
Abstract
Purpose:
We present a simple and easy to apply surgical approach for partial nephrectomy that combines open and laparoscopic surgery allowing for vascular control in technically challenging renal tumors and for reduction of ischemia time.
Patients and Methods:
Five patients underwent partial nephrectomy using the combined laparoscopic/open approach. After complete laparoscopic mobilization of the kidney and securing of the renal vessels, the kidney is transferred extracorporally through a small pararectal incision for tumor resection.
Results:
The technique was feasible in all cases, with no conversion needed. In three cases, no clamping of the renal artery was necessary. The mean operative time was 219 minutes (range 195–260 min). Pathologic examination revealed no malignancy in two (40%) cases. The estimated median blood loss was 500 mL (range 250–1000 mL). Renal function decreased from 84.9 mL/min (range 48.0–89.0 mL/min) to 78.8 mL/min (range 52.6–82.6 mL/min). Mean hospital stay was 5 days (range 3–14 d).
Conclusion:
Based on our initial experience, we propose a feasible surgical option for minimally invasive partial nephrectomy, which is, in particular, suitable for technically challenging renal tumors (endophytic and central tumors, large tumors, tumors in solitary kidneys).
Introduction
Surgical approaches such as laparoscopy have led to reduced invasiveness and morbidity. PN can be performed laparoscopically, although advanced skills are necessary. 7 Further developments represent single-port laparoscopic approaches and the incorporation of robot-assisted surgery. 8,9 Critical points of these approaches include hemostasis and warm ischemia time.
We investigated a simple and novel minimally invasive approach for PN that combines open and laparoscopic approaches to improve hemostasis and ischemia time from an optimal vascular control. From the surgical point of view, this technique is suitable in particular for technically challenging tumors, such as large tumors, endophytic or centrally located tumors, or tumors in solitary kidneys, in which maintenance of renal function is of paramount importance.
Patients and Methods
Since September 2008, a prospective analysis of the initial five patients undergoing PN by an open/laparoscopic approach was performed. Among them, four (80%) patients had a normal contralateral kidney (elective indication). One patient underwent contralateral radical nephrectomy because of renal-cell carcinoma 65 months before surgery (imperative indication). Patient demographics, perioperative data, and final pathologic outcomes were evaluated for all patients (Table 1). Among them, three patients were men. Mean age was 62.1 years (range 41.9–68.6 y).
BMI=body mass index; EBL=estimated blood loss; (d)=days.
The renal masses were categorized as follows: 4.8 cm endophytic tumor of the right middle pole adjacent to the collecting system (patient A), 2.0 cm endophytic tumor of the left lower pole (patient B), 1.4 cm endophytic tumor of the left lower pole (patient C), 3.3 cm centrally located endophytic tumor adjacent to the collecting system on the right side (patient D), and 5.8 cm exophytic right lower pole tumor adjacent to the collecting system (patient E). Differential indication for the present technique was an endophytic (patients A–C) or central (patient D) location of the tumor as well as involvement of the collecting system (patients A, D, E).
For laparoscopic mobilization of the kidney, a conventional transperitoneal approach was performed. The colon was dissected off the Gerota fascia and retracted medially. The Gerota fascia was incised and the kidney defatted at an adequate distance from the kidney tumor. After opening the Gerota fascia, the kidney was completely mobilized, leaving the perirenal fat attached to the tumor. The entire hilum was thoroughly mobilized, and the renal artery and vein were secured by vessel loops (Fig. 1). After laparoscopic mobilization of the kidney, a pararectal incision of approximately 8 cm was performed, which is usually used for laparoscopic nephrectomy or laparoscopic donor nephrectomy. Using this incision, the kidney was transferred extracorporally while the renal vessels with loops stay intracorporally (Fig. 2).
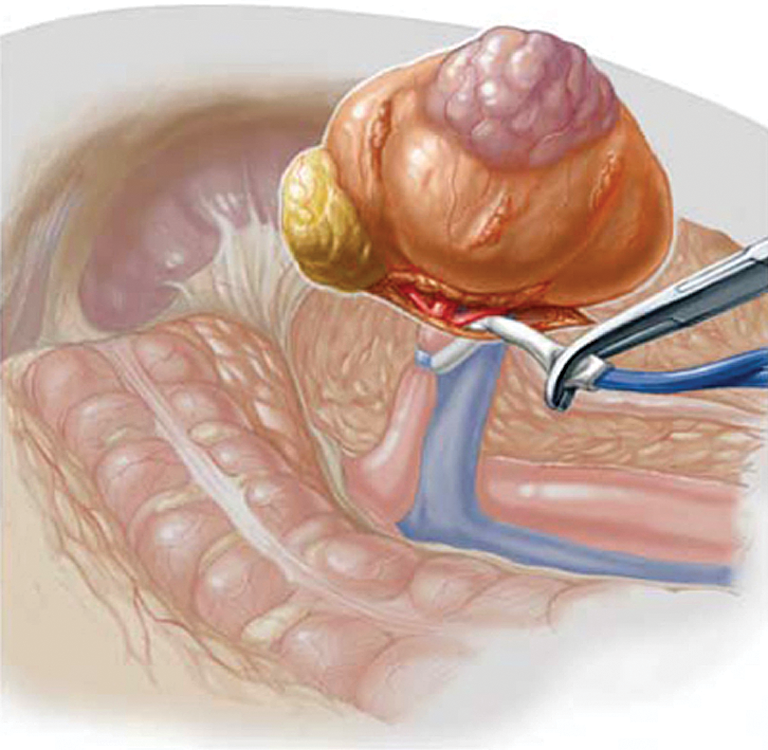
After conventional laparoscopic mobilization of the kidney leaving the perirenal fat attached to the tumor, the renal vessels are exposed and secured by vessel loops. Through pararectal incision, the kidney is exposed extracorporally for partial nephrectomy.

Photograph of the operation situs:
Clamping of the artery is usually not necessary for small peripheral tumors. Ten minutes before clamping the renal artery, 20 mg of furosemide and 100 mL mannitol (15%) were administered intravenously for renoprotection.
Open PN was performed conventionally. In brief, the fibrous renal capsule was incised at 2 to 4 mm from the tumor. The renal parenchyma was sharply and bluntly separated in the renal cortex and only bluntly in the medulla along the parallel structures of tubules and collecting ducts of the renal papillae. Small vessels were coagulated and large vessels were oversewn with 4/0 polyglycolic acid sutures. The removed tumor was sent for frozen section analysis of the central (tumor adherent) margins of resection. Additional random biopsy samples were taken from the resection bed of the preserved kidney to determine peripheral margins. An argon-beam laser was used for coagulation. The renal fibrous capsule was closed with a running monofilament mattress suture using 5/0 poly-p-dioxanone.
Data are given in median and range. Comparison of dependent variables was tested using the nonparametric Wilcoxon rank sum test. Statistical analysis was performed using the SPSS software package (Chicago, IL). Statistical significance was regarded at P<0.05.
Postoperative hemoglobin was assessed 48 hours postoperatively. Serum creatinine level was measured preoperatively, 1 day, 1 week, and 3 weeks after surgery. Glomerular filtration rate (GFR) was estimated according to the simplified Modification of Diet in Renal Disease formula 10 and estimated preoperatively and 3 months postoperatively. Statistical analysis was performed using the SPSS software package.
Results
A total of five patients undergoing combined open/laparoscopic PN were enrolled in our study. The mean operative time was 219 minutes (range 195–260 min). Cardiac infarction developed in one patient on the second day after surgery, and the patient was admitted to the intermediate care unit for 4 days. This patient was transfused with 3 units of packed red blood cells to put the hemoglobin level into supernormal values. The patient experienced a prolonged hospital course because of cardiovascular reasons and was discharged at day 14 after surgery. Apart from this patient, no perioperative morbidity was observed. Mean hospital stay was 5 days (range 3–14 d).
Pathologic examination revealed no malignancy (oncocytoma and myxoid regressively altered hemangioma) in two (40%) cases. In three (60%) patients, renal-cell carcinoma, which was found in the histopathologic analysis (two clear cell, one chromophobe), was completely resected with negative intraoperative surgical margins in frozen section analysis.
With respect to hemostasis (Table 1), the estimated median blood loss was 500 mL (range 250–1000 mL). Using the unclamp technique (n=3), average blood loss was 800 mL (range 400–1000 mL). Hemoglobin values baseline (Table 2) before surgery decreased from 13.5 g/dL (range 12.5 g/dL–15.9 g/dL) to 9.7 g/dL (range 7.5 g/dL–12.4 g/dL) 2 days after surgery (P<0.05).
Preop=preoperative; postop=postoperative; Hb=hemoglobin; GFR=glomerular filtration rate.
With respect to renal function, serum creatinine level was 0.89 mg/dL (range: 0.7–1.46 mg/dL) preoperatively compared with 0.94 mg/dL (range 0.73–1.35 mg/dL) 1 week after surgery (P<0.05 vs preoperatively) and 0.9 mg/dL (range 0.79–1.5mg/dL) 3 months after surgery (P<0.05 vs preoperatively). In three cases, clamping of the renal artery was not necessary. Renal function (Table 2) decreased from 84.9 mL/min (range 48.0–89.0 mL/min) to 78.8 mL/min (range 52.6–82.6 mL/min).
Discussion
With the advances in abdominal imaging, the incidence of small asymptomatic renal masses has increased. 11 PN is now regarded as the gold standard for therapy, showing similar oncologic outcomes compared with radical nephrectomy. 2,3
Laparoscopic PN is technically challenging and can be performed safely in experienced hands. The laparoscopic approach, however, has been associated with a higher rate of complications in large series compared with open PN. The approach has demonstrated oncologic equivalency to open surgery. 7,12 Laparoscopic PN offers an abbreviated hospital stay, shorter convalescence, and less pain compared with the open approach.
Major drawbacks for open PN, but in particular for laparoscopic PN, include achieving adequate hemostasis 13 and warm ischemia time during clamping of the artery leading to renal impairment from ischemia/reperfusion injury. Occasionally, exophytic small renal masses can be approached without hilar clamping in selected patients 14,15 or by use of thermal energy, such as GreenLight™ laser 16 or radiofrequency coagulation. 17 Although a higher blood loss is encountered, potential ischemic and vascular injury to the kidney is avoided. 18 –20
Renal function is maintained by PN by preserving renal parenchyma and protection from renal function deterioration. 4 The benefits of PN ascend beyond renal function preservation, protecting from a variety of related systemic morbidities such as cardiovascular disease, anemia, malnutrition, and neuropathy. Therefore, renal impairment after surgery for renal-cell cancer reduces quality of life 4 and predisposes to higher mortalitiy. 6,21
Technologic advancements have challenged minimally invasive surgery to further reduce patient morbidity. We present a feasible and easy-to-apply approach combining the laparoscopic with the open surgery approach, allowing for hilar vascular control, rapid resection of the tumor with low ischemia times whenever required and potential easy reconstruction of the collecting system. Generally, the resection is performed without clamping of the artery. The advantage of the described technique is the option to rapidly interrupt the circulation whenever required. This approach is in particular appropriate, when conventional laparoscopic surgery is challenging such as for tumors in solitary kidneys, as well as for central or endophytic tumors, and for upper pole tumors. In particular, central tumors are challenging because they require deeper resection, necessitating control of larger segmental vessels and closure of the collecting system. Upper pole tumors reduce maneuverability and visibility for the surgeon. Exophytic tumors in general do not require clamping of the renal artery since hilar clamping has the potential to cause both renal vascular and ischemic injury to the kidney. As for challenging tumors, warm ischemia time can be reduced by using this approach.
Conclusion
Based on our initial experience, we propose a feasible surgical option for minimal-invasive PN. This technique is suitable for advanced PN in difficult cases such as large tumors, endophytic or centrally located tumors or tumor in solitary kidneys, in which maintenance of renal function is of utmost importance.
Footnotes
Disclosure Statement
No competing financial interests exist.