
Abstract
Growing evidence supports the use of nephron-sparing techniques for the management of appropriately selected renal masses up to 7 cm. Compared with the surgical standard of open partial nephrectomy, minimally invasive approaches have demonstrated equivalent cancer control with reduced patient morbidity. Robot assistance has the potential to provide patients and physicians greater access to minimally invasive nephron-sparing surgery. We describe a robot-assisted retroperitoneal approach for the management of posterior renal masses. Our early results suggest reduced perioperative morbidity with the ability to manage more complex tumors.
Introduction
Laparoscopic partial nephrectomy demonstrates equivalent cancer control and improved convalescence compared with open partial nephrectomy. 4 Robot-assisted partial nephrectomy may make minimally invasive NSS more accessible to surgeons by facilitating intracorporeal suturing and knot tying. Based on our experience with laparoscopic retroperitoneal partial nephrectomy, we developed an approach to robot-assisted retroperitoneal partial nephrectomy (RRPN) that leverages the advantages of both a minimally invasive extraperitoneal approach and the robotic platform for intracorporeal renorrhaphy. Others have described similar techniques. The versatility of being able to perform a transperitoneal or retroperitoneal approach allows the surgeon to tailor the surgical procedure to the tumor characteristics.
Technique
Patient selection
Based on previously published work, 5 we select patients with posterior tumors that were located in the interpolar area or lower pole. For patients with upper-pole tumors, we favor either a transperitoneal laparoscopic or robotic approach. Although morbid obesity may obscure landmarks, is not a contraindication for RRPN. In these patients, the flank position and elevation of the kidney rest may aid in identification of the tip of the 11th and 12th ribs, anterior superior iliac spine, and costovertebral angle to aid in port placement. Patients with previous intra-abdominal surgery are also well-suited for this approach.
Patient positioning (Fig. 1)
Normal preoperative preparations are undertaken. Patients are placed in the full flank position on a beanbag with the anterior superior iliac spine positioned over the elevated kidney rest and the umbilicus positioned over the break in the maximally flexed table. The anterior arm is positioned on an armrest that is tilted toward the head as much as possible. The patient is secured to the table with a beanbag and cloth tape.
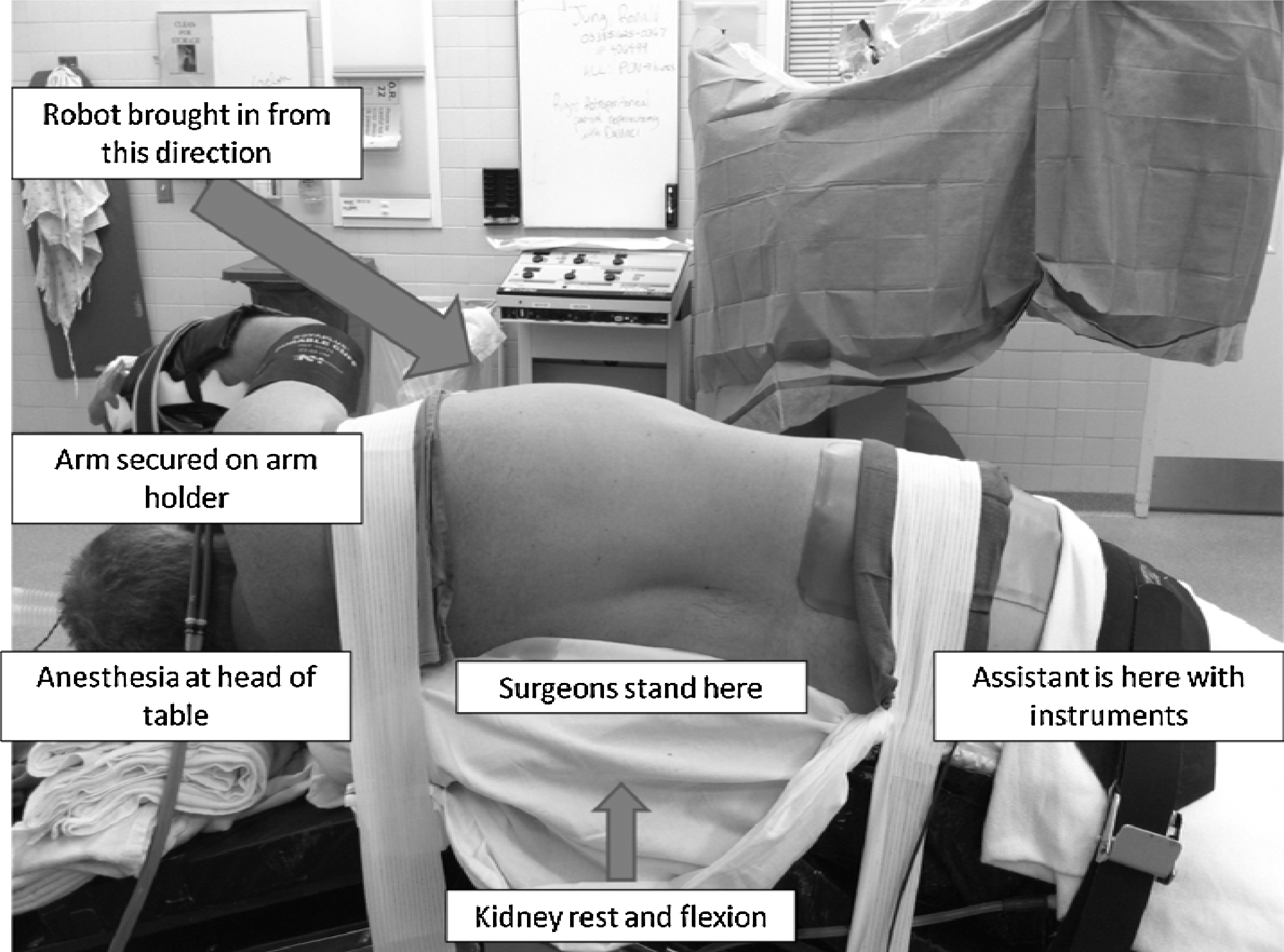
Patient positioning and room setup.
Initiation of the procedure (Fig. 2)
The patient is prepped and draped in the usual sterile fashion. A 2-cm incision is made below the tip of the 12th rib and extended through the fascia. The retroperitoneum is accessed with a tonsil clamp, and the space is bluntly dilated. It is important to go through the thoracolumbar fascia or this will need to be incised once the initial ports are placed to visualize the kidney. A 12-mm balloon dilating trocar is passed and aimed posterior toward the ipsilateral shoulder and inflated under direct vision using a 0-degree lens of a standard laparoscope and camera to create the working space. The dilator is removed and replaced with a conventional 12-mm trocar wrapped with petroleum gauze to avoid air leak. A purse-string suture is placed around the skin to also aid in reducing air leak. We switch to a conventional trocar because we have found the robotic camera sticks to the valve in the balloon dilator port, making it difficult to remove to clean if needed.

An 8-mm robotic port is placed under direct vision at the 12th costovertebral angle. Using blunt dissection (generally with a laparoscopic Kittner), the peritoneum is then swept medially to create space for a medial 8-mm robotic trocar that is placed two fingerbreadths below the level of the 11th rib. Two assistant ports (5 mm and 12 mm) are placed on either side of the anterior superior iliac spine. The table is angled 45 degrees, and the da Vinci® robotic surgical system (Intuitive Surgical, Sunnyvale, CA) is docked from the patient's anterior side approaching cephalad (Fig. 1). We have used both the S and Si system without difficulty but have not used the original standard system for this procedure. We have not used the third arm because of space limitations.
Identification of the hilum and tumor (video)
A 30-degree upward pointing lens is used for the procedure. Depending on visualization, a 0-degree lens can be used. We think, however, that the 30-degree upward pointing lens positions the camera to allow the assistant more space to work at the bedside, improving the ability to assist. Using the robotic scissors and bipolar grasper, the hilum is identified in line with the 8-mm costovertebral port. The artery and vein are isolated to allow bulldog placement. We then incise the Gerota fascia and dissect the mass free from its attachments to the surrounding perinephric fat, with the exception of a cap of fat overlying the tumor. Intraoperative ultrasonography is performed to identify the edges of the tumor as well as the depth of penetration. The capsule surrounding the tumor is scored with electrocautery.
Tumor resection and renorrhaphy (video)
Ten minutes before resection, we ask the anesthesiologists to administer 12.5 g of mannitol. The hilum is clamped using laparoscopic bulldog clamps. We prefer bulldogs over a Satinsky clamp because this avoids introducing an additional port into a tight working space. In addition, the bulldog eliminates the risk that the vascular clamp could be inadvertently bumped by the robotic or bedside surgeon. An athermal technique is used to resect the tumor. The tumor is placed in an endocatch bag, and a biopsy of the base is sent for frozen section. The argon beam is used to coagulate the edges of the resection. In a running fashion, 4-0 and 2-0 absorbable suture is used to close the collecting system and the renal sinus, respectively. Sewing can be expedited with the aid of absorbable suture clips (Lapra Ty clips, Ethicon Endo-surgery, Inc, Cincinnati, OH) placed on the cut edge of the renal parenchyma or nonabsorbable suture clips when the suture is placed through the capsule (Hem-o-lok clips, Teleflex Medical, Research Triangle Park, NC). Early unclamping can be considered at this point.
Our routine is to place a rolled nitrocellulose bolster with two preplaced 0-absorbable sutures on CT-1 needles, passed inside-out of the resection bed through the capsule, secured in place using Hem-o-lok clips, and tightened by sliding the clip against the capsule. 6 Additional premade 0-absorbable sutures on a CT-1 needle with a Hem-o-lok secured at one end can be used to further secure the bolster into place. We often use a hemostatic agent and an additional sheet of nitrocellulose to secure hemostasis. The bulldog clamps are then removed (if not already done), and an additional 12.5 g of mannitol is administered. The Gerota fascia can be reapproximated over the defect using suture or clips. The insufflation pressure is decreased to 5 mm Hg to inspect for bleeding.
Procedure completion
The robot is undocked and a 30-degree conventional laparoscope that was used at the beginning to create the retroperitoneal space is used to facilitate placement of a 10F round drain in cases where the collecting system or sinus was entered. The endocatch bag is removed through the camera port, extending the incision as necessary to remove the tumor and overlying fat intact. Depending on the size of the fascial defect, a Carter-Thomason device with a 0-absorbable PGA suture or a running 0-absorbable PGA suture on a UR-6 needle can be used to close this incision. The incisions are irrigated and the skin closed with subcuticular suture. Dressings are placed, and the patient is awoken and taken to the recovery room.
Post-operative care
The patient's diet is advanced as tolerated. Antibiotics are continued for 24 hours. Patients are encouraged to ambulate the day after surgery. The bladder catheter is removed the following morning and, if a drain has been left in place, it is removed if the output remains low in the subsequent 4 hours. The patient can then be discharged home. The patient is seen 2 weeks after surgery, and subsequent oncologic surveillance is guided by pathologic results.
Role of the bedside surgeon
The bedside surgeon is crucial in the successful completion of the procedure. After the robot is docked into position, the assistant aids in cephalad retraction with a laparoscopic Kittner and exposure of the hilum with the laparoscopic suction. After adequate mobilization of the hilum, the assistant aids in identifying the tumor by continued assistance with retraction. To evaluate the full extent of the tumor, the assistant must be comfortable in the use of laparoscopic ultrasound. The assistant is also responsible for safely placing the bulldog clamps preceding resection of the tumor and removing the clamps at the completion of the resection and reconstruction. During tumor resection and management of bleeding from the tumor bed, the assistant must be confident in providing adequate exposure and suction; replacing robotic instruments; placing suture, bolster material, and hemostatic agents efficiently; and cutting and removing suture. We have found it helpful to discuss the anticipated steps in detail before clamping the kidney and reviewing the success of the operation at the end of the surgery to identify areas of quality improvement. While these are the same roles as in the transperitoneal approach, the smaller work space necessitates more intentional movements by the assistant and better coordination.
Equipment
Table 1 describes the equipment used.
Role in Urologic Practice
From January 9, 2009 through June 21, 2010 we have performed 16 RRPN. Table 2 summarizes the perioperative results of our patients undergoing RRPN. This represents the collective experience of four surgeons with experience in laparoscopic, robot-assisted, and open partial nephrectomy. We typically operated with two experienced surgeons early in our experience. Nephrometry scores 7 demonstrate that most of these tumors were moderately complex with two tumors abutting the renal hilum. All patients underwent three-dimensional axial imaging within 3 months of surgery. In the majority of cases, we clamped only the renal artery. Postoperatively, a drain was placed in most patients and was removed after the Foley catheter on the day of discharge.
Figure 3 demonstrates the progressive decrease in operative time and ischemia time during the 18-month period. Two conversions occurred: One to a transperitoneal robotic approach because of peritoneotomy and one to conventional laparoscopy because of difficulty with positioning of the robotic arms and camera during dissection of the tumor. A total of six postoperative complications occurred. One patient presented to the emergency department with pain, which, after extensive evaluation with CT, laboratory studies, and chest radiography, was found to be musculoskeletal and was managed with oral pain medication. Pneumonia developed in two patients; it was managed with oral antibiotics (one patient was admitted to the hospital overnight). Urinary retention developed in one patient; tamsulosin was initiated, and the catheter was removed 1 week after surgery. Atrial fibrillation developed postoperatively in one patient who had a history of this condition; he was treated with diltiazem by his cardiologist. Finally, one patient presented to clinic 1 week after the surgery with increasing flank pain. Renal ultrasonography demonstrated a 4 × 3 cm fluid collection adjacent to the bolster that was managed with retrograde stent placement in the operating room. This resolved, and the patient had the stent removed 3 weeks after surgery. There was no postoperative hemorrhage necessitating blood transfusion, and no episodes of acute renal failure.

Changes in operative parameters over time.
The critical portion of this procedure is sufficient development of the retroperitoneal space without entry into the peritoneum and adequate port placement. Although a 5-mm intraperitoneal trocar can be used to vent the peritoneum, peritoneal violation increases the difficulty of the procedure, necessitating cephalad retraction by the assistant. In addition, poor port placement may make tumor dissection more challenging. If this occurs, conversion to a conventional laparoscopic approach may be necessary.
RRPN represents a useful technique in the armamentarium of tools to manage small renal masses. This technique requires comfort with the laparoscopic retroperitoneal and robotic approaches. Early on, assistance of an experienced surgeon is essential. Our initial data suggest that, in appropriately selected patients, perioperative outcomes are excellent using this technique.
Footnotes
Disclosure Statement
Dr. Jeffrey S. Montgomery is a proctor for Intuitive Surgical. Dr. Alon Z. Weizer is a proctor for Intuitive Surgical and a consultant for Teleflex Medical. The other authors have no conflicts of interest to declare.
Abbreviations Used
*
A video demonstrating this technique is available at