy without the need to maintain tension of previous throws of the stitch.

Closure of the renal capsule with a 12-inch 2-0 V-Loc on a GS-21 needle (36 mm tapered, similar to a CT-1) cut to 7 inches. A running mattress closure was performed with each throw anchored with a Hem-o-lok clip. The barbs on the suture prevent clips from sliding back, so additional clips are unnecessary to anchor the sliding clip renorrhaphy.
Age, body mass index, American Society of Anesthesiologists (ASA) score, tumor size, percentage of endophytic tumor, total operative time, console time, warm ischemia time, estimated blood loss (EBL), and length of stay were compared between the two groups. The Levene test was used to test for the equality of variance between the two groups. Normality of the distribution was tested using the Shapiro-Wilk test and confirmed with the Kolmogorov-Smirnov test and graphical displays. Of the variables tested, age, tumor size, ASA score, total operative time, EBL, and length of stay were not distributed normally. Hence, the Mann-Whitney U test was used for these variables. For the other continuous variables, the independent samples t test was used. The Pearson chi-square test was used to compare the cases that involved entry of the collecting system and the Fisher exact test was used to compare postoperative complication rates. All tests were two-sided with significance level set at 0.05. The statistical analysis was performed using PASW software (PASW 17, IBM, Chicago, IL).
Results
A total of 15 consecutive patients underwent successful RAPN with polyglactin suture for renorrhaphy followed by 15 patients with the V-Loc 180 wound closure device. Table 1 demonstrates the comparative outcomes between the two groups. Demographic and tumor characteristics were equivalent. Mean operative and console time were found to be equivalent; warm ischemia time, however, was significantly shorter in the V-Loc group (18.5 vs 24.7 min, P = 0.008). All barbed suture renorrhaphy procedures were performed without instances of suture slippage or tearing. The barbs held the sliding clip renorrhaphy intact without the need for extra clips to prevent the clips from sliding back.
Mean difference 6.2 minutes (95% confidence interval, 1.7–10.7 min).
SD = standard deviation; BMI = body mass index; ASA = American Society of Anesthesiologists.
There was a single focal, microscopic positive margin in the polyglactin group in a patient who underwent tumor enucleation and who has elected to pursue close surveillance. There were two postoperative bleeding incidents in the polyglactin group (none in the V-Loc group), both of which necessitated transfusion and one angioembolization. Median follow-up was 1 month for the V-Loc group and 4.5 months for the polyglactin group.
Discussion
NSS has evolved to become the preferred method of management of small renal masses, 1 offering preservation of renal function compared with radical nephrectomy 11,12 with evidence of improved survival. 13 LPN has demonstrated comparable functional and oncologic outcomes to open partial nephrectomy with improved convalescence. 14,15 RAPN has emerged as a viable alternative to facilitate the technical challenges of LPN, demonstrating perioperative outcomes at least comparable with LPN with the benefit of reduced warm ischemia times. 4,16 –18 A technical modification that has improved efficiency of renorrhaphy during RAPN and helped reduce warm ischemia times is the sliding clip renorrhaphy technique by Benway and associates. 4
We incorporated barbed suture into the sliding clip renorrhaphy technique during RAPN. In our experience, the V-Loc barbed suture allowed the surgeon to work efficiently with both hands and focus exclusively on subsequent stitch placement, without the need to maintain tension on preceding throws to prevent slippage. The V-Loc barbed suture distributed tension evenly across the renorrhaphy, allowing for good tissue apposition and hemostasis. The improvement in efficiency with barbed suture helped us to achieve a 25.1% reduction in mean warm ischemia time (6.2 minutes; P = 0.008) compared with our previous renorrhaphy technique.
To address the possibility that part of this efficiency gain was because of progression in the learning curve rather than suture type, we compared operative characteristics in the control group with the 15 RAPNs that immediately preceded them. This analysis demonstrated no difference in warm ischemia time, EBL, total operative time, tumor size, or complexity (data not shown). All surgeries were performed by a surgeon with >100 previous cases, well beyond the estimated learning curve of 30 cases to optimize warm ischemia time during RAPN. 4,19
The first description of barbed suture was for the repair of flexor tendons of the palms and fingers. 20 Barbed suture has been used by plastic and gynecologic surgeons for procedures including abdominoplasty, breast reduction, myomectomy, and hysterectomy. 6,7,9,10 The V-loc 180 absorbable wound closure device was initially studied for skin closure. Subsequent studies on porcine enteric anastomoses by Demyttenaere and colleagues 21 demonstrated closure equivalence with Maxon, equivalent histopathologic inflammatory response at 3, 7, and 14 days, but faster anastomosis times.
Studies that relate to the use of barbed suture in urology are limited, 22 –24 and most have been performed in porcine or model systems. We have previously reported our technique using V-Loc suture for urethrovesical anastomosis during robot-assisted radical prostatectomy. 25 Our study is the first to report on the use of barbed suture for renorrhaphy during RAPN in human patients and to compare perioperative outcomes with polyglactin sutures commonly used in renorrhaphy.
Weld and coworkers 23 performed an in vivo porcine study that compared 0 Quill SRS™ PDO (Angiotech, Vancouver, CA) barbed suture and 2-0 polyglactin in laparoscopic pyeloplasty and bladder neck anastomosis. They demonstrated equivalent efficacy and operative time between the suture types, but raised concerns relating to postoperative histologic changes. They noted significantly higher lamina propria fibrosis and perianastomotic fat fibrosis, but no differences in muscle fibrosis and granulation tissue with the polydiaxonone barbed sutures when used for bladder neck anastomosis. No difference in inflammatory response was seen using the same sutures for pyeloplasty. The impact of barbs or suture composition on the inflammatory response is unclear, as is the clinical relevance in kidney surgery.
Shikanov and colleagues 24 performed the first study of barbed suture for renorrhaphy during LPN in a porcine model. They performed lower pole heminephrectomy on 20 renal units and performed renorrhaphy with either Quill SRS PDO or polyglactin. All renorrhaphy procedures were performed in two layers using 2-0 suture for the inner layer and #1 suture for the capsular layer. They found equivalent procedure time, ischemia time, and suturing time, as well as hematoma and urinoma formation and leakage rates on necropsy.
We noted several advantages of renorrhaphy using barbed suture, including increased efficiency, decreased warm ischemia times, and a nonsignificant reduction in overall procedure time. When performing the renorrhaphy, the suture barbs allow for a closure without the need to maintain constant tension, and they prevent slippage of the suture or clips to maintain tighter tissue apposition. We still use Hem-o-lok clips to secure the barbed suture as in the standard technique, as Benway and associates 26 demonstrated that the sliding-clip distributes compressive force, providing closing pressure superior to other closure techniques without ripping through the renal parenchyma. With barbed suture, however, redundant clips are not needed to reinforce these clips to prevent them from sliding back. All of these factors contributed to efficiency gains.
Several limitations of this study and the technique of barbed suture renorrhaphy deserve comment. While the first 2 cm of the suture are without barbs (Fig. 1), allowing for readjustment of the throw without adverse effects, it is difficult to retract sutures or adjust throws once the barbs are engaged in the tissue. There is also a hypothetical concern of increased inflammation or fibrosis caused by the suture barbs. Although this may be of concern in urethrovesical anastomosis, we feel it is of little significance for partial nephrectomy, and we have noted no short-term adverse events. In addition, the absorption profile of the V-loc 180 is longer than that of polyglactin. This should be of no significance in renorrhaphy; nevertheless, barbed suture with a shorter absorption profile may soon be available.
One consideration regarding the use of barbed suture for rennorhaphy is cost (3-0 V-loc sutures are $23.65, 2-0 are $27.45, while 2-0 and 0 polyglactin sutures are $4.25. Hem-o-lok clips are $4.00 per clip. Mitigating the increased barbed suture cost is the decrease in suture and Hem-o-lok clip usage. Formerly, we premade two capsular stitches per cm of renal mass (ie, six 0 polyglactin sutures for a 3-cm mass) and at least three sutures for the inner layer. We now usually use only four barbed suture—two for the inner layer and two for the outer. We also use only a single Hem-o-lok clip to secure the leading suture end at the conclusion of renorrhaphy vs two previously. The average closure cost of a 3-cm defect is, therefore, $158.80 using V-Loc, compared with $146.25 using polyglactin. We think a $12.55 increase in cost per case is negligible, given the increases in efficiency gained. The collective decrease in warm ischemia time or operative time over multiple cases could also contribute to cost savings. Also, there are potential cost benefits to society of a reduction in warm ischemia time in terms of preservation of renal function.
Our study pertained to only RAPN and did not analyze the use of this suture with other partial nephrectomy approaches. We think, however, that the use of barbed suture for renorrhaphy and the potential benefits would also apply to LPN or open partial nephrectomy. Further studies, with long-term follow-up are needed to further define the role of barbed suture for renorrhaphy in partial nephrectomy.
Conclusion
We present the first clinical application of V-Loc 180 barbed suture for use in renorrhaphy during partial nephrectomy, demonstrating safety and feasibility. Incorporation of barbed suture simplifies the renorrhaphy technique and improves efficiency during minimally invasive partial nephrectomy, resulting in reduced warm ischemia times.
Footnotes
Disclosure Statement
No competing financial interests exist.