
Abstract
Purpose:
To determine the influence of warm or cold ischemia on postoperative renal function, we conducted preoperative and postoperative analysis by renal scintigraphy of patients who were undergoing open partial nephrectomy (OPN) and laparoscopic partial nephrectomy (LPN).
Patients and Methods:
From May 2005 to February 2010, the preoperative and postoperative renal function was evaluated by 99mTc-mercaptoacetyltriglycine (MAG3) clearance in 37 patients who were treated with OPN (n=13) and LPN (n=24). LPN were achieved via retroperitoneal (RPLPN; n=12) or transperitoneal (TPLPN; n=12) routes. Renal cooling was performed after renal hilar clamping in OPN and RPLPN, but not TPLPN. Renal function was evaluated according to the ratio of affected to contralateral renal MAG3 clearance.
Results:
Mean ischemic time was 29.5 minutes in OPN, 25.5 minutes in TPLPN, and 50 minutes in RPLPN (P<0.01); median blood loss was 230 mL in OPN (P<0.05), 110 mL in TPLPN, and 53 mL in RPLPN. There was no significant difference in postoperative total renal function between the groups. Although ischemic time in RPLPN was longer than in TPLPN, the postoperative recovery of affected renal function from 1 week to 3 months for RPLPN and OPN (cold ischemia) was significantly better than for TPLPN (P<0.01).
Conclusions:
Cold ischemia has an advantage of postoperative recovery of affected renal function. If a patient has a risk of renal dysfunction, cold ischemia during renal hilar clamping is recommended to avoiding deterioration.
Introduction
It is important to preserve renal function after LPN and to select appropriate methods for LPN. Previous studies have demonstrated methods for reducing warm ischemia, such as the modified closure technique, 2 on-demand extracorporeal clamping, 3 or renal cooling during tumor extraction. 4 Some authors have suggested that renal damage occurs when warm ischemia exceeds 30 minutes, especially in patients with a risk of renal dysfunction, such as those of older age. 5,6 In contrast, Bhayani and associates 7 have shown that warm ischemia for up to 55 minutes does not significantly influence long-term renal function after LPN. Beri and colleagues 4 have suggested intraoperative cold ischemia for LPN using arterial perfusion as a viable alternative when ischemia time is expected to exceed 30 minutes in patients with complex tumors. Renal cooling during renal clamping and the safe limit for ischemic time have been discussed in many reports.
In the present study, to determine the impact of cold and warm ischemia on postoperative renal function, we evaluated preoperative and postoperative affected renal function by 99mTc-mercaptoacetyltriglycine (MAG3) in patients who were undergoing open partial nephrectomy (OPN) and LPN.
Patients and Methods
Patients
From May 2005 to February 2010, 37 patients received a diagnosis of renal tumor, including 25 (68%) men and 12 (32%) women, with a median age of 59 years (range 35–82 years). The anatomic aspects of the renal tumors were evaluated by the Preoperative Aspects and Dimensions Used for an Anatomical (PADUA) classification of renal tumors. 8 The patients were treated with OPN (n=13) or LPN (n=24), including transperitoneal LPN (TPLPN; n=12) or retroperitoneal LPN (RPLPN; n=12) in a single institution. The patients gave their consent to evaluation of renal function by renal scintigraphy after the operation. There was no difference in renal function and preexisting diseases, such as hypertension or diabetes mellitus, between the two groups.
Operation
OPN was performed in patients with cystic, buried, or hilar tumor. TPLPN or RPLPN was selected according to the location of the tumor; TPLPN was performed for tumors located at the front and inside the kidney, and RPLPN was performed for tumors in other locations. To prevent renal damage, intravenous injections of 100 mL 20% mannitol were administered before renal artery clamping and after removal of the clamp in all cases. In cases of OPN or RPLPN, the affected kidney was cooled by ice slush or near-freezing saline, respectively, after clamping of the renal vessels. In cases of RPLPN, near-freezing saline was infused from the stopcock of the port that was connected to a pressured infusion bag by a wide irrigation tube. The 2-L near-freezing saline could be rapidly injected while aspirating the saline that was warmed in the retroperitoneal space. 9 For preparation of near-freezing saline, the 1-L bag of saline was placed in a freezer at −30°C for 3 hours before surgery and kept in a refrigerator at 4°C. This protocol resulted in ice formation in about half of the bag. The saline temperature was 2.0 to 4.0°C.
Evaluation of renal function
Renal function was analyzed by estimated glomerular filtration rate (eGFR)=194×serum creatinine−1.094×age−0.287×(1 − sex × 0.261), where sex was 0 for male and 1 for female, and renal scintigraphy using 99mTc-MAG3 before and 1 week and 3 months after the operation. Affected renal function was evaluated by the ratio of affected renal MAG clearance to contralateral renal MAG clearance. The Steel-Dwass test is a nonparametric multiple comparison procedure and was performed to evaluate the differences among the groups.
Results
Patient characteristics and the operative data for PN for renal tumor are shown in Table 1. There were no differences in median tumor size and operative time between the groups. The median ischemic time for RPLPN (50 min; range 33–58 minu) was significantly longer than that for OPN (29.5 min; range 21–54 min) and TPLPN (25.5 min; range 14–64 min) (P<0.01). Blood loss during OPN was a median 230 mL (range 65–583 mL), which was greater than that for TPLPN (110 mL; range 20–1000 mL) and RPLPN (53 mL; range 16–252 mL) (P<0.05). The median PADUA score was 9 (range 8–11) for OPN, 7 (6–9) for TPLPN, and 8 (7–10) for RPLPN. Intraoperative complications were observed in one patient, who experienced pneumothorax during RPLPN. Postoperative hematoma (no blood transfusion) was observed in two patients in the OPN and TPLPN groups. Pathologic examination revealed renal-cell carcinoma in 31 patients, angiomyolipoma in 4, and oncocytoma in 2. All surgical margins were found to be negative for residual malignancy.
P<0.01.
P<0.05.
OPN=open partial nephrectomy; LPN=laparoscopic partial nephrectomy; TPLPN=transperitoneal LPN; RPLPN=retroperitoneal LPN; PADUA=Preoperative Aspects and Dimensions Used for an Anatomical.
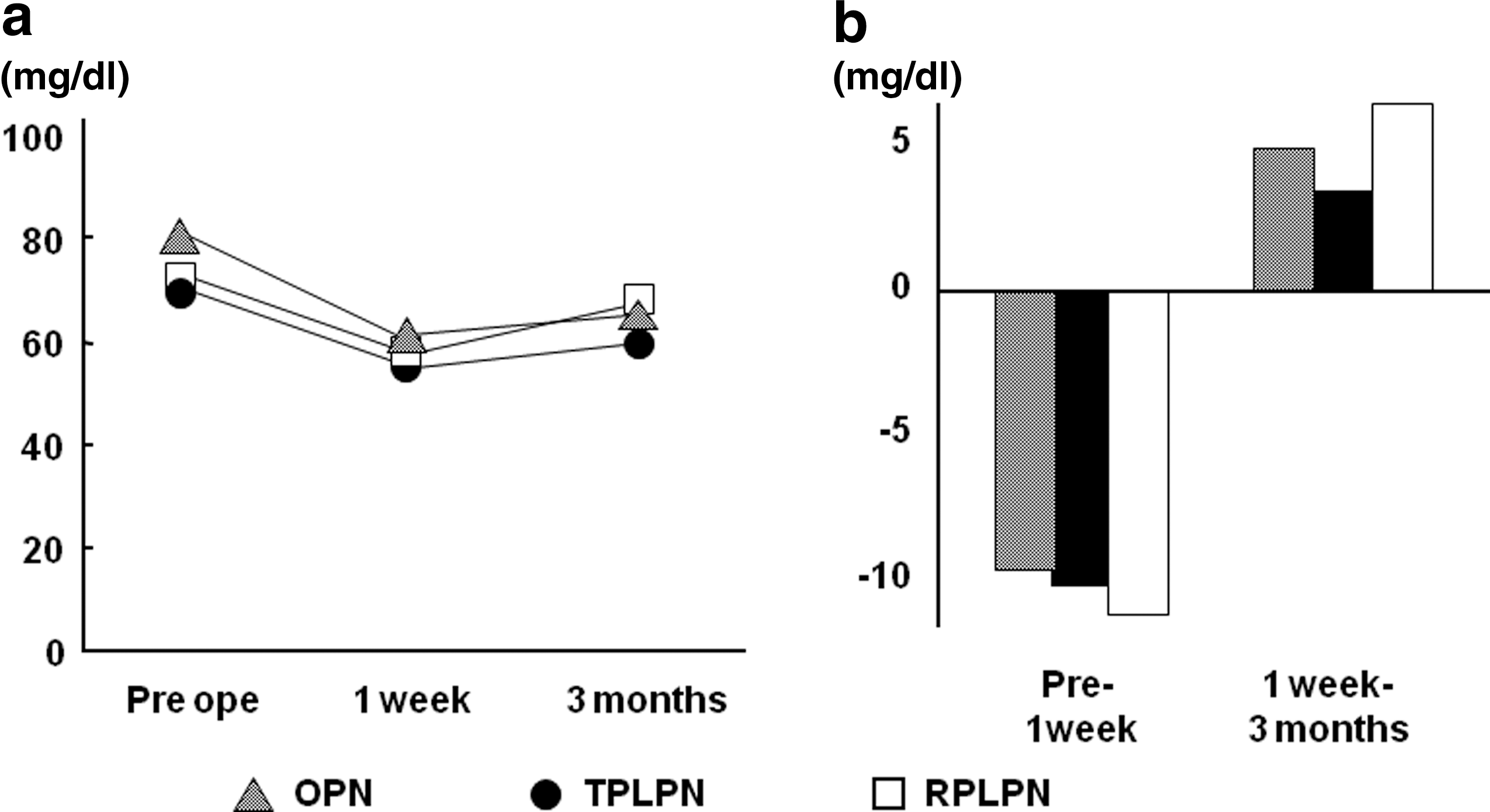
Preoperative and postoperative total renal function estimated by eGFR and the change after operation are shown in Figure 1. eGFR increased 1 week after surgery, and 3 months later it recovered to preoperative levels. There was no significant difference in total renal function and change in eGFR between the groups.
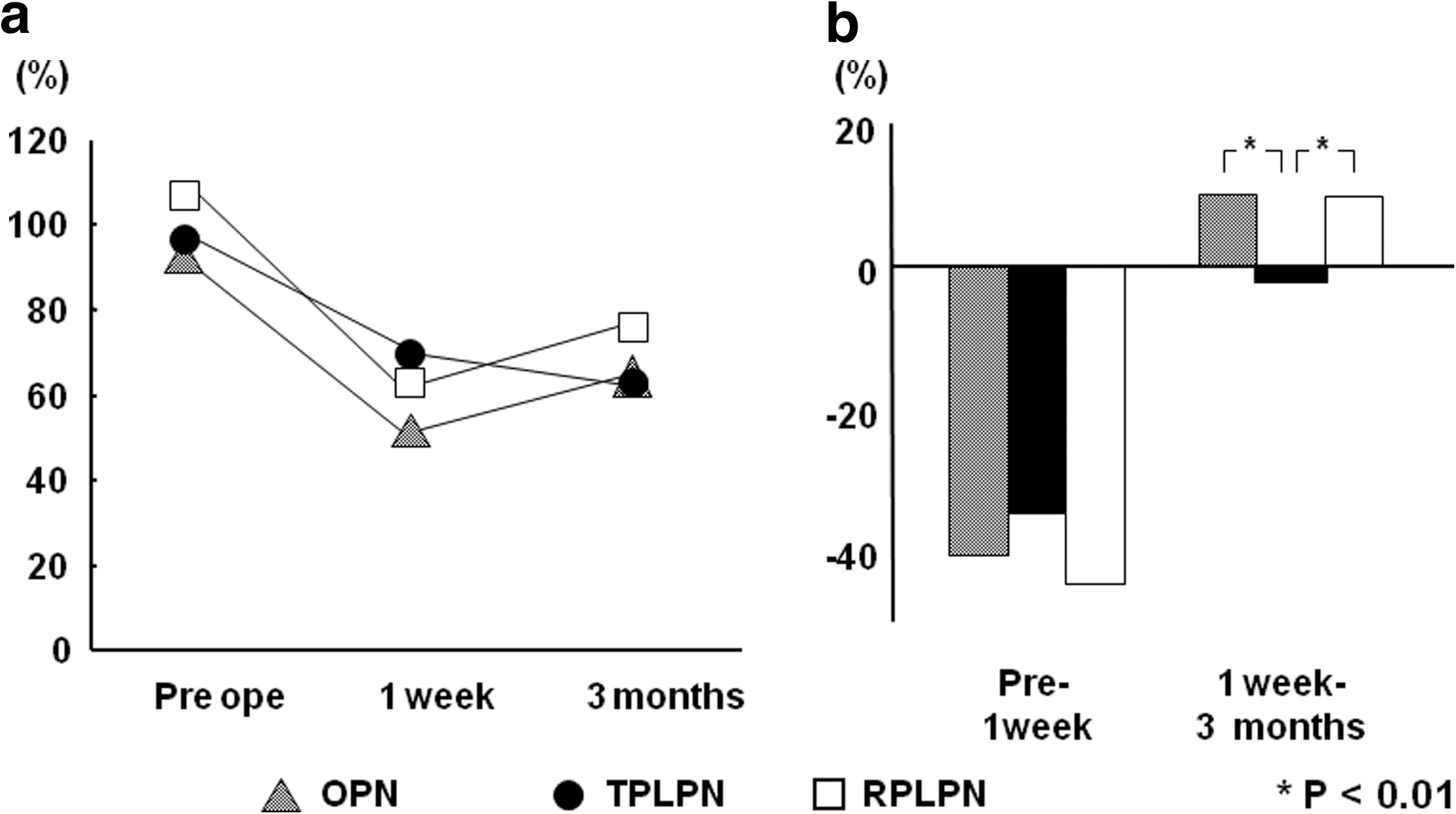
Preoperative and postoperative affected renal function and the change after surgery are shown in Figure 2. The affected renal function that was evaluated by affected/contralateral renal MAG clearance decreased by about 40% at 1 week after surgery in both groups, and then recovered by about 10% from 1 week to 3 months after surgery, but not in the TPLPN group. Although ischemic time in the RPLPN group was longer than in the TPLPN group, the postoperative recovery of affected renal function from 1 week to 3 months in the RPLPN and OPN (cold ischemia) groups was significantly better than that in the TPLPN (warm ischemia) group (P<0.01).
The relationship between ischemic time and postoperative recovery of affected renal function is shown in Figure 3. There was a negative correlation between warm ischemic time and change in affected renal function (R=−0.39) that did not reach statistical significance in the TPLPN group (Fig. 3a). In cases with warm ischemic time of ≥30 minutes, the affected renal function did not improve from 1 week to 3 months after surgery (Fig. 3a). In contrast, in almost all cases when cold ischemia was performed, the affected renal function did not decrease (Fig. 3b).
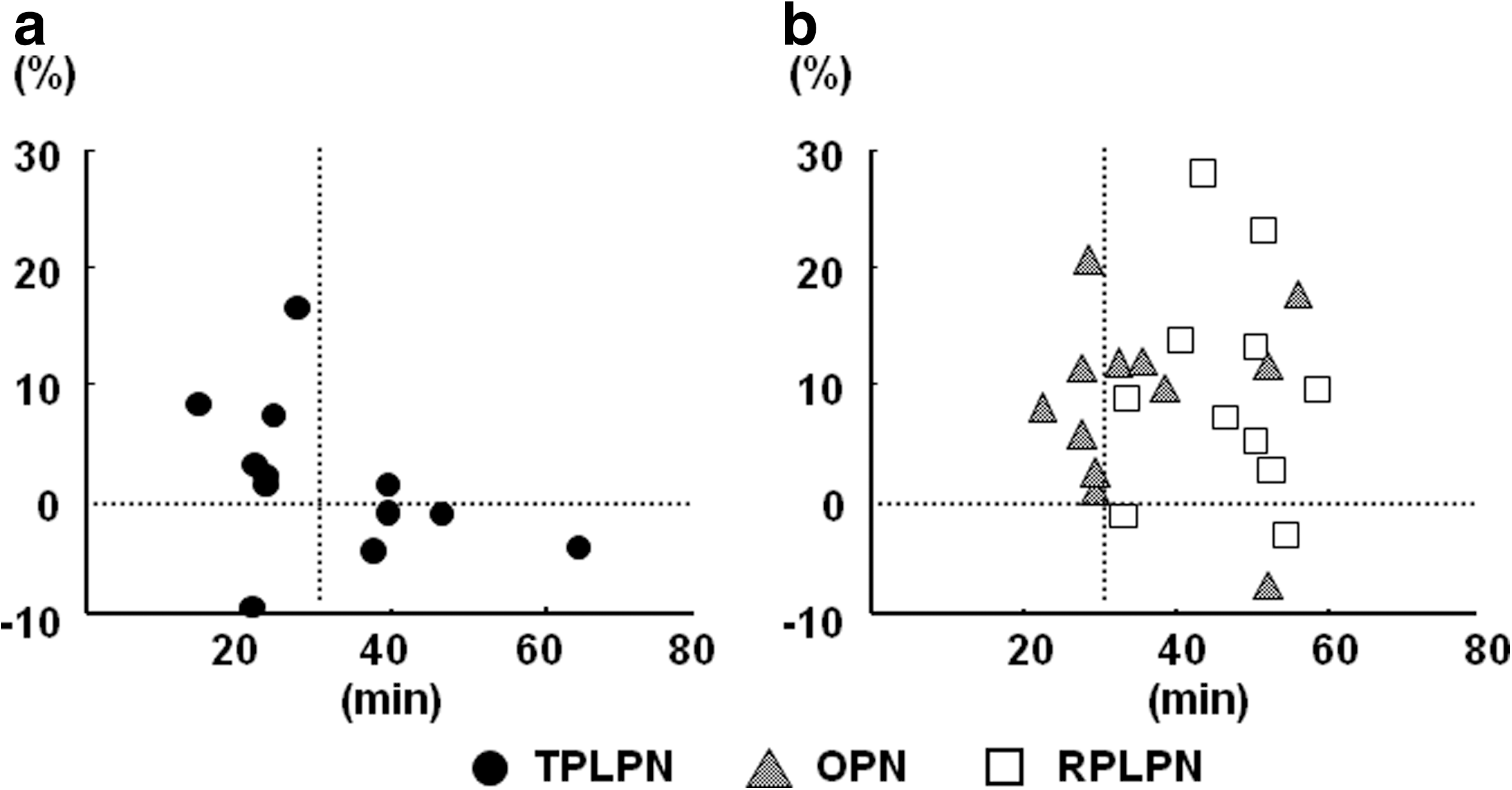
Ischemic time and postoperative recovery of affected renal function from 1 week to 3 months after
Discussion
Radical nephrectomy is a significant risk factor for the development of chronic kidney disease; therefore, PN is recommended to avoid renal dysfunction and is being increasingly performed. 10 Successful preservation of renal function after PN depends on renal ischemia during tumor extraction. The methods for preventing renal dysfunction caused by renal ischemia are still under discussion.
The renal vessels are usually clamped to avoid bleeding when the tumor is extracted by PN. The renal hilum is clamped with renal cooling (cold ischemia) in many cases, because cooling avoids severe damage to the kidney. In contrast, warm ischemia refers to clamping of blood vessels without cooling the kidney, and a short ischemic time is important for prevention of renal dysfunction. Previous studies have shown that a long warm ischemic time is associated with recovery of renal function and increased risk of renal dysfunction. 4 –6,11,12
The safe limit for warm ischemic time has been discussed in recent studies that have shown renal dysfunction in the 35–50-minute range. 5,7,13 –15 Shekarriz and coworkers 16 have evaluated the affected renal function in 17 patients with preoperative and postoperative renal scans after LPN. In two patients with warm ischemic time >30 minutes, the affected renal function decreased at 3 months after LPN. In our patients, recovery of the affected kidney in the RPLPN group was better than that in the TPLPN group, although ischemic time during RPLPN was longer than during TPLPN. Our results also suggest that warm ischemic time of >30 minutes influences postoperative recovery of renal function. To evaluate whether the affected renal function recovers in patients with a long warm ischemic time, we need further evaluation for a long period after surgery.
TPLPN and RPLPN both have advantages and disadvantages. In TPLPN, the control of forceps is easy because of the wide range and unrestrained location of the port site, but cooling of the kidney is difficult. In RPLPN, cold ischemia can be achieved by infusion of cooled materials into the retroperitoneal space, although suturing techniques are difficult. In our cases of LPN, ischemic time in RPLPN was longer than that in TPLPN, even if renal cooling times were excluded. The long ischemic time might have been because of the difficulty of the RPLPN procedure. We performed injection of near-freezing saline from the stopcock of the port that was connected to a pressured infusion bag by a wide irrigation tube. This method provides efficient renal cooling, because cold saline can be rapidly injected while aspirating the saline that has been warmed in the retroperitoneal space. Although some studies have shown that the cold ischemic time limit is 35 minutes after a renal cooling time of about 10 minutes, 11,17 the affected renal function after OPN and RPLPN did not decrease in many of our patients.
Bhayani and associates 7 have shown that a warm ischemia time of up to 55 minutes does not significantly influence long-term total renal function after LPN in patients with a contralateral functioning kidney. In our study, there was no difference in total renal function evaluated by eGFR during OPN, TPLPN, and RPLPN. Based on the affected renal function, however, the recovery after OPN and RPLPN (cold ischemia) was significantly better than with TPLPN (warm ischemia). In patients with a normal contralateral kidney, postoperative renal function evaluated by eGFR might be masked by contralateral renal function. Shekarriz and colleagues 16 have shown that temporary hilar clamping with a mean warm ischemia time of 22.5 minutes results in preservation of renal function in the affected kidney. We also suggest the assessment of affected renal function to analyze the influence of renal ischemia in PN.
Conclusions
Cold ischemia has the advantage of recovery of postoperative affected renal function. If patients have a risk of deterioration of renal function, cold ischemia for avoiding renal damage should be better than warm ischemia during renal hilar clamping. LPN is a safe and effective approach for NSS if the patient and the methods are appropriately selected.
Disclosure Statement
No competing financial interests exist.