
Abstract
Background and Purpose
: Renal fossa recurrence of renal-cell carcinoma (RCC) after radical nephrectomy historically necessitates open surgical resection. Cryoablation provides a minimally invasive alternative to open resection for local recurrence. We describe our experience with percutaneous cryoablation in three patients who were experiencing fossa recurrence.
Patients and Methods
: We retrospectively reviewed medical records of three patients with renal fossa recurrence of RCC who were treated with percutaneous cryoablation.
Results
: Percutaneous cryoablation was well tolerated; no complications were noted, and patients were discharged within 23 hours. One patient needed an additional cryoablation procedure, and one patient underwent subsequent open extirpation. Metastatic disease developed in one patient, while the other two patients remain negative for disease by axial imaging and percutaneous biopsy. All patients are alive at 43 months (range 22–54 months).
Conclusions
: Percutaneous cryoablation, a minimally invasive intervention, has low morbidity and may be offered as an alternative to extirpation, although long-term oncologic data are lacking.
Introduction
Patients and Methods
After obtaining Institutional Review Board approval, we retrospectively reviewed the medical records of patients with renal fossa recurrence of RCC who were treated by one attending urologist. A choice of cryoablation or open surgical resection was offered to patients with no obvious evidence of metastatic disease. Three patients elected to undergo percutaneous cryoablation, with one patient needing two procedures. The procedure was performed with the patient prone in the CT scanner under conscious sedation with local anesthesia.
Because the kidney was no longer in situ, spinal needles were sometimes used to infuse normal saline into the retroperitoneum to create a space between the colon and mass (Fig. 1). Three or four Galil® 17-gauge cryoablation needles (Galil Medical, Yokneam, Israel), in addition to one temperature probe positioned in the center of the mass, were advanced with CT guidance. Two freeze–thaw cycles were performed, with 8 minute hold at first freeze, 6 minute hold at second freeze, and 5 minutes allowed for thawing between cycles. Iceball formation was monitored radiographically (Fig. 2). If iceball formation appeared insufficient, a third freeze cycle with a 5 minute hold was performed to ensure adequate thermal damage. The freeze temperature was −70°C.

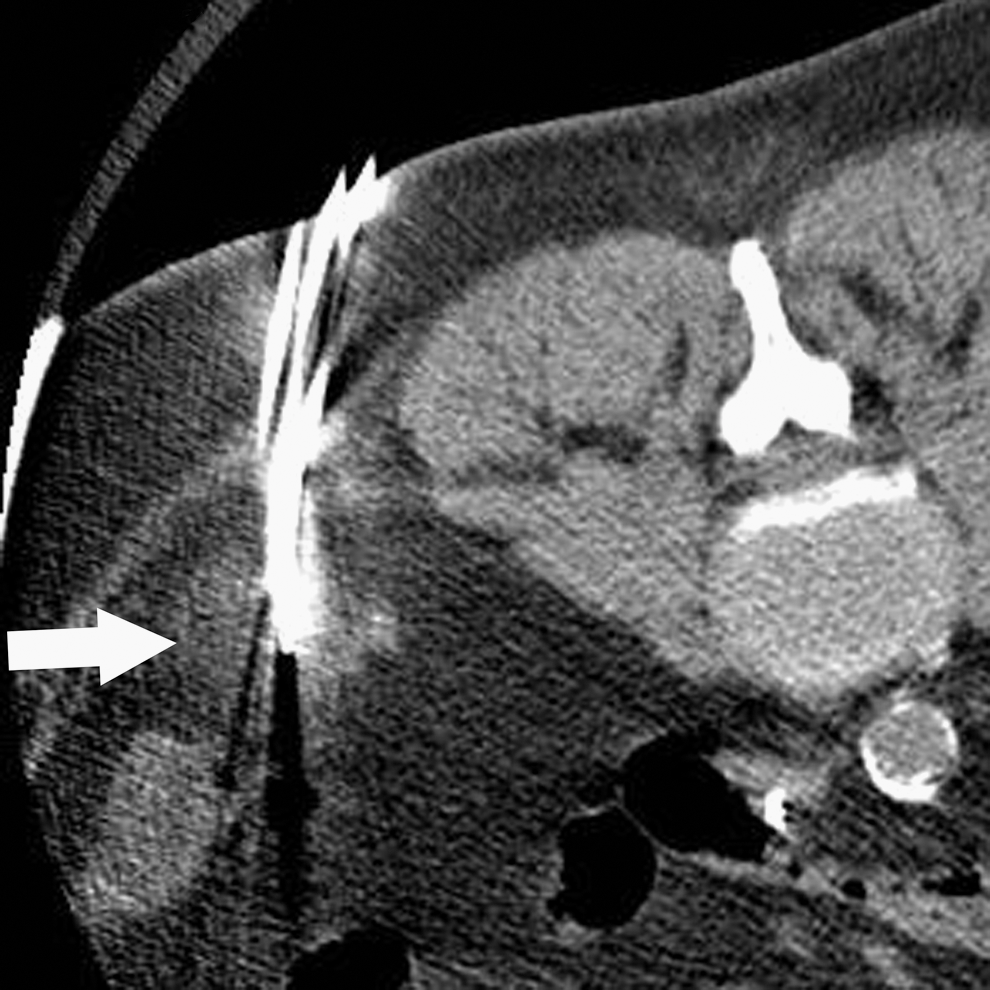
An iceball (arrow) appears as a hypodensity surrounding the cryoablation needles.
Each patient remained in the hospital for 23-hour observation, including postoperative hemoglobin checks in recovery and before discharge. After cryoablation, patients were followed with axial imaging of the abdomen and pelvis every 3 months, in addition to periodic chest radiography and liver function studies.
Results
Table 1 includes characteristics of the three patients, who were men with previous nephrectomies for clear-cell carcinoma. One of the three had bilateral nephrectomies and received a renal transplant before recurrence. All recurrences were remote, with an average time to recurrence of 46 months (range 27–71 mos). Characteristics related to original pathology, recurrence, and treatment are summarized in Table 1. Before treatment, all patients were believed to be free of metastasis, although one patient had lung lesions on CT that were too small to characterize. All recurrences were identified on surveillance scans and were noted to be enlarging or enhancing. The average size of the fossa mass was 2.8 cm. All three recurrences were pathologically proven to be clear-cell carcinoma, either before or at the time of cryoablation.
Fourth needle placed after first freeze-thaw cycle to ensure adequate iceball formation.
Patient currently receiving sunitinib (Sutent®) for metastatic disease. Before cryoablation, patient had lung lesions on chest radiography and CT that were too small to characterize.
BMI = body mass idex; TNM = tumor, node, metastasis.
Each patient underwent percutaneous cryoablation with at least two freeze–thaw cycles, as described previously. The average procedure time was 89.3 minutes. Postprocedure hemoglobin levels were stable. No complications were noted, and all patients were discharged to home within 23 hours. Two of the three patients needed further treatment. Patient 1 underwent repeated cryoablation for continued rim enhancement. Imaging at 3 and 6 months postablation revealed central necrosis with persistent rim enhancement. When the enhancement had not resolved by the 9-month CT scan, the patient chose to repeat percutaneous cryoablation. A biopsy obtained at that time demonstrated residual or recurrent tumor. Patient 2 showed an increase in the size of his mass on his third follow-up CT at 9 months postablation, and he elected to undergo open surgical extirpation through a midline incision. The mass excision was not exceedingly difficult, with final pathologic evaluation revealing a 5 × 2 cm Fuhrman grade 3 to 4 clear-cell carcinoma, mostly surrounded by skeletal muscle but coming within 1 mm of the margin. Lung lesions that had been too small to characterize before his cryoablation or surgical extirpation began enlarging and were diagnosed as metastatic RCC, for which he is currently receiving sunitinib.
At this writing all patients are still alive, with a mean overall survival since initial recurrence ablation of 43 months (range 22–54 months). All three continue to be monitored with serial axial imaging every 3 months. In addition, patients 1 and 3 underwent repeated percutaneous biopsy of lesions after treatment. Biopsy results were negative, demonstrating coagulation necrosis or organizing hematoma with no evidence of malignancy. No disease is evident in these patients at 22 and 47 months.
Discussion
Isolated renal fossa recurrence is rare and may behave differently from other metastases. Itano and associates 4 demonstrated that although renal fossa recurrence portends a poor outcome, surgical resection improves survival. In that study, ipsilateral recurrence in the renal fossa developed in 30 of 1,737 patients who were treated with radical nephrectomy. Those who were treated with observation (n = 9) had a 5-year cause-specific survival of 13%, whereas those who were treated with surgical resection (n = 10) had a 5 to 7 cause-specific survival of 51%. Medical therapy (n = 11), including radiation, chemotherapy, or immunotherapy, also had dismal results, with a survival rate of 18%. Surgical resection was associated with significant morbidity, however, with 67% of patients undergoing surgical resection needing blood transfusions and 33% having perioperative complications. The average hospital stay for recurrence resection was 12 days. Schrödter and colleagues 5 also showed in a series of 16 patients that aggressive surgical management may result in prolonged survival but that ≥50% of such patients ultimately succumb to metastatic disease.
To improve the risk–benefit ratio, a minimally invasive but oncologically sound procedure should be explored. Laparoscopic surgical resection may minimize morbidity but still requires general anesthesia and hospitalization. 6 McLaughlin and coworkers 7 explored thermoablative techniques for fossa recurrence, using CT-guided, percutaneous radiofrequency ablation under general anesthesia to treat a 5.5 × 7.0 cm mass. There were no complications, and the patient had evidence of continued mass regression with no enhancement at 16 months. In our series, all patients were discharged within 23 hours of the procedure. There were no complications, and no patients needed blood transfusions. All procedures were performed in less than 2 hours with no patient needing general anesthesia. While long-term data are lacking and our series is small, the results are encouraging in regard to cancer control; two of three patients have no evidence of disease after cryoablation.
Laparoscopic-assisted or percutaneous cryoablation is an emerging technology for the management of RCC. Promising short-term success rates have been reported with few complications. This form of therapy is especially attractive for patients with comorbidities. 8 –10 Cryoablation is believed to achieve its results both by freezing-based direct cell injury and freezing-based vascular injury. Direct cryoinjury occurs by intracellular ice formation and dehydration. Moreover, changes in intracellular lipids and proteins promote cell death. Vascular injury is caused in part by vessel distension, which ultimately results in cell sludging. Alternating coagulation and thrombosis leads to stasis. If the vessel recovers, there is an additional risk of a reperfusion injury. Both direct cell injury and vascular injury culminate in tumor necrosis. 11 In the series reported by Schwartz and colleagues 12 of 85 cryoablation procedures for solitary renal masses with a mean follow-up of 10 months, one patient had pathology-proven recurrence. The complication rate for percutaneous cryoablation ranges between 8% and 21%, with most complications being minor and not necessitating further intervention. 9,13
The combination of its demonstrated potential to cure RCC and infrequency of clinically significant complications make cryoablation of renal fossa recurrences an attractive option. It has not yet been determined which patients should be offered this technique. Certainly, anatomic considerations must play a role, because cryoablation is not likely to be successful for masses abutting large vessels and could be risky for masses adherent to bowel. Two options for elevating bowel that may have slipped into the renal fossa after nephrectomy include prone positioning and injection of saline to create a buffer. For obese patients or those with respiratory concerns, prone positioning may be safer performed under general anesthesia. One should also consider the thickness of the abdominal wall, as a cutdown may be necessary to accommodate the length of the needles.
The three patients described here returned to their daily routines quickly, a benefit especially valuable to those in whom metastatic disease is present but not symptomatic. That being said, treatment does not end with the procedure. Appropriate patient selection is key, because close surveillance is necessary. Two of the three patients needed additional surgical management, because there was evidence of disease after the first intervention. A potential explanation for local failure could be that the recurrence has increased angiogenesis and vascularity, decreasing the ability of cryoablation to cause vascular injury. With close follow-up, the response of the lesion can be identified and, if necessary, re-treatment scheduled. We image the patients with either contrast-enhanced CT or MRI every 3 months. Biopsy is helpful in determining whether the mass is residual scar tissue and necrosis or residual/recurrent malignancy. Repeated cryoablation or surgical open surgical resection can be safely performed after initial cryoablation failure.
Although further studies are necessary to validate cryoablation in comparison with surgical extirpation for cure, cryoablation should be considered an option, especially for those with multiple comorbidities.
Conclusion
Percutaneous cryoablation provides a minimally invasive intervention with low morbidity. The patient must be followed closely and may require re-treatment, however. Mass biopsy is a helpful adjunct when deciding on further treatment. As with surgical extirpation, success is dependent on recurrence being limited to the renal fossa.
Disclosure Statement
Kristina Suson, M.D., Howard Richard: No competing financial interests exist.
Michael Phelan, M.D., is a consultant for MidAtlantic Cryo.