
Abstract
Purpose:
To compare direct costs associated with open partial nephrectomy (OPN), laparoscopic partial nephrectomy (LPN), and robot-assisted LPN (RALPN).
Methods:
A meta-analysis of nonoverlapping studies was performed to determine operating room (OR) time, equipment use, and length of stay (LOS) for OPN, LPN, and RALPN. Cost models using cost data obtained from our institution were created, and robotic cost and maintenance were amortized over 7 years. One- and two-way sensitivity analyses were performed to evaluate the effect of changing variables on the cost effectiveness of each approach.
Results:
Seven RALPN, 18 LPN, and 8 OPN data series were identified, comprising a total of 477, 2220, and 2745 procedures, respectively. Weighted mean OR time was 188, 200, 193 minutes; weighted mean LOS was 2.6, 3.2, and 5.9 days for RALPN, LPN, and OPN, respectively. LPN was the most cost-effective approach at a mean direct cost of $10,311, with a cost advantage of $1116 and $1652 over OPN ($11,427) and RALPN ($11,962), respectively. Sensitivity analyses demonstrate that significant decreases in robotic costs are required for RALPN to be cost effective.
Conclusion:
Despite similar OR times, LPN is more cost effective than OPN because of shorter LOS. Because of lower instrumentation costs, LPN is the most cost effective despite a longer LOS than RALPN. RALPN has high cost of maintenance and instrumentation, which is partially compensated by the shorter LOS. Evidence of oncological and functional equivalence to OPN is warranted to determine the future role of RALPN.
Introduction
However, new technologies such as robotics are associated with increased costs and are often implemented without considering clinical benefit or financial burden. For example, LPN has gained momentum since it was first described in 1993, 6 but concerns of added healthcare costs were warranted, given the increased expense of newly developed laparoscopic instrumentation. As a result, we previously showed that the higher cost of LPN surgical equipment is compensated by the decreased length of hospitalization resulting in LPN being a more cost-effective procedure. 7,8 Although the role of RALPN will be better defined after long-term oncological and functional outcomes are established, a cost analysis comparing RALPN to LPN and OPN is prudent to ensure proper healthcare resource allocation, given the increasing incidence of small renal masses and the gaining popularity of robotics in urology. 9,10 In this study, we perform a meta-analysis of published OPN, LPN, and RALPN series and developed a cost-comparison model to determine direct hospital costs of these surgeries.
Materials and Methods
A meta-analysis was performed using PubMed and Medline to identify articles with outcomes for OPN, LPN, and RALPN (Table 1). Data on average tumor size, operating room (OR) time, and length of stay (LOS) were collected. Overlapping studies, studies including hand-assisted laparoscopy cases, and studies that provided only median data values were excluded. For OPN and LPN, literature was limited to contemporary (published since 2000) series to avoid bias against variations in surgical technique. Given the clinical infancy of RALPN, small case series (<20 patients) were excluded to minimize bias from early learning curve. Weighted means for OR time and LOS were calculated and utilized for all cost analyses. For European and Asian series, OR times were used in data analysis but LOS was excluded because of cultural differences in determining timing of discharge. 11 Cost models were created with TreeAge Pro 2009 (TreeAge Software, Williamstown, MA) using hospital cost data (not charge data) obtained from University of Texas Southwestern Medical Center OR administration and billing office. Hospital charge data were not used in our analysis because it incorporates profit margins, which do not directly correlate to resources allocated. We assumed minimal differences in complication rates between procedures. 12 One- and two-way sensitivity analyses were performed to evaluate the effect of varying OR time, LOS, and equipment costs on the cost effectiveness of each approach.
European or Asian studies: LOS was excluded from weighted mean analyses.
Data were reported as median values, so not included.
LOS = length of stay; LPN = laparoscopic partial nephrectomy; NR = not reported; OPN = open partial nephrectomy; OR = operating room; RALPN = robot-assisted laparoscopic partial nephrectomy.
Costs
Hospital costs include OR costs, anesthesia (professional and nursing fees), room and board, medication costs, and laboratory/pathology services. For RALPN, our hospital costs also include the purchase ($1.5 million) and maintenance fee ($150,000/year) for the da Vinci robot (Intuitive Surgical, Sunnyvale, CA). In our cost model, it was assumed the robot would be used across specialties for a total of 300 cases/year over a 7-year period. This case volume (300 cases) was used because it is unlikely that a robot can be used for many more cases on a yearly basis and reduces the bias with respect to low utilization of the robot. Capital equipment is typically amortized over 7 years at our institution as well as at other institutions. Under these assumptions, the robot adds an additional $364,285 per year to hospital cost or ∼$1214 per case.
Certain surgical supplies remain constant for all partial nephrectomy approaches (drapes, suture, and hemostatic agents such as Floseal [Baxter, Deerfield, IL] and Surgicel [Ethicon, Somerville, NJ]). Primary equipment cost determinants for LPN and RALPN include disposable laparoscopic instrumentation such as trocars, Visiport device, suction irrigator, clip appliers, and staplers. In addition, RALPN requires Hot Shears, two large needle drivers, grasper, and forceps, each costing $220 (averaged over 10 uses).
At our institution, OR time is billed at $12.9 per minute or $772 per hour and room and board costs at $508 per night. Average pharmacy and laboratory/pathology costs were direct costs derived from 14 patients who underwent LPN and 16 patients who underwent OPN at the University of Texas Southwestern Medical Center. 7 Average pharmacy costs were $576 for LPN and $837 for OPN; these costs correlated to differences in hospital LOS. Laboratory and other study costs were $609 for LPN and $950 for OPN and included costs for perioperative blood tests, blood bank, chemical analysis of drainage fluid, electrocardiogram, radiography, and others. We used same costs for pharmacy and laboratory studies for RALPN and LPN. Recovery room fee was fixed at $270 based on a representative subgroup of patients. 1 Surgeon and anesthesia professional fees were based on Medicare reimbursement rates for Texas in 2010.
Results
A total of 7 RALPN, 18 LPN, and 8 OPN data series were identified for this study, comprising a total of 477, 2220, and 2745 procedures, respectively (Table 1). Weighted mean OR time was 188, 200, and 193 minutes; weighted mean LOS was 2.6, 3.2, and 5.9 days; and weighted mean tumor size was 2.9, 2.7, and 4.0 cm for RALPN, LPN, and OPN, respectively.
LPN was the most cost-effective approach at a mean direct cost of $10,311 (8543–12,348), with a cost advantage of $1116 and $1652 over OPN ($11,427 [10,521–13,457]) and RALPN ($11,962 [10,238–13,504]), respectively (Table 2).
Given the similarities in OR time, the main determinants of cost for the various approaches were surgical equipment and LOS costs. RALPN surgical equipment was most expensive ($1820), as it was $995 and $1535 more than the cost of LPN and OPN surgical equipments, respectively. The shortest LOS of 2.6 days for RALPN did not overcome its high surgical equipment costs. The longer LOS of 5.9 days for OPN made it more costly than LPN, despite its low surgical equipment costs at $285. RALPN costs also included the additional $1214, which represented the average cost per case required to compensate for the purchase and maintenance of the robot over 7 years.
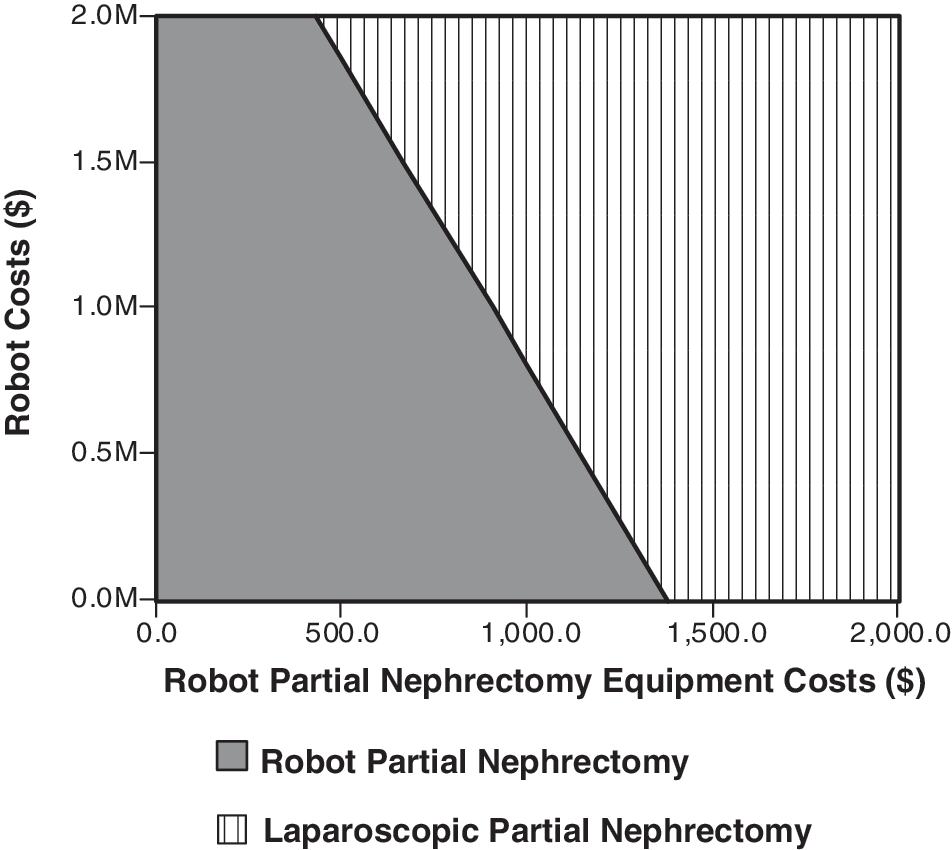
Sensitivity analyses aid in addressing potential targets to improve the cost effectiveness of a procedure. From our study, modifications in robotic costs, surgical equipment, and LOS-related costs could make RALPN and OPN cost equivalent to LPN cost. One-way sensitivity analyses modified one variable at a time to measure its effect on cost and indicated that RALPN is cost equivalent to LPN if OR time is 106 minutes and equivalent to OPN if OR time was 161 minutes. RALPN did not achieve cost equivalence with LPN even if performed on outpatient basis but was cost equivalent to OPN if LOS was 1.6 days. RALPN could be cost equivalent with LPN and OPN if equipment cost decreased to $169 and $1284 per case, respectively. Similarly, OPN is cost equivalent to LPN if OR time is 138 minutes and LOS is 3.75 days. Two-way sensitivity analyses simultaneously modify two variables to measure the effect on cost. For example, if RALPN LOS is 2 days, then RALPN equipment costs would have to be <$500 per case to be cost equivalent to LPN (Fig. 1a). Also, if operative time for RALPN was 120 minutes, then equipments cost of $1544 would result in cost equivalence with LPN (Fig. 1b). Similarly, if RALPN equipment costs were $1250 per case, then purchase and maintenance of the robot would need to be ∼$600,000 to be cost equivalent to LPN (Fig. 2). Figure 3 allows evaluation of cost equivalence of OPN and LPN by varying LOS and OR time for OPN. If LOS of OPN is around 4 days, then OR time would need to be under 180 minutes for OPN to be cost superior to LPN.

Two-way sensitivity analysis: effect of varying robot-assisted laparoscopic partial nephrectomy (RALPN) length of stay (LOS) and operating room (OR) equipment cost (
Two-way sensitivity analysis: effect of varying robotic costs and RALPN equipment cost.
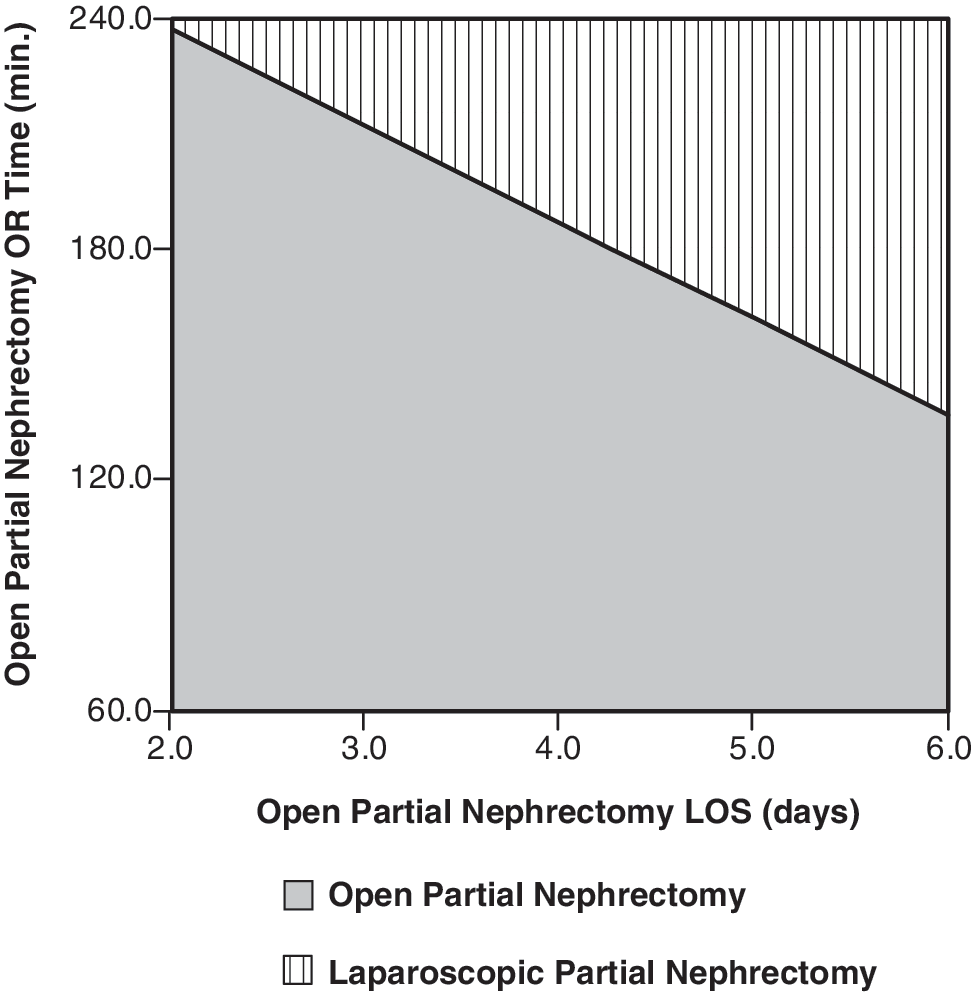
Two-way sensitivity analysis: effect of varying open partial nephrectomy LOS and OR time.
Discussion
Improvement of health outcomes is the primary measure of a new treatment's efficacy. As such, increased costs for a new treatment are warranted if survival or quality of life is definitively improved. However, new healthcare technologies, such as robotics, are commonly implemented into practice without considering clinical benefits or economic consequences. For example, robot-assisted prostatectomy has not shown consistent advantages with respect to functional or oncological outcomes compared to laparoscopic or open prostatectomy. 13 Yet, robot-assisted prostatectomy remains the most commonly performed robotic surgery even though it has the highest hospital cost of any prostatectomy approach. 14 As demand and utilization of robotics continue to increase in urology, 10 it is imperative to assess the cost effectiveness of other robotic procedures to ensure proper resource allocation. RALPN was first described by Gettman et al 15 and has since emerged as a minimally invasive alternative that may reduce the technical difficulties of LPN, but its impact on direct costs has not been evaluated. Here, we provide a meta-analysis of published OPN, LPN, and RALPN series and evaluate direct hospital costs of these surgeries while also providing analyses to address means of cost reduction.
Our study shows that LPN is the most cost-effective partial nephrectomy approach, with a direct cost advantage of $1116 and $1652 over OPN and RALPN, respectively. Although OR times were similar between all partial nephrectomy approaches, LPN was most cost effective because of short LOS and low surgical equipment costs. RALPN had the shortest weighted mean LOS of 2.6 days, but this cost advantage was outweighed by high surgical equipment costs and the additional costs of purchasing and maintaining the robot. OPN had the longest weighted mean LOS of 5.9 days, which made this the 2nd most costly approach despite having the least expensive surgical equipment costs.
For RALPN to become cost equivalent to LPN, a variety of factors must be changed. One-way analyses indicate that RALPN OR time would need to be 106 minutes and equipment cost should be $169 per case to be equivalent to LPN, assuming the other variables were constant. From our meta-analysis, one RALPN series had an OR time of <106 minutes, 16 so this OR time constraint is feasible. However, this OR time was from the smallest RALPN series in our study and could represent a selection bias of less-complicated cases. As is evident from the larger RALPN series, RALPN OR time approximates that of LPN and OPN, which confirms our previous study evaluating the literature that found similar OR times for minimally invasive partial nephrectomy and OPN. 8 Achieving a LOS of 1 day for RALPN is unlikely because current medical practice does not permit RALPN to be done in an outpatient setting. Using the shortest LOS of 2 days in the RALPN literature, RALPN equipment costs would have to be <$500 per case to be cost equivalent to LPN (Fig. 1). Similarly, if RALPN equipment costs were $1250 per case, then RALP cost of purchase and maintenance would need to be ∼$600,000 to be cost equivalent to LPN (Fig. 2). Such decreases in robotic purchase and equipment costs would require continued development of robotic technology and increased industrial competition. Clearly, robotic costs add financial burden to hospitals, which varies depending on the number of robotic cases performed per year. Thus, utilization of robotics should be based on evidence of improved patient outcomes to justify the high costs. If a robot is not available, then LPN is more cost effective than OPN unless decreases in both OPN LOS and OR time are achieved (Fig. 3).
A recent systematic review of the literature suggests that RALPN is technically feasible and offers favorable operative parameters and perioperative oncological outcomes. 17 However, the review fails to demonstrate any advantages of RALPN with respect to renal preservation or long-term oncological efficacy. A recent multi-institutional study showed that RALPN decreased warm ischemia times when compared with LPN, which could indicate potential for improved renal function. 5 A such, a recent international paper by Benway et al 18 attempts to define short-term functional outcomes of RALPN, but there is no mention of time to follow-up, number of patients followed, or a comparative cohort with which to gauge the functional data. The impetus to increase the use of LPN gained significant momentum only after it was shown to have equivalent functional 19 and long-term oncological 20 efficacy as OPN while also being more cost effective. 7,8 Clearly, further studies on defining RALPN effects on renal preservation and long-term oncological outcomes are needed. As some surgeons do not feel comfortable or technically trained in LPN, the application of LPN continues to be low in the United States. It is possible that RALPN will be a way of increasing the utilization of minimally invasive partial nephrectomy when compared with the alternatives of OPN or laparoscopic radical nephrectomy.
RALPN does show therapeutic promise by improvements in convalescence, which is exemplified by our findings that it has the shortest LOS of any partial nephrectomy approach. It has been well documented that LPN decreases blood loss, decreases narcotic requirements, shortens hospital stay, and improves convalescence when compared with OPN. 21 As RALPN is merely an extension of LPN, it is likely that RALPN can provide these same benefits as well. More importantly, RALPN proponents argue that robotics help provide these benefits of minimally invasive surgery to patients when LPN is not always technically feasible by a surgeon. Expanding the use of minimally invasive surgery is a remarkable attribute for robotics, but again the clinical benefits must be truly outlined and understood to warrant the significantly higher costs.
This study does have several limitations. First, our cost model uses data provided from our own institution, which limits the generalizability of the study. Although costs for room and board may differ between institutions based on geography, the similarities of OR times and subsequent OR costs between the various surgeries in this study should minimize some bias from our model's calculations. Second, all RALPN series were performed by skilled laparoscopists at academic centers who have extensive experience in LPN. The costs of RALPN are bound to increase when the procedure is attempted by less-experienced surgeons, potentially making RALPN even more costly than OPN. Third, this study does not include the additional costs of complications, which can increase LOS-related costs. The direct cost of LPN is potentially underestimated in our analysis, because LPN is 1.66 times more likely to result in a postoperative complication and 3.05 times more likely to require a secondary procedure compared with OPN. 4 To assess the financial magnitude of this bias would be difficult, given individual variations in treating complications as well as discerning the extended LOS for these patients. RALPN series show complication rates as high as 11.7% 22 to 15% 23 but these are still not as high as 24.9% and 19.2% reported for LPN and OPN, respectively. 4 As the RALPN series had a smaller weighted tumor size of 2.9 cm compared with 4.0 cm for the OPN series, this might indicate that the RALPN cases were carefully selected, which resulted in fewer complications, shorter LOS, and decreased direct cost. A recent study by Patel et al 24 demonstrated that RALPN for tumors >4 cm had a 26.7% complication rate (4/15), whereas Patard et al 25 showed that OPN for tumors >4 cm had a 23.1% complication rate (30/130). Although the number of RALPN cases are small compared with those in OPN, it is likely that any bias from tumor size effect on complication rates and LOS is minimal. Further, even an expensive complication that costs $10,000 but only occurs 1% of the time adds only $100 to the model. As such, small differences in complication rates would not impact the overall conclusions significantly. Fourth, our model utilized cost and purchase of a single console robot, but dual console robots have been recently introduced with significantly higher costs near $2.2 million. Academic centers are most likely to acquire dual console robots, making RALPN costs higher than that indicated in our analyses. Finally, this analysis was done from the hospitals perspective and does not include other economical healthcare concerns, such as costs passed on to the patient by hospitals or the loss of productivity incurred by longer hospitalizations.
Conclusion
Despite similar OR times, LPN is more cost effective than OPN because of shorter LOS. Because of lower instrumentation costs, LPN is the most cost effective despite a longer LOS than RALPN. RALPN has high costs of maintenance and instrumentation, which are partially compensated by a shorter LOS. Evidence of oncological and functional equivalence to OPN is warranted to determine the future role of RALPN.
Footnotes
Disclosure Statement
No competing financial interests exist.