
Abstract
Background and Purpose:
Precise needle puncture of the renal collecting system is an essential step for successful percutaneous nephrolithotomy (PCNL). Puncture is technically challenging and has many pitfalls for the urologic surgeon. We describe the development of a novel navigation system, the Locator, to assist accurate percutaneous needle placement and compare this with conventional manual techniques.
Materials and Methods:
The essence of the device is that it stabilizes the needle for PCNL puncture. It relies on an adjustable lockable multidirectional head that is securely fixed to the operating table. The radiolucent head holds a 10F metal guide that allows renal collecting system puncture. The system uses the traditional fluoroscopic “bull's-eye sign” to achieve precise and fixed alignment. Objective assessment was obtained by in vitro testing using simulated PCNL puncture with and without using the Locator. Time to successful puncture and fluoroscopy screening time (FST) was assessed.
Results:
Six urologic trainees were recruited to test the Locator. Simulated PCNL puncture was quicker and with reduced fluoroscopy when the apparatus was used. The mean FST for traditional hand vs Locator puncture was 46 vs 16 seconds (P = 0.03), and the mean time to puncture was 225 vs 118 seconds (P = 0.26).
Conclusion:
The Locator is a simple, cheap, and novel assistant to achieving successful PCNL puncture. It achieves this by stabilizing the needle during puncture. Preliminary in vitro testing suggests that the device may reduce fluoroscopy exposure and be quicker. The device warrants further evaluation in the clinical setting.
Introduction
We thus aimed to design a simple mechanical apparatus that would aid the urologic surgeon by improving PCNL puncture efficacy. In addition, we wanted the system to decrease time to successful puncture and reduce fluoroscopic screening time (FST).
Materials and Methods
The Locator: Description of the apparatus
The essence of the device is that it stabilizes the needle for PCNL puncture. The device consists of two articulated arms with two spherical joints that provide full positioning (six degrees of freedom) capabilities (Fig. 1). It is securely fixed to the operating table via a standard anesthetic screen (metal right angle) (Figs. 2, 3). The working head consists of a radiolucent extension arm, whose maneuverability is hand controlled outside the fluoroscopy beam (Fig. 2).

The percutaneous nephrolithotomy navigation apparatus consists of a metal bracket (right) that is secured to a metal anesthetic screen. It has two adjustable and lockable multidirectional heads and a radiolucent end piece (left) that contains the metal guide for “bull's-eye sign” fluoroscopic alignment.

Needle arrangement using 10-gauge metal guide on the device, a 14F metal “liver biopsy” needle, and an 18F, 20 cm “two part disposable needle” (left). The bracket to attach to a metal right angle (anesthetic screen) is to be secured to the operating table (right).
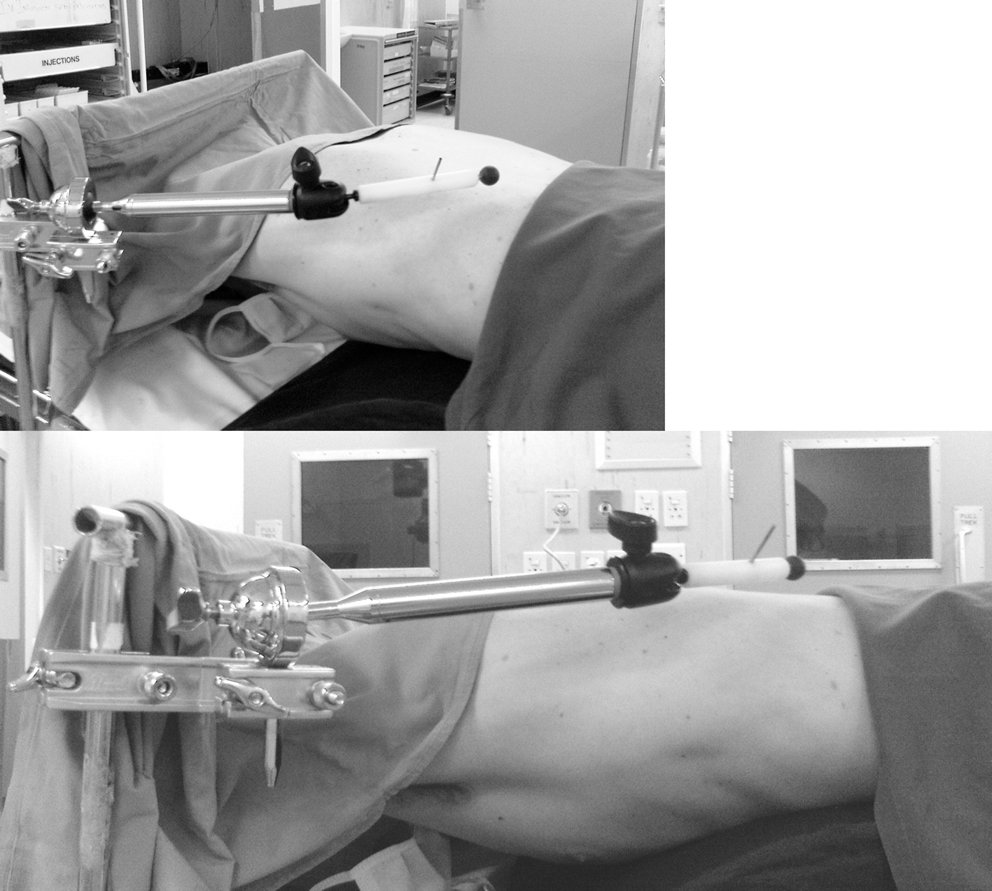
Clinical views of the Locator in situ.
The appropriate direction for needle advancement into the desired renal calix is determined by obtaining a needle superimposition or “bull's-eye sign” on the fluoroscopic screen (Fig. 4). The bull's-eye sign is achieved by aligning the plane of the radiographic beam with the C-arm in the 30-degree position. The fluoroscopic bull's-eye is achieved using the gantry's 10-gauge metal guide (Fig. 2). Into this guide, once alignment is visualized in the 30-degree C-arm position, a 14-gauge metal “liver biopsy” needle is used for puncture of the lumbodorsal fascia. The C-arm is rotated back to the 0-degree position to estimate puncture depth for an 18-gauge Cook® (Bloomington, IN) disposable two-part trocar needle to make the renal and collecting system puncture.
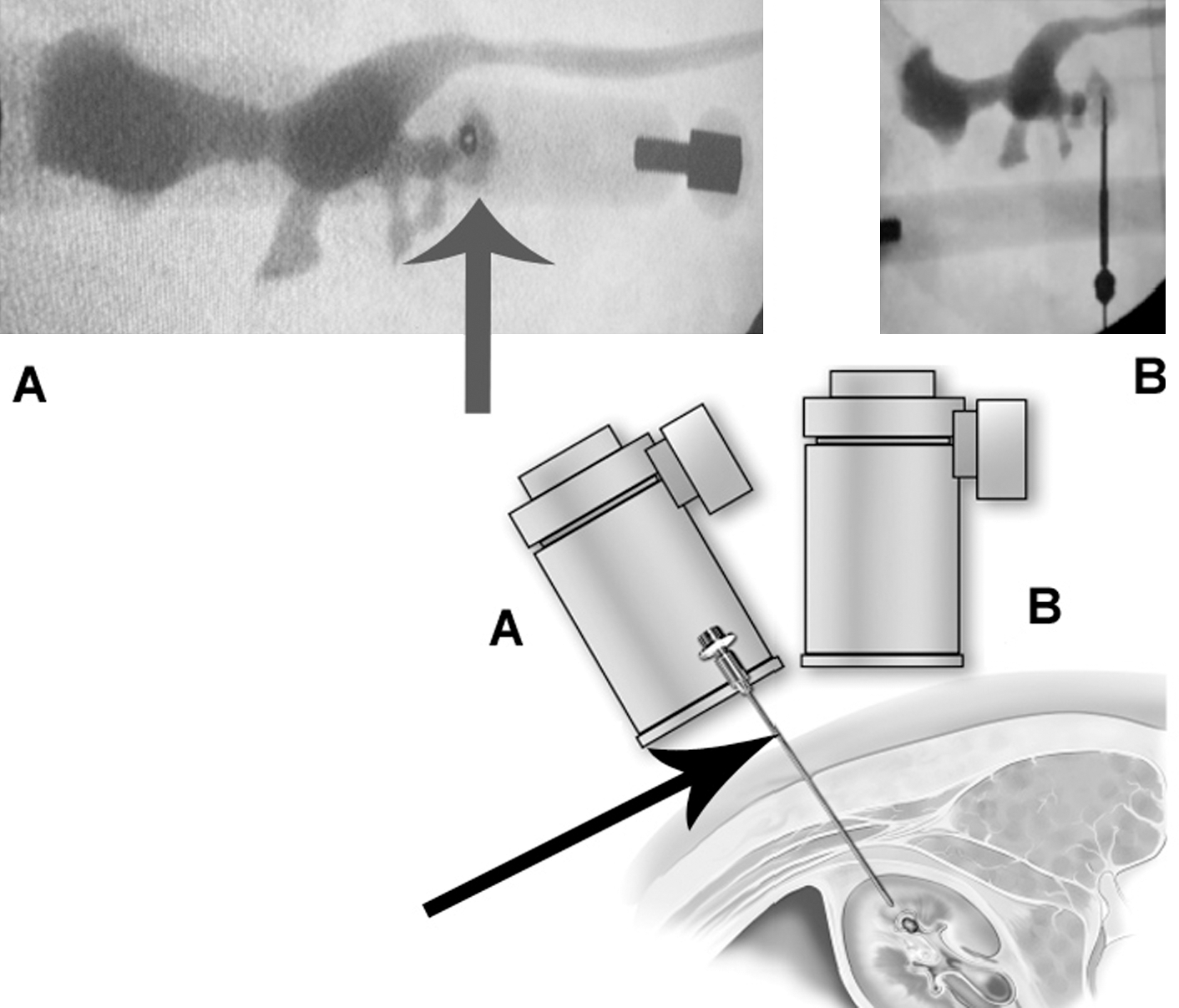
The black arrow shows where the Locator device is positioned to stabilize the needle during otherwise routine fluoroscopic percutaneous nephrolithotomy puncture. (
Assessment of puncture efficacy
Our aim was to ascertain if the Locator confers any advantage to the surgeon who is performing PCNL. Objective assessment of the efficacy of the apparatus was obtained by in vitro testing. This was done by simulated PCNL puncture with and without use of the Locator. Six urologic trainees (with little previous PCNL experience) were recruited for the testing. Two end points were assessed: Time to successful puncture and FST.
The in vitro testing method (Fig. 5) involved fluoroscopic screening of a small (2 cm) hidden (under 10 cm polystyrene) radiopaque metal key. The key was connected to an electric circuit, and a light illuminated when the key was successfully touched by the puncture needle.

In vitro testing using simulated fluoroscopy puncture with a small (2 cm) hidden radiopaque key connected to an electric circuit to indicate when the key is touched by the puncture needle.
The Student t test (paired) was used to assess statistical significance, using GraphPad software. 4
Results
The mean FST for simulated PCNL puncture was statistically reduced if the Locator was used by the trainees, 16 vs 46 seconds (P = 0.03), compared with traditional hand puncture. Total time for puncture was reduced in the Locator group, but this did not reach statistical significance (118 vs 225 seconds, P = 0.26).
Discussion
PCNL is established as the main modality for managing large renal calculi since Fernstrom and Johansson 5 first used a nephrostomy tract to extract a stone in 1976.
PCNL is presently the most demanding operative stone technique to master. This difficulty is solely related to obtaining access to the renal collecting system.
Published data suggest that learning curves for PCNL plateaus only after 60 procedures as primary surgeon. 6 Successfully obtaining this renal access is a challenging task for many urologists. Lee and coworkers 7 found that only 27% of urologists who were trained in PCNL continue to perform it. In addition, only 11% of American urologists who perform PCNL obtain the access themselves. 3 Various aids have been developed to improve apprenticeship, including laboratory simulators, virtual reality trainers, etc. 8,9
The goal in developing the Locator was to overcome the technical difficulties of PCNL access and reduce the learning curve for trainees. It is a simple and cheap apparatus that stabilizes the needle during the puncture process.
Various techniques are described to obtain collecting system puncture. Most urologic surgeons use the bull's-eye sign technique making use of the end-on needle appearance at 30 degrees off the vertical plain under fluoroscopy to achieve correct alignment. 10 The Locator uses this same technique but removes the need for periodic checking of fluoroscopic alignment, as in the manual technique. Once the bull's-eye sign is obtained, the Locator is locked in place, thus avoiding any drift in alignment as commonly occurs with a manual puncture.
The limitations of the in vitro assessment of the device's efficacy need to be acknowledged:
The number of trainees used was small.
Concerns about unnecessary radiation exposure limited the number of puncture attempts the trainees were requested to perform.
The crude assessment tool (Fig. 4) does not accurately simulate the challenges of in vivo puncture. For example, there was no movement of the target because of respiration.
In spite of these limitations, this preliminary report has indicated that the device possibly has a potential to reduce FST and make the puncture faster. Further in vivo clinical assessment to prove this is warranted.
Ultrasonography has been advocated as an alternative to fluoroscopy. It prevents radiation exposure and advocates claim it can be used for all stages of the PCNL procedure. 11 Fluoroscopic guidance, however, remains de facto the preferred modality. 1 The deleterious effects of ionizing radiation are well known, and various techniques have been described to reduce exposure by using a dose that is “as low as reasonably achievable” (the ALARA principle). 12
Tepeler and associates 1 have demonstrated that in a series of 282 patients undergoing PCNL in which the mean FST was 10.19 minutes. This time was significantly prolonged by large stone burden and multiple access procedures. It has been estimated that a urologist can perform 35 PCNL procedures per month and stay within the safety recommendations. 1 The Locator may have the potential to protect the urologic surgeon and the patient from the radiation hazard.
Various sophisticated robots have been developed to aid PCNL puncture. Wickham, Imperial College London, initiated this work that was refined at Johns Hopkins, Baltimore, with the development in 2003 of the Tracker and later the AcuBot (URobotics). 13,14 This robot is mounted onto the operating table, is remotely controlled, has six degrees of freedom of the robotic arm, and can be used with fluoroscopic or CT guidance. It is in clinical use and has been shown to improve the accuracy of needle placement compared with standard manual techniques. 15 Robotic puncture compared favorably for time to access, number of attempts, and estimated blood loss. These robotic devices, however, remain expensive and are not yet in wide clinical use.
Conclusion
The Locator is a simple, cheap, and novel assistant for achieving successful PCNL puncture. Preliminary in vitro testing has suggested that the device possibly has the potential to reduce fluoroscopy exposure and achieve a quicker puncture. A mechanical engineer has refined the apparatus, and further clinical evaluation to attempt to prove its efficacy is warranted.
Footnotes
Disclosure Statement
No competing financial interests exist.