
Abstract
Purpose:
We established a new strategy for nonpalpable testis, including intra-abdominal testis, testicular nubbins, and intracanalicular testis, to correct these conditions by laparoscopic procedures.
Patients and Methods:
Of the 53 boys (mean age, 24.5 months), nonpalpable testis was on the right side in 13, on the left in 34, and bilateral in 6. Three boys with nonpalpable testis involved contralateral palpable undescended testis. We applied only laparoscopic treatment without open inguinal incision for all cases. After laparoscopic orchiopexy and orchiectomy, we performed subsequent laparoscopic inguinal ring and/or peritoneal defect closure to prevent postoperative inguinal hernia formation, and concurrent laparoscopic repair for cases of contralateral undescended testes and open processus vaginalis under the same anesthesia.
Results:
All boys underwent laparoscopic treatment immediately after laparoscopic evaluation. We performed laparoscopic orchiopexy for 22 cases with intra-abdominal testes. Twenty-seven boys underwent laparoscopic groin exploration, and 24 underwent subsequent laparoscopic orchiectomy for testicular nubbins, and 3 underwent subsequent laparoscopic orchiopexy for intracanalicular testes. In two boys with testicular nubbin, an open processus vaginalis was present. Forty-nine boys underwent laparoscopic inguinal ring and/or peritoneal defect closure after orchiopexy or orchiectomy to prevent inguinal hernia formation or hydrocele testis. Concurrent laparoscopic contralateral inguinal closure was performed for two cases with opened contralateral processus vaginalis.
Conclusions:
Our new strategy is useful because all patients with nonpalpable testis could be treated successfully by only laparoscopic management, avoiding open inguinal incision, preventing inguinal hernia formation, and enabling the concurrent repair of contralateral undescended testis and open processus vaginalis.
Introduction
Laparoscopic orchiopexy has gained great acceptance for intra-abdominal testis, although multiple orchiopexy techniques have been used. The main advantage is that laparoscopic orchiopexy allows us to dissect the spermatic cord structure into the retroperitoneum up to the level of the origin of the spermatic vessels. This dissection enables fixing the testis in the scrotum without tension on the cord. Another advantage of laparoscopic orchiopexy is the ability to start treatment as soon as a diagnosis is made and to permit minimally invasive surgery. This advantage can apply to other cases, such as testicular nubbin and intracanalicular testis.
In general, there are several possible surgical findings of diagnostic laparoscopy for nonpalpable testis. The first is an intra-abdominal vanishing testis (blind ending vas and vessels), indicating that further exploration is generally unnecessary. The second is intra-abdominal testis, for which laparoscopic orchiopexy is generally indicated. The third is the vas and vessels exiting the internal ring, diagnosed as extra-abdominal testicular nubbin or intracanalicular undescended testis. In this case, generally, a subsequent open inguinal incision was made to perform orchiectomy for testicular nubbin or orchiopexy for intracanalicular undescended testis; however, we considered that laparoscopic groin exploration after laparoscopic observation could avoid unnecessary open inguinal incision because it enables subsequent laparoscopic orchiectomy or orchiopexy.
This strategy may enable laparoscopic treatment for every case with nonpalpable testis, and concurrent laparoscopic procedures, such as laparoscopic inguinal ring and/or peritoneal defect closure to prevent postoperative inguinal hernia formation or hydrocele testis, and laparoscopic repair for cases of contralateral undescended testes and open processus vaginalis under the same anesthesia.
In this study, we present our new strategy for nonpalpable testis, including intra-abdominal testis, testicular nubbins, and intracanalicular testis, to correct these cases by only laparoscopic procedures, and discuss the possible benefits of this strategy.
Patients and Methods
Fifty-three boys with 59 nonpalpable testis (9–142 months old; mean age 24.5 mos) presented at our institution from November 2006 to July 2010. The diagnosis of nonpalpable testis was established at least three times—during the office examination, at the time of admission, and was confirmed by examination with the patient under general anesthesia. Testes that became palpable under anesthesia were excluded from the study. Of these 53 boys, nonpalpable testis was on the right side in 13, on the left side in 34, and bilateral in 6. Three boys with unilateral nonpalpable testis involved contralateral palpable undescended testis.
We applied only laparoscopic treatment without open inguinal incision for all these cases. In addition, after laparoscopic orchiopexy and orchiectomy, we performed subsequent laparoscopic inguinal ring and/or peritoneal defect closure to prevent postoperative inguinal or hydrocele testis formation, and concurrent laparoscopic repair for cases of contralateral undescended testes and open processus vaginalis under the same anesthesia. All operations were performed mainly by one surgeon (YK).
Surgical techniques
An anterior scrotal incision was made and a subdartos pouch created. A step dilator and trocar system was used to deliver the testis to the scrotum, as previously reported. 5 A laparoscopic grasper was passed through the neoinguinal canal from the scrotum to the neointernal ring medial to the inferior epigastric vessels. and the testis was delivered in the scrotum via the neoinguinal canal. The testis was fixed in the scrotum using a 5-0 polyglactin suture. If the vessel cord was too short to move the testis to the opposite internal ring without tension, we performed laparoscopic one-stage Fowler-Stephens orchiopexy using a low ligation procedure. Finally, laparoscopic complete closure of the internal ring and peritoneal defect was performed with 5-0 polyglactin to prevent postoperative inguinal hernia formation or hydrocele testis.

Laparoscopic groin exploration and subsequent laparoscopic internal ring and peritoneal defect closure.
Results
We performed laparoscopic observation and subsequent laparoscopic orchiopexy for intra-abdominal testes and intracanalicular testes, or laparoscopic orchiectomy for testicular nubbins, depending on the presence and location of the testes (Fig. 2). Of the 53 boys, 22 had intra-abdominal testes, including 9 on the left and 10 on the right, and 3 on both. Twenty-four had testicular nubbins, 21 on the left and 3 on the right. Four had intra-abdominal vanishing testes (blind ending cord) on the left. Three boys with bilateral nonpalpable testes had intracanalicular undescended testes bilaterally. All boys, except four cases of intra-abdominal vanishing testes, underwent laparoscopic management using three trocars immediately after laparoscopic evaluation. Of the 22 boys with intra-abdominal testes, 21 underwent laparoscopic orchiopexy, while 1 underwent one-stage Fowler-Stephens laparoscopic orchiopexy with the low ligation technique. All testes reached into the low or midscrotum. Three boys with intra-abdominal testes and coexistent contralateral intracanalicular palpable testes underwent laparoscopic bilateral orchiopexy using the same trocars without further additional trocar placement under the same general anesthesia.
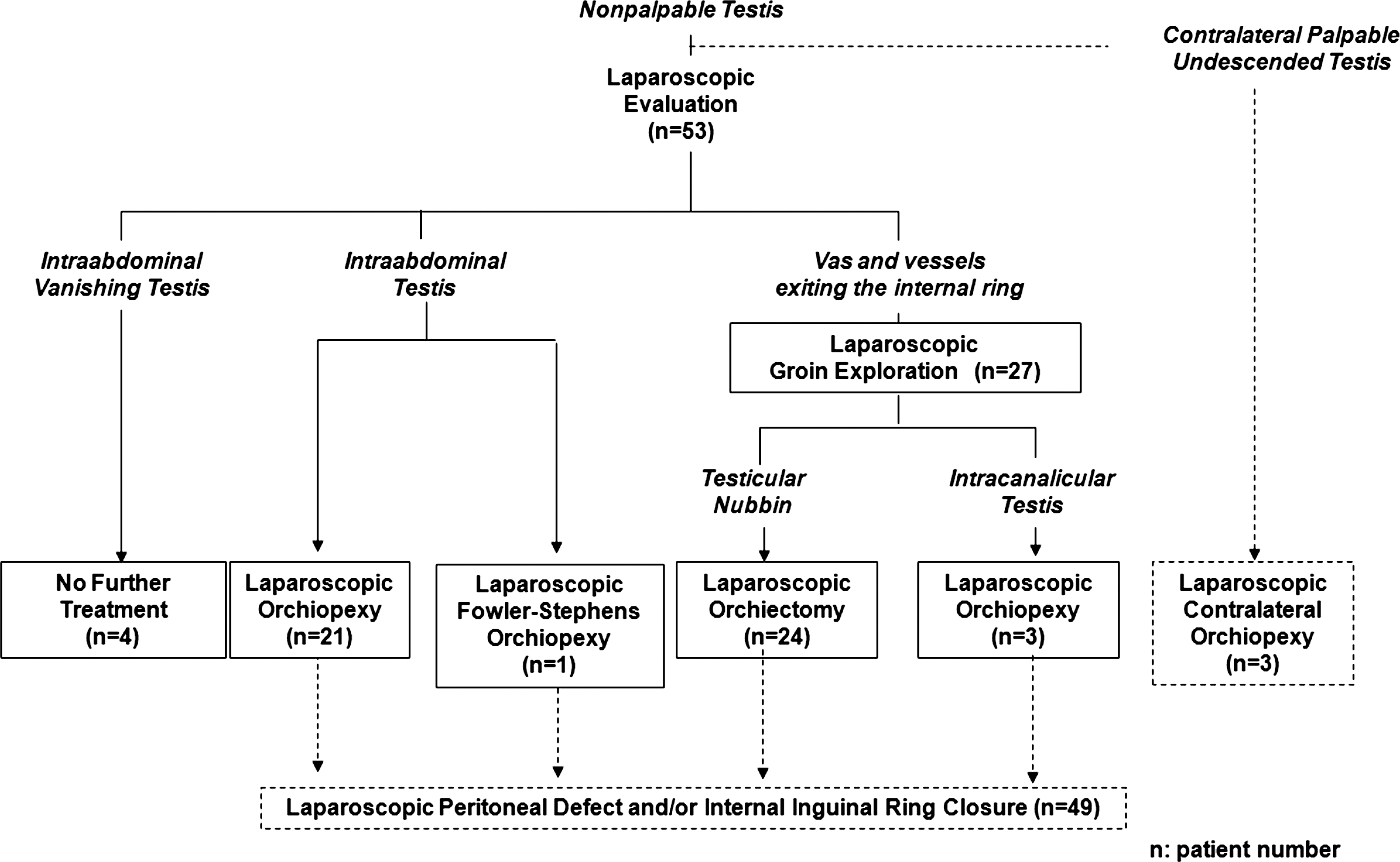
Results of laparoscopic examination and subsequent management for nonpalpable testis.
All boys with testicular nubbins underwent laparoscopic groin exploration and subsequent laparoscopic orchiectomy. A nubbin in all cases were delivered into the abdomen and removed successfully. On histopathologic examination of resected testicular nubbin specimens, the structure of seminiferous tubules was completely lost; hemosiderin deposits were observed. In two boys with testicular nubbins, an open processus vaginalis was present, and simultaneous laparoscopic transaction of the processus vaginalis and subsequent internal ring closure were performed. Three boys with bilateral intracanalicular undescended testes, which were not palpable despite careful physical examination under general anesthesia, had bilateral open processus vaginalis and underwent bilateral laparoscopic groin exploration and subsequent laparoscopic orchiopexy and internal ring and peritoneal defect closure. As a result, therefore, nine boys, including three boys with bilateral intra-abdominal testes, three boys with bilateral intracanalicular undescended testes, and three boys with intra-abdominal testes, and coexistent contralateral intracanalicular palpable testes underwent laparoscopic bilateral orchiopexy.
We performed laparoscopic internal ring and/or peritoneal defect closure to prevent postoperative inguinal hernia formation or hydrocele testis for all 49 boys who underwent laparoscopic orchiopexy and orchiectomy. In two boys with unilateral intra-abdominal testes or testicular nubbins, the contralateral processus vaginalis was opened, and laparoscopic contralateral inguinal closure was performed.
The average surgical time for observation in boys with intra-abdominal vanishing testes (blind ending cord) was 12.5 ± 2.9 minutes. The average surgical times, including the diagnostic time, were 125.0 ± 18.2, 89.6 ± 27.2, and 44.5 ± 17.2 minutes in bilateral laparoscopic orchiopexy, unilateral orchiopexy, and laparoscopic orchiectomy with subsequent inguinal ring and/or peritoneal defect closure, respectively. The preopertive and postoperative appearances of the internal ring in the cases of intra-abdominal testis, testicular nubbin, and intracanalicular testis are shown in Figure 3.
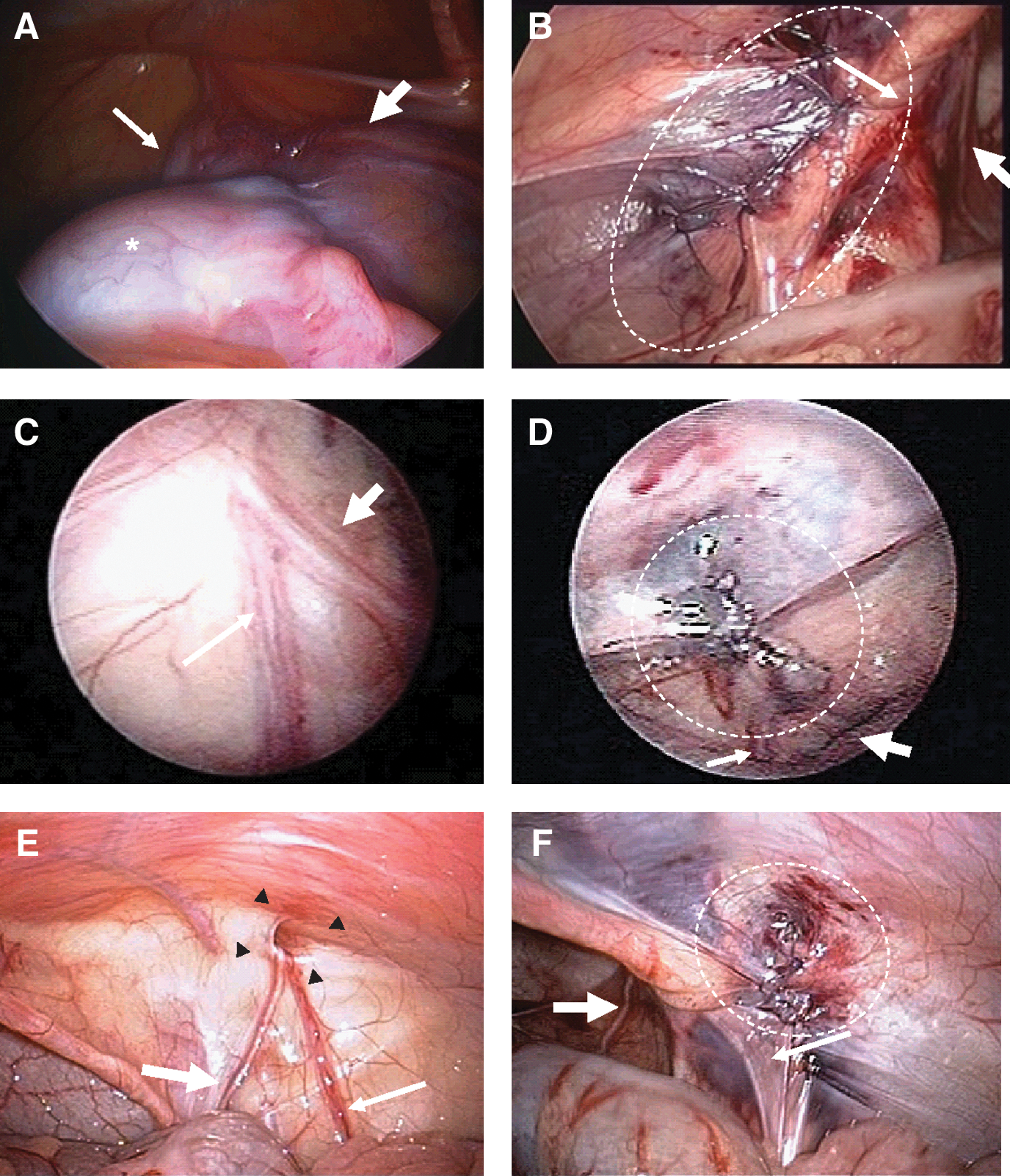
Preoperative (
There were no intraoperative or postoperative complications. Mobilization and normal oral intake were allowed the next day in all boys, and they had all resumed full activity by the following day. Follow-up ranged from 1 to 45 months (mean 19.0 mos). All boys who underwent laparoscopic orchiopexy had testes equivalent to their preoperative size in the scrotum, and there has been no evidence of testicular atrophy. Postoperative inguinal hernia formation and hydrocele testis were not observed in any cases.
Discussion
In this study, we applied only laparoscopic treatment without open inguinal incision for all boys with intra-abdominal testes, testicular nubbins, or intracanalicular testes. After laparoscopic orchiopexy and orchiectomy, we could perform subsequent laparoscopic inguinal ring and/or peritoneal defect closure to prevent postoperative inguinal hernia formation or hydrocele testis. In addition, we could perform concurrent laparoscopic repair for cases of contralateral undescended testes and open processus vaginalis under the same anesthesia.
Laparoscopic orchiopexy for intra-abdominal testis is advocated as a standard procedure; however, a potential dilemma arises when the vas and vessels are seen exiting the internal ring, as either a testis or nubbin may be found distally. 6 Many surgeons make an open inguinal incision to complete exploration and to find the testis or testicular nubbin; therefore, most patients undergoing initial laparoscopy will have either a second inguinal incision to remove a testicular nubbin or a scrotal incision to place the testis. On the other hand, laparoscopic groin exploration can avoid unnecessary open inguinal incision.
Recently, the usefulness of scrotal incision for the management of unilateral nonpalpable testis has been reported because the majority of testicular nubbins are easily removed via this approach and the cosmetic outcome is excellent. 6 –9 Although initial scrotal incision is a useful procedure for scrotal testicular nubbin, it may be unacceptable for some cases of intracanalicular testicular nubbin and the presence of patent processus vaginalis. The rate of scrotal testicular nubbin varies among previous reports.
Belman and Rushton 8 reported that a vanished testis was mostly a scrotal event and recommended scrotal exploration and not laparoscopy as the first step if surgery is selected in boys with a solitary testis. Snodgrass and associates 9 reported that of 30 monorchism cases, scrotal nubbins occurred in 26 (87%) and inguinal nubbins occurred in 2 (7%); however, Alam and Radhakrishna 10 reported that 9 of 15 (60%) testicular nubbins were located in the inguinal region. As reported previously, an advantage of laparoscopic groin exploration and subsequent orchiectomy for vanishing testis may be to remove the intracanalicular testicular nubbin more completely, irrespective of location of testicular nubbin, because the antegrade approach can provide good anatomic orientation for observation and removal. 11 In addition, this procedure enables closure of an open processus vaginalis, although scrotal incision has the possibility of leaving it, because we cannot know about the presence of the processus vaginalis until we observe the internal inguinal ring.
In our study, an ipsilateral and contralateral open processus vaginalis was present in two (8%) boys and one (4%) boy, respectively, with a testicular nubbin. Elder 12 reported that 4 (5%) of 79 vanished or absent testes had a patent processus vaginalis. We believe that laparoscopic transection of the processus vaginalis and subsequent internal ring closure after laparoscopic orchiectomy is necessary for boys with a testicular nubbin to prevent postoperative inguinal hernia formation or hydrocele testis, as described below in detail.
Although Schleef and colleagues 13 previously reported laparoscopic groin exploration and resection of the nubbin for vanishing testis with a hypoplastic cord structure exiting the internal ring by initial laparoscopic observation, they performed an open inguinal incision and subsequent open orchiopexy for intracanalicular testis with a normal-sized cord structure exiting the internal ring, and transscrotal orchiopexy for a contralateral undescended testis. We could perform laparoscopic orchiopexy for not only an intra-abdominal testis but also intracanalicular testis with findings of a normal cord structure by initial laparoscopic evaluation, and contralateral palpable undescended testis. Docimo and coworkers 14 performed laparoscopic orchiopexy for a highly palpable undescended testis and reported its usefulness. Riquelme and associates 15 reported that laparoscopic orchiopexy for a palpable undescended testis could be performed without a higher complication rate than the open procedure with several advantages over the laparoscopic approach. We also believe that laparoscopic orchiopexy could be useful for intracanalicular undescended testis, especially in nonpalpable cases, because it can be performed immediately after accurate diagnosis by laparoscopy.
Whether inguinal ring and/or peritoneal defect closure after orchiopexy for intra-abdominal and intracanalicular testis as well as orchiectomy for testicular nubbin is necessary remains controversial. The processus vaginalis or hernia sac is usually separated from the cord structures and ligated at the internal ring during open orchiopexy; however, most reports do not close the native internal ring when laparoscopic orchiopexy is performed, although there are reports of postoperative hernia formation and hydrocele testis. 16,17 Dissection of the spermatic cord structure into the retroperitoneum is needed to fix the testis in the scrotum without tension on the cord. After dissection of the spermatic cord structure, a large peritoneal defect is made. Laparoscopic inguinal ring and/or peritoneal defect closure are easy and safe procedures; therefore, this procedure should be advocated after laparoscopic orchiopexy for intra-abdominal testis to prevent postoperative inguinal hernia formation and hydrocele testis. As described above, laparoscopic internal ring closure should also be advocated for patients with testicular nubbins for the same reason.
We performed bilateral laparoscopic orchiopexy and complete laparoscopic internal ring closure with only three trocar placements without further additional trocar placement for three boys with both nonpalpable testis and a contralateral palpable undescended testis. In two boys with a unilateral intra-abdominal testis or testicular nubbin, the contralateral processus vaginalis was opened, and concurrent laparoscopic contralateral inguinal closure was performed. Palmer and Rastinehad 18 reported that the incidence of an open internal ring was about 9%, and the usefulness of concurrent laparoscopic repair of the contralateral hernia. Another advantage of our strategy is that it enables the contralateral palpable undescended testis and contralateral patent processus vaginalis to be inspected or repaired completely at the same time.
Conclusions
Our new strategy is useful because all patients with nonpalpable testis could be treated safely and successfully by only laparoscopic management, with avoidance of open inguinal incision, prevention of inguinal hernia formation or hydrocele testis, and the concurrent repair of contralateral undescended testis and open processus vaginalis, although further evaluation will be needed.
Footnotes
Disclosure Statement
No competing financial interests exist.