
Abstract
Purpose:
The study focused on the use of balloon or telescopic/serial dilation methods in percutaneous nephrolithotomy (PCNL) in the Global PCNL Study.
Patients and Methods:
Centers worldwide provided data from consecutive patients who were treated with PCNL during a 1-year period. Tract dilation was performed using a balloon or telescopic/serial dilator. Patient characteristics, perioperative complications, and treatment outcomes were assessed by the treating physician. Postoperative complications were graded according to the modified Clavien grading system.
Results:
A total of 5537 eligible patients were entered in the database from November 2007 to December 2009, including 2277 (41.1%) who received balloon dilation and 3260 (58.9%) who received telescopic/serial dilation. The predominant method used was telescopic/serial dilation in Asia (94.7%) and South America (98.0%), and balloon dilation in North America (82.6%). In Europe, the rates of balloon (50.7%) and telescopic/serial (49.3%) dilation procedures were similar. The rates of bleeding (9.4% vs 6.7%), blood transfusions (7.0% vs 4.9%), and drop in mean hematocrit level (4.5% vs 2.5%) were higher in the balloon vs telescopic/serial dilator group. Clavien scores II and IIIA were slightly in favor of the telescopic/serial dilator group. Median operative time was longer in the balloon dilation group (94.0 min vs 60.0 min).
Conclusions:
The Global PCNL Study has identified differences in the method of dilation used between centers in Asia, Europe, and the United States. In the balloon dilation group, a total longer operative time and higher bleeding and transfusion rates were observed. The differences in outcome may be influenced by patient heterogeneity, including previous anticoagulation therapy or surgical procedures, in addition to the number of stones treated and rate of staghorn calculi, which were all higher in the balloon group.
Introduction
PCNL needs a large percutaneous tract into the kidney to enable the passage of the nephroscope, and tract dilation is a major procedure, which can be particularly complicated in certain patients, such as those with scar tissue from previous procedures. 6,7 There are three established dilation methods, and although the techniques were pioneered for nephrostomy tract dilation in the 1980s, they remain widely used today: These are the Amplatz polyurethane serial dilators, metallic telescopic dilators as described by Alken, and balloon dilators. 8 –11
Balloon dilation is reported to be associated with shorter operative times, reduced fluoroscopic exposure, and lower rates of bleeding complications compared with multi-incremental methods. 12 –15 The balloon technique, however, uses disposable instruments and is considered expensive compared with telescopic dilation, which is performed with reusable instruments. 15 More recently, the use of single-step dilation with an Amplatz dilator performed over a metallic telescopic dilator (“one shot”) has been shown to provide favorable morbidity while reducing fluoroscopic exposure compared with traditional telescopic dilation. 13,16
PCNL is an area of special interest to the Clinical Research Office of the Endourological Society (CROES). As such, CROES established the PCNL Global Study, which comprised a database of information on more than 5800 patients from 96 centers in 26 counties who were treated by PCNL. The primary objective of the PCNL Global Study was to assess stone-free rates, while the secondary aims were to assess perioperative morbidity and to identify risk factors for poor outcomes. 17 Comprehensive analyses of the Global PCNL dataset are ongoing. 18
In this analysis, we evaluated patient characteristics and outcomes in PCNL using balloon or telescopic/serial tract dilation and attempted to investigate factors that influenced the choice of dilation method worldwide. This article is the second in the series that will be presented from the PCNL Global Study. The first publication from the study focused on indications, complications, and outcomes in the total study population. 19
Patients and Methods
Data collection
A steering committee of global experts in PCNL treatment was invited by the CROES council to direct the study. The target was to enroll 100 centers worldwide, including smaller centers, which performed <25 procedures a year, to “high volume” centers, which performed >100 procedures annually. Centers invited to participate were members of the Endourological Society or were considered to have high expertise in the surgical field.
Electronic databases were made available to participating centers, and data were sent encrypted to the headquarters of CROES. Institutional Review Board approval was obtained at participating centers, if needed. The lead investigator at each center coordinated data collection and submitted regular updates to the central database. Each center provided data for consecutive PCNL patients for a study period of 1 year starting from the date of inclusion of the first patient.
Patients and procedures
Patients who underwent PCNL for the primary or secondary treatment of kidney stone indications during the study period were eligible for inclusion; there were no specific exclusion criteria. PCNL procedures were performed according to local clinical guidelines and practices; detailed methodology is provided in a previous publication. 19 PCNL involved the use of ultrasonograpphy and/or radiography in combination with fluoroscopy to locate the upper tract. Nephrostomy tract dilation was performed using balloon dilation, metal telescopic dilation, or Amplatz serial dilation. The aim of tract dilation was to create a reliable tract for the insertion of an Amplatz sheath down which the nephroscope was passed. After puncture of the collecting system under fluoroscopic guidance, a stiff guidewire was inserted down the ureter. In balloon dilation, the dilator was inserted with the distal end placed in the collecting system as close to the stone as possible. The balloon was then inflated using a pressure inflation device until all wasting in the balloon had disappeared. The Amplatz sheath was inserted over the balloon, then the balloon was deflated and removed. 11 For metallic telescopic dilators, each dilator was inserted over the previous making the tract progressively larger; the largest dilator was typically 30F, over which the Amplatz sheath was placed before removing the dilators. 10 Amplatz dilation involved the serial passage of plastic fascial dilators from 10F to 30F; the Amplatz sheath was passed over the final dilator, and the dilator was again removed. 8
The severity of bleeding was based on the clinical judgment of the treating physician, and blood transfusions were performed according to local practice guidelines. Patient characteristics, perioperative complications, and treatment outcomes were assessed by the treating physician. At participating centers, Institutional Review Board approval was obtained, if required; otherwise, the lead investigator was responsible for ensuring the quality of clinical data collected.
Data analyses
The similarities between telescopic and serial dilator methodologies led to the pooling of outcome from patients who were treated with either dilator. Patients were grouped according to the tract dilation method used: Balloon dilation or telescopic/serial dilation. The variables of interest were the global distribution and demography of the use of tract dilation methods, patient characteristics, complication rates, operative time, and length of hospital stay. The study centers were classified according to the volume of procedures performed in the study year: Low <25; medium 25–100; high >100. The modified Clavien grading system was used to standardize the classification of the overall perioperative morbidity and to allow for a comparison between groups. 20 –22 Body mass index (BMI) was assessed according to World Health Organization (WHO) classifications. The data were analyzed with SPSS version 16.0. All data are descriptive and based on frequencies.
Results
The first patient was entered into the database on November 2007 and the database closed in December 2009. The Global PCNL database included 5803 patients, of whom 266 patients were excluded from the analysis because no information about the method of dilation was available. The remaining 5537 patients included 2277 (41.1%) in the balloon dilation group and 3260 (58.9%) in the telescopic/serial dilation group.
Study centers
Among the 96 centers represented in the Global PCNL database, 28 centers used balloon dilators only, 25 centers used telescopic/serial only, and 43 centers used telescopic, serial, or balloon dilators. Table 1 and Figure 1 show the methods of dilation used according to continent and by country. Countries that provided the largest number of patients were India (n = 1012), Turkey (n = 632), Romania (n = 624), and the United States (n = 580). Argentina, China, Greece, and Spain each provided data from more than 200 patients.
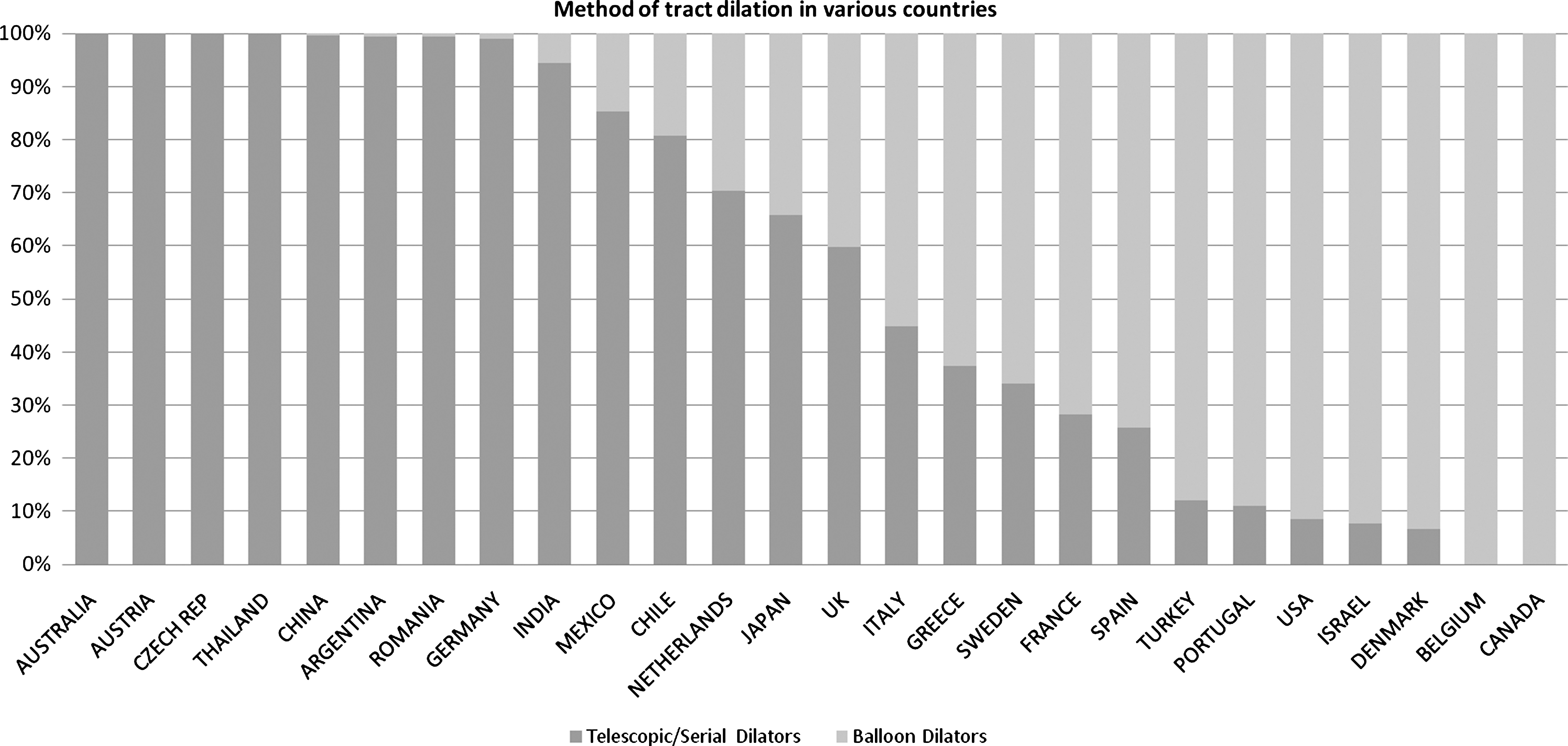
Frequency of balloon dilation and telescopic/serial dilation over 1 year by country.
Telescopic/serial dilation was the predominant method in Asia (1271/1342; 94.7%) and South America (337/344; 98.0%), while balloon dilation was the major method used in North America (650/787; 82.6%). In Europe, neither balloon (1549/3055; 50.7%) nor telescopic/serial (1506/3055; 49.3%) dilation predominated. By country, telescopic/serial dilatation was used in >90% of patients in Argentina, Australia, Austria, China, Czech Republic, Germany, India, Romania, and Thailand. Balloon dilation was used in >90% of patients in Belgium, Canada, Denmark, Israel, and the United States.
In high-volume centers (>100 procedures in the study year), the frequency of telescopic/serial dilation was higher than balloon dilation at 67.2% and 32.8%, respectively (Table 2). The techniques were used with similar frequency in low- and medium-volume centers.
Patient characteristics
Preoperative patient characteristics are shown in Table 3. The mean age of patients in the balloon and telescopic/serial groups was 50.8 years and 48.8 years, respectively. The median BMI in the telescopic/serial and balloon groups was 25.8 kg/m2 and 26.9 kg/m2, respectively. The use of preoperative anticoagulation therapy was more common in the balloon vs telescopic/serial group at 8.5% and 3.5%, respectively. There was a trend toward a greater proportion of patients with previous procedures in the balloon group than the telescopic/serial group, particularly for previous SWL at 29.0% and 16.2%, respectively. Staghorn stones were more frequent in the balloon vs telescopic/serial group at 31.0% and 25.3%, respectively.
ASA = American Society of Anesthesiologists; PCNL = percutaneous nephrolithotomy; SWL = shockwave lithotripsy; URS = ureteroscopy.
Preoperative BMI by continent and by WHO classification in the dilator groups is shown in Tables 4 and 5, respectively. BMI was similar for the dilation methods for each continent. According to the WHO classification, obesity was more common in the balloon group at 27.6% compared with the telescopic/serial group at 16.7%.
BMI = body mass index.
Outcomes
The main variables of interest in regard to postoperative outcome are shown in Table 6. For complications, such as bleeding, blood transfusions, and drop in hematocrit, the mean rates were numerically higher in the balloon vs telescopic/serial group. The median range of the Clavien score (II and IIIA) were slightly in favor of telescopic/serial dilators, while the serious complications (≥IIIB) were in the same range for both balloon and telescopic/serial dilators. Median operative time favored telescopic/serial dilation, but duration of hospital stay was the same for both groups. The mean rate of fever favored the balloon group.
In regard to staghorn stones (data not shown), very little difference between dilation methods was noted in the rates of complications with the exception of a higher mean rate of bleeding with balloon dilation (12.3% vs 8.5%) as well as a longer mean operative time (120 min vs 85 min).
Discussion
During a study period of 1 year, a total of 5803 patients from 96 centers worldwide were included in the Global PCNL database. As part of a series of analyses, in this study we assessed tract dilation in PCNL using balloon dilators compared with telescopic/serial dilators. Tract dilation was performed using a balloon dilator in 41.1% of procedures, and telescopic/serial dilation was used in 58.9% of procedures. More than 95% of procedures in Asia and South America involved telescopic/serial dilation, and in North America, balloon dilation was the major method used, with rates of 91.4% in the United States and 100% in Canada. Each technique was used with equal frequency in Europe. In countries such as the Czech Republic, India, Thailand, and Argentina, more than 95% of procedures involved telescopic/serial dilation, and in North America and countries such as Belgium and Israel, >90% of procedures involved balloon dilation. This would suggest that cost strongly influences the choice of procedure, and balloon dilation tends to be used if cost is not an issue. In some countries, however—for example, Chile and Spain—there was more than 20% use of each method, suggesting that a “real choice” had been made.
At high-volume centers at which more than 100 procedures were performed in 1 year, the rate of telescopic/serial dilation was 67.2% and balloon dilation was 32.8%, whereas in low- and medium-volume centers, there was no clear trend for either technique. In these centers, there was availability and experience with both techniques, which were applied depending on the case presented. For example, in a patient with a stone in the renal pelvis, a balloon might be used, and in the case of a staghorn stone, a telescopic/serial dilation might be used.
Metallic telescopic dilators typically cost $750 to $1000 with a further cost of sterilization of approximately $75. Serial dilators cost around $100 to $150, whereas balloon dilators typically cost around $200 to $400 and can only be used for one tract dilation. Prices may vary between different designs of dilators and different countries; however, to date, no studies have compared the direct and indirect costs associated with balloon and telescopic/serial methods.
There was a trend toward a greater proportion of patients with previous procedures in the balloon group than the telescopic/serial group, particularly for previous SWL. The explanation for this may be the distribution of balloon treatment in those countries where there are fewer economic restrictions and there is a wider choice of treatment options. For example, in the United States, urologists may be more liberal in recommending a SWL treatment, and if this fails, move on to PCNL. In “developing countries,” there may less access to SWL and with budget restrictions, the treating surgeon might move directly to PCNL. Moreover, an increasing number of colleagues are aware of the limited effectiveness of SWL and weigh this vs a more effective surgical approach. 23
Complications have been reported in about 83% of patients who undergo PCNL. and careful patient selection is needed. 6 Frequent complications include bleeding, extravasations, and fever; less common complications include septicemia and pleural injury. 6 Patient-related predictors of poor outcomes include staghorn stones, stone surface area, and previous procedures for kidney stones, while procedural-related risk factors include the number of tracts and the method of tract dilation. 7,24 Balloon dilation has been reported as having a better hematologic safety profile than Amplatz and metal telescopic dilation. 7,12,14 In a retrospective analysis of a large contemporary case series involving 200 cases, however, whereas balloon dilation reduced operative time and hospital stay compared with metal telescopic dilation, the two techniques had similar morbidity profiles. 15
The risk of bleeding complications may have influenced the choice of dilation method in the study as the rates of preoperative anticoagulation therapy use in the balloon dilation group was 8.5% compared with 3.7% for telescopic/serial dilation. There was also a trend toward the increased use of balloon vs telescopic/serial dilation among patients with previous procedures, particularly SWL, at 29.0% and 16.2%, respectively. Preoperative physical status may have also influenced choice, with a trend toward increasing use of balloon dilation vs telescopic/serial dilation with increasing American Society of Anesthesiologists scores. Stone location did not differ greatly between the groups, although there was a numerically higher median stone load among patients in the balloon vs telescopic/serial dilation groups, and staghorn stones were slightly more frequent at 31.5% vs 25.3%, respectively. In the study, the rates of bleeding and of blood transfusions were numerically lower in the telescopic/serial dilator group at 6.6% and 4.0%, respectively, compared with the balloon dilator group at 9.4% and 7.0%, respectively.
It has been suggested that obesity increases the technical difficulty of PCNL, and this may increase the risk of complications. The influence of BMI on outcomes in PCNL is unclear, however, with some studies reporting a negative impact on complication rates 25 –28 and others reporting that BMI did not strongly influence outcomes. 29 –32 In a retrospective review of a large (n = 234) contemporary case series of patients who underwent PCNL with balloon dilation, BMI was not significantly correlated with stone-free rate, complication rate, hemorrhage, or length of hospital stay. 33 In the present study, we found that median BMIs were similar between groups at 26.9 mg/kg 2 and 25.8 mg/kg 2 for balloon and telescopic/serial dilation, respectively. According to the WHO classifications of BMI (ie, underweight, normal, overweight, obese), 27.6% of the balloon dilator group compared with 16.7% of the telescopic/serial dilator group were obese (BMI ≥30.0 kg/m2).
To our surprise, the data indicated that median operative time was longer in the balloon dilation group. We have no clear explanation for this. Actually, it is generally believed that the use of a balloon for dilation actually saves operative time. Maybe some of the centers already had a percutaneous tube or an established tract, thus facilitating the surgery and maybe even affecting the choice of dilation. Data on the presence of established tracts are not available, however, because they were not captured in the database. Moreover, the dilation time is only a small part of the total operative time and was not captured separately in the database. Obviously, in the balloon group, the rate of staghorn calculi was higher with a higher stone rate and thus needs more operative time to render patients stone free.
The observational nature of this study is a clear limitation. It is well recognized, however, that the integration of prospective database studies and clinical studies is needed for the advancement of surgical techniques. 34 Indeed, there are many obstacles to performing randomized controlled trials (RCTs) of surgical techniques, meaning that the quantity and quality of clinical research in surgery is limited, and general surgical practice is less likely to be based on RCT evidence than general medical practice. 34 –39 Therefore, in 2002, McCulloch and colleagues 34 proposed that “detailed prospective audit data collection is essential for surgical research.” Indeed, whereas prospective observational studies cannot replace well-designed clinical trials, and such trials are warranted in endourology, the Global PCNL Study is important for the advancement of surgical excellence in PCNL indications.
Conclusion
This analysis of the Global PCNL Study has shown that there were differences in the method of dilation used between centers in Asia, Europe, and the United States. In the balloon dilation group, total longer operative times and transfusion rates were observed. The differences in outcome may be influenced by patient heterogeneity, including previous anticoagulation therapy or surgical procedures, in addition to the number of stones treated and stone load, which were all higher in the balloon group. Last but not least, findings must be regarded with caution given the descriptive nature of the current work. Further analysis will identify the presence of potential independent risk factors.
Footnotes
Acknowledgment
The Global PCNL Study was supported by an unrestricted educational grant from Olympus.
Disclosure Statement
No competing financial interests exist.
Abbreviations Used
Appendix
| COUNTRY | PRINCIPAL INVESTIGATOR |
|---|---|
| GERMANY | ALKEN |
| SPAIN | AMON SESMERO |
| UNITED STATES | AVERCH |
| ITALY | BIANCHI |
| NETHERLANDS | BOELLAARD |
| ROMANIA | BOJA |
| AUSTRALIA | BOLTON |
| ROMANIA | BOTOCA |
| UNITED STATES | BREDA |
| UNITED KINGDOM | BUCHHOLZ |
| ROMANIA | BUCURAS |
| SPAIN | BUENO CHOMON |
| ITALY | CAUDA |
| ITALY | CELIA |
| ITALY | CORMIO |
| ITALY | CRISCI |
| ITALY | D'ADDESSI |
| ARGENTINA | DAELS |
| NETHERLANDS | DE LA ROSETTE |
| ITALY | DE LISA |
| ITALY | DE SIO |
| INDIA | DESAI |
| ISRAEL | DUVDEVANI |
| TURKEY | ERDOGRU |
| ITALY | FRATTINI |
| ITALY | GAROFALO |
| ROMENIA | GEAVLETE |
| ITALY | GIUSTI |
| INDIA | GOPALAKRISHNAN |
| SWEDEN | GRABE |
| UNITED STATES | GRASSO |
| GERMANY | GROSS |
| INDIA | GUPTA |
| MEXICO | GUTIERREZ |
| NETHERLANDS | HENDRIKX |
| FRANCE | HOZNEK |
| SPAIN | IBARLUCEA |
| INDIA | KANDASAMI |
| INDIA | KAPOOR |
| THAILAND | KIJVIKAI |
| AUSTRIA | KLINGLER |
| NETHERLANDS | KUMS |
| TURKEY | KURAL |
| ARGENTINA | LABATE |
| GREECE | LIATSIKOS |
| UNITED STATES | LINGEMAN |
| PORTUGAL | LOPES |
| SPAIN | LOPEZ GARCIA |
| UNITED STATES | LOUIE |
| DENMARK | LUKE |
| INDIA | MANDAL |
| GREECE | MELEKOS |
| INDIA | MODI |
| ITALY | MONTANARI |
| UNITED STATES | NADLER |
| UNITED STATES | NAKADA |
| JAPAN | NUTAHARA |
| GERMANY | OLBERT |
| TURKEY | ONAL |
| DENMARK | OSTHER |
| CZECH REP | PACIK |
| INDIA | PAL |
| UNITED STATES | PEARLE |
| UNITED STATES | PREMINGER |
| GERMANY | RASSWEILER |
| CANADA | RAZVI |
| SPAIN | RIOJA |
| ITALY | RIPPA |
| ITALY | SABA |
| FRANCE | SAUSSINE |
| ITALY | SCARPA |
| SPAIN | SERRANO PASCUAL |
| INDIA | SHAH |
| CHINA | SHI |
| CHILE | SILVA BARROILHET |
| GREECE | SKOLARIKOS |
| UNITED STATES | SMITH |
| ISRAEL | SOFER |
| GERMANY | STOLZENBURG |
| NETHERLANDS | STRIJBOS |
| CHINA | SUN |
| CANADA | SZYMANSKI |
| TURKEY | TEFEKLI |
| UNITED KINGDOM | TIMONEY |
| UNITED KINGDOM | TOLLEY |
| TURKEY | TURNA |
| SPAIN | VALDIVIA-URIA |
| BELGIUM | VAN CLEYNENBREUGEL |
| UNITED STATES | VENKATESH |
| NETHERLANDS | VIJVERBERG |
| SWEDEN | WALFRIDSSON |
| UNITED STATES | WOLF |
| UNITED STATES | WONG |
| CHINA | XUE |
| JAPAN | YAMAGUCHI |
| CHINA | ZHANG |