
Abstract
Purpose:
To study the feasibility and safety of laparoendoscopic single-site (LESS) radical nephrectomy, we compared the operative results with conventional laparoscopic radical nephrectomy.
Patients and Methods:
Ten patients underwent LESS radical nephrectomy for renal tumors (group 1). Two types of single-port devices, a SILS port and a homemade single-port device that was made using a surgical glove and a wound retractor, were used through a 4-cm periumbilical incision. The operative results of LESS radical nephrectomy matched those of 12 patients who underwent conventional laparoscopic radical nephrectomy (group 2). For comparing the 2 groups, the Mann-Whitney U test and the Fisher exact test were used.
Results:
LESS surgeries were completed successfully, without conversion to conventional laparoscopic or open surgery. The patients' characteristics did not differ significantly between the two groups. The mean operative times in groups 1 and 2 were 127.7 ± 22.3 minutes and 126.1 ± 43.1 minutes, respectively (P = 0.235). The mean estimated blood loss was 185.7 ± 121.9 mL and 324.0 ± 187.0 mL, respectively (P = 0.65). The complication rates were 10% and 17%, respectively (P = 0.658). The mean times to postoperative initiation of ambulation and initiation of oral intake were not different in the two groups (1.1 vs 1.0 days, P = 0.269; 1.0 vs 1.0 day, P = 1.0). The mean lengths of hospital stay were 6.5 and 6.1 days (P = 0.435). The mean tumor sizes were 4.0 cm and 5.2 cm (P = 0.345).
Conclusions:
LESS radical nephrectomy is technically feasible and comparable to conventional laparoscopy. Long-term follow-up and technical development, however, are needed for assessing the cancer-control effect and facilitating the minimal invasiveness of the surgery.
Introduction
Laparoendoscopic single-site (LESS) surgery is one of the advancements in the field of urology. It has gained popularity because it needs a smaller incision, which improves postoperative recovery and cosmesis. 6,7 Recent studies presented the initial experiences of LESS renal surgeries, including simple nephrectomy, donor nephrectomy, radical nephrectomy, and partial nephrectomy. 8 –11 Comparative studies with conventional laparoscopy, however, have been rarely reported. 10
We present our experience of LESS radical nephrectomy and compare the operative results with those of conventional laparoscopic radical nephrectomy.
Patients and Methods
Between March 2009 and April 2010, a total of 43 patients underwent LESS renal surgeries in a single center. The surgeries included renal cyst excision, pyeloplasty, adrenalectomy, simple nephrectomy, radical nephrectomy, partial nephrectomy, and total nephroureterectomy. Ten patients who underwent LESS radical nephrectomy were included in this study (group 1). Twelve patients who underwent conventional laparoscopic radical nephrectomy in the same period served as a control group (group 2). Patients freely chose an operative method without any limitation. All operations were performed by a single surgeon. Preoperative laboratory tests and radiologic studies, including abdominopelvic CT, were performed.
LESS radical nephrectomy was performed transperitoneally. The patients were placed in a 70-degree lateral position. Two types of single-port devices were used. Initially, a homemade-port device, made with a size 6 surgical glove and a small-sized Alexis wound retractor (Applied Medical, Rancho Santa Margarita, CA), was used for seven patients. It was inserted into the peritoneal cavity through a 4-cm periumbilical incision. Four trocars were inserted into the glove of the homemade port and fixed using rubber bands. For the recent surgeries for three cases, however, we used a commercially available, multiple-instrument access port (SILS port, Covidien, Norwalk, CT). This port device was inserted into the peritoneal cavity through a 4-cm periumbilical incision. In addition, a 12-mm balloon trocar (Applied Medical, Rancho Santa Margarita, CA) was inserted into the incision (Fig. 1).
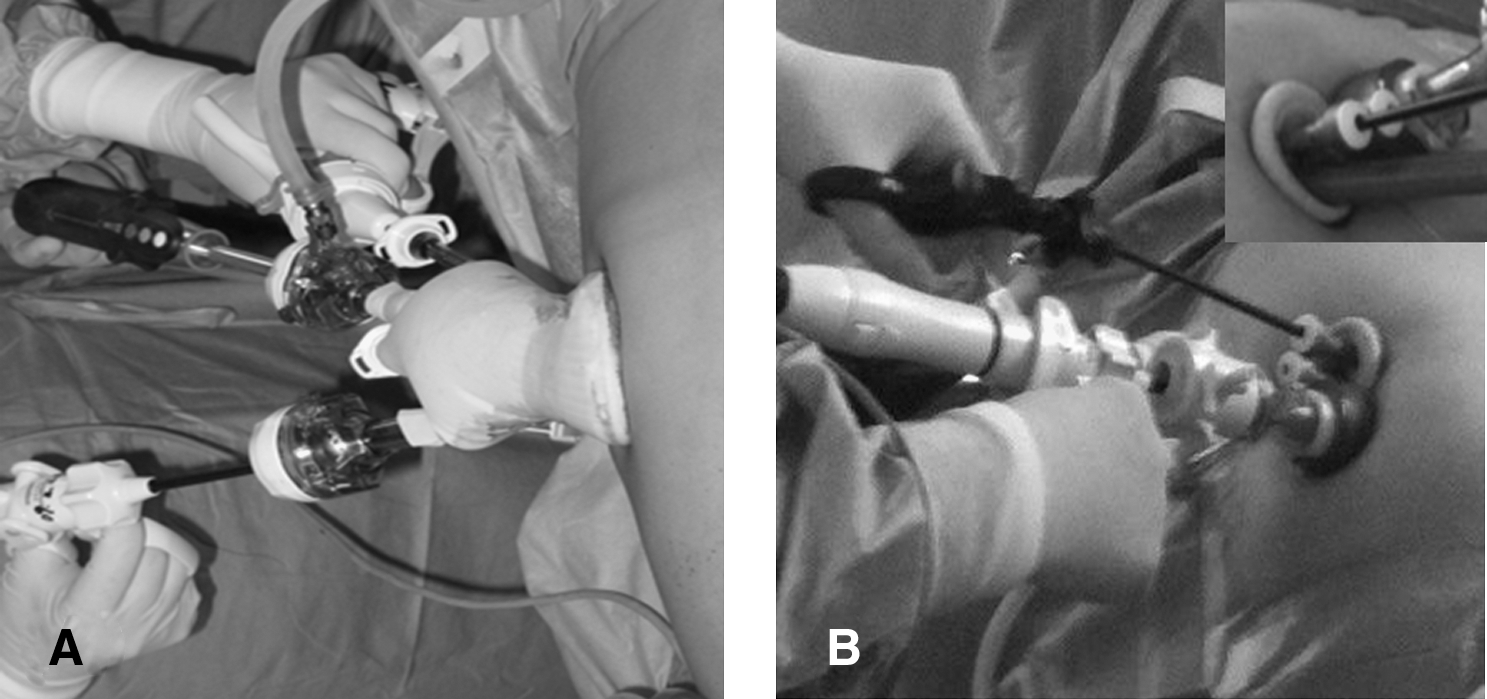
Single-port device. (
After carbon dioxide insufflation to maintain an intraperitoneal pressure of 14 mm Hg, a 30-degree, 10-mm laparoscope (EndoEye, Olympus Optical, Tokyo, Japan) was inserted into the peritoneal cavity. The operation was performed with standard 5-mm laparoscopic instruments, ultrasonic scissors (SonoSurg, Olympus Optical, Tokyo, Japan), and 5-mm articulating instruments (Cambridge Endo, Framingham, MA) (Fig. 1).
The LESS procedure replicated the procedure used in conventional laparoscopic surgeries. The ureter was identified in the retroperitoneal fat medial to the psoas muscle and clamped with Hem-o-lok clips (Teleflex Medical, Research Triangle Park, NC). The gonadal vein was clamped in the same manner as the ureter. During cephalad dissection, lymphadenectomy that included para-aortic lymph nodes was performed. For the right nephrectomy, an articulating forceps was used for liver retraction during hilar dissection (Fig. 2). The renal artery was dissected circumferentially and secured with Hem-o-lok clips. The renal vein was treated with a 35-mm vascular Endo-GIA stapler (Ethicon EndoSurgery, Cincinnati, OH). To dissect the superior margin, the dissected kidney was retracted downward using grasping forceps. Dissection between the inferior border of the spleen or liver and the kidney was completed. After completion of nephrectomy, the specimen was removed, and a Jackson-Pratt drain was left in place and fixed through the periumbilical incision (Fig. 2).

Completion of the operation. (
Retrospective data collection that included operative results was performed, and the collected data were matched with those of conventional laparoscopic radical nephrectomy. We analyzed the data using the SPSS program version 13.0. For comparison of the two groups, Mann-Whitney U test and Fisher exact test were used.
Results
All cases of LESS surgery were completed successfully, without conversion to conventional laparoscopic or open surgery. The characteristics of the patients who underwent LESS radical nephrectomy (group 1) or conventional laparoscopic radical nephrectomy (group 2) are presented in Table 1. There was no significant difference between the two groups. Three (30%) patients in group 1 had a history of abdominal operations, including hysterectomy, cholecystecomy, and lung lobectomy.
Mann-Whitney U test.
Fisher exact test.
Group 1 = laparoendoscopic single-site radical nephrectomy; Group 2 = conventional laparoscopic nephrectomy; BMI = body mass index.
There were no significant differences in the operative results of the two groups (Table 2). The mean operative times of 127.7 ± 22.3 minutes and 126.1 ± 43.1 minutes were not different in the two groups. The mean estimated blood loss of group 1 was larger than that of group 2; however, there was no statistical difference (P = 0.65). Two (16.7%) patients in group 2 needed transfusions. The operative complication rates were 10% and 17% in groups 1 and 2, respectively (P = 0 .658). Two patients (10%) in group 1 experienced wound infections, and two patients (16.7%) in group 2 experienced wound infection and lymphocele. Postoperative pain control was achieved by patient-controlled analgesia with morphine 40 mg and ketorolac 150 mg for 2 days. Diclofenac injection was administered to one (10%) patient in group 1 and three (25%) patients in group 2. The mean times to postoperative initiation of ambulation and oral intake were different in the two groups. In addition, the mean lengths of hospital stay were not different in the two groups.
Mann-Whitney U test.
Fisher exact test.
Group 1 = laparoendoscopic single-site radical nephrectomy; Group 2 = conventional laparoscopic nephrectomy.
There was no difference in the mean tumor sizes of groups 1 and 2 (Table 3). The pathologic results showed 8 cases of clear-cell type renal-cell carcinoma (RCC), 1 case of papillary type RCC, and 1 case of angiomyolipoma in group 1, and 10 cases of clear-cell type RCC, 1 case of papillary type RCC, and 1 case of collecting-duct type RCC in group 2. The surgical margins in all cases were negative.
Mann-Whitney U test.
Group 1 = laparoendoscopic single-site radical nephrectomy; Group 2 = conventional laparoscopic nephrectomy; RCC = renal-cell carcinoma; AML = angiomyolipoma.
Discussion
Laparoscopic radical nephrectomy offers significant advantages over open surgery as a less invasive surgery and has become a standard treatment for patients with localized renal tumor. 1 –5,12 Laparoscopic surgery has advanced to a minimally invasive approach to decrease operative morbidity while maintaining oncologic principles. To this end, laparoscopic surgery using a single incision and multi lumen port has been introduced. 9 Single-incision laparoscopic surgery was named laparoendoscopic single-site (LESS) surgery after a consensus in Cleveland. 13 LESS surgery yields superior cosmetic results and faster recovery than standard laparoscopic surgery. 8
Since Raman and colleagues 9,10 reported the first LESS nephrectomy in a porcine model and in human subjects, successful cases of initial LESS radical nephrectomy and partial nephrectomy for renal tumors have been reported. 11,14 Large series of LESS radical nephrectomy and comparative studies with conventional laparoscopy, however, have been rarely reported. Rais-Bahrami and coworkers 15 presented their initial experience of LESS renal surgery. They performed transperitoneal LESS radical nephrectomy in two patients using two 5-mm ports and a 12-mm port within the umbilicus, along with a 5-mm flexible-tip laparoscope (LTF series, Olympus Surgical, Orangeburg, NY) and flexible working instruments (RealHand, Novare Surgical System In., Cupertino, CA). The umbilical incision was extended for specimen extraction. The mean operative time was 124 minutes, and mean estimated blood loss was 125 mL.
Stolzenburg and colleagues 16 presented eight cases of LESS radical nephrectomy for renal tumors. They performed the transperitoneal approach with a transumbilical incision and used a TriPort (Advanced Surgical Concepts, Dublin, Ireland), which had three channels (a 12-mm and two 5-mm channels), and a RealHand roticulating forceps (Novare Surgical System In., Cupertino, CA). The median operative time was 141 minutes, and the median blood loss was 103 mL. The incision length was 3 to 6 cm. They suggested that LESS surgery was a feasible and safe approach in patients with low body mass index and early-stage tumor. Raman and associates 10 presented a comparative study of 11 cases of LESS nephrectomies including 6 cases of radical nephrectomy and 22 cases of conventional laparoscopic nephrectomy. They used three trocars in a periumbilical skin incision for LESS nephrectomy. Although the median operative time was 122 minutes in the LESS group as well as in the conventional laparoscopy group, the estimated blood loss was lower in the LESS group (20 mL).
Our experience with LESS radical nephrectomy showed that the operative results, including operative time, blood loss, and hospital stay, were comparable to those of conventional laparoscopy. Our LESS technique has distinguishing operative features. We used a 30-degree, 10-mm laparoscope, EndoEye, with an integrated coaxial camera head and a light cable to provide high-definition images without changing illumination in the bleeding field, which had a 5-mm laparoscope. Although we used a 5-mm laparoscope for LESS renal cyst excision, pyeloplasty, and adrenalectomy, we preferred a 10-mm laparoscope for nephrectomy. An articulating instrument of laparoscopic forceps (Cambridge Endo) is useful for liver retraction during right nephrectomy. When the liver is lifted by the curved portion of the instrument, the tip portion is able to grasp and dissect the tissue. Manipulation of the articulating instrument, however, is difficult and it may be out of the surgeon's range of vision.
For single-site devices, we initially used a homemade device, because single-port devices were not commercially available in Korea at that time. 17 This device had four channels. A 12-mm trocar for the right hand of the operator was used for the ultrasonic scissors or the Endo GIA staplers. A 5-mm trocar for the assistant was used for aspiration and irrigation, or for the retractor. An 11-mm trocar for the camera holder was used for the 10-mm laparoscope (EndoEye). Another 5-mm trocar for the left hand of the operator was used for the articulating instruments. Although it took time to make the device and insert it into the peritoneal cavity, and it could be torn during insertion of the instrument, the device itself was developed at a low cost and provided a broad range of movement because of high flexibility.
For the recent cases, we used a commercially available device, the SILS port, which has three channels (a 12-mm and two 5-mm channels). The 12-mm trocar was used for the 10-mm laparoscope. The two 5-mm trocars were used for the left hand of the operator and the assistant. A 12-mm balloon trocar (Applied Medical, Rancho Santa Margarita, CA) for the right hand of the operator was added to allow use of Endo-GIA staplers. A fascial suture was made between the SILS port and the 12-mm balloon trocar to prevent CO2 leakage.
We have presented limited data that were obtained from preliminary experiences. The operative data are comparable to those of conventional laparoscopy, and the LESS surgery provides cosmetic advantages. The numbers of cases, however, are too small to clearly elucidate statistical P values. The LESS radical nephrectomy may provide an alternative to standard laparoscopic radical nephrectomy for renal tumors. The procedure requires further development of the surgical instruments and operative techniques, however.
Conclusion
Our experience with a limited number of cases shows that LESS radical nephrectomy for renal tumors is technically feasible. Two types of single-port devices, a homemade port and a SILS port, were useful and safe. The operative results are comparable to those of conventional laparoscopic surgery. Instrument development and advanced laparoscopic skills are necessary, however, for the completion of the operation. Long-term follow-up results are also needed to assess the cancer control effect.
Footnotes
Acknowledgment
This article was supported by Wonkwang University in 2010.
Disclosure Statement
No competing financial interests exist.