
Abstract
Background and Purpose:
Ectopic pelvic kidney is a rare congenital anomaly. It carries more risks for obstruction and stone formation than a normal located kidney. The treatment of renal stones in these patients is challenging. We present our experience with laparoscopic pyelolithotomy for treatment of selected patients with large and multiple renal stones in ectopic pelvic kidneys.
Patients and Methods:
After insertion of a ureteral catheter, pneumoperitoneum was achieved by Veress needle, and the kidney was exposed. The renal pelvis was identified, dissected, and opened. The stones were extracted using laparoscopic forceps. The rigid nephroscope was used to extract any caliceal stones. The renal pelvis was sutured, and the stones were removed from the peritoneal cavity. The procedure was concluded after placement of an intraperitoneal drain.
Results:
A total of 11 patients with large renal pelvic and/or multiple stones underwent laparoscopic transperitoneal pyelolithotomy. A transmesenteric approach was used in eight patients while the colon was mobilized off the kidney in three patients. All stones were removed except one that needed Double-J stent placement and one session of shockwave lithotripsy. After one auxiliary procedure, the stone-free rate was 100%. There were no major intraopertive or postoperative complications. Within a mean follow-up period of 23 months, no stone recurrence occurred.
Conclusions:
Laparoscopic pyelolithotomy for large and multiple stones in ectopic pelvic kidneys is a feasible minimally invasive treatment option. The technique allows removal of all the stones without fragmentation, which may decrease the possibility for rapid stone recurrence.
Introduction
The pelvic kidneys present a special challenge during standard endoscopic intervention for stone treatment; ureteroscopy and percutaneous nephrolithotomy (PCNL). Shockwave lithotripsy (SWL) may be considered as a reasonable treatment option for small stones in pelvic kidneys. 5 Alternative approaches are warranted in such conditions, especially during manipulation of large and/or multiple intrarenal stones. Laparoscopy has been used to visualize the kidney and related intra-abdominal structure to achieve safe and correct puncture of the pelvic kidney during PCNL. 6 Laparoscopic pyelolithotomy emerges as an alternative minimally invasive technique for treatment of patients with large, multiple, and branched intrarenal stones in both normally located and ectopic kidneys. 7,8 We present our experience with laparoscopic pyelolithotomy in eleven patients with large or multiple stones in ectopic pelvic kidneys.
Patients and Methods
The patients included in the present study were selected from all patients who were treated for stones in ectopic pelvic kidneys in our department. No patient with concomitant distal obstruction or multiple small stones (<1 cm) were included in this study. The procedure started by cystoscopic placement of an open-tip ureteral catheter under fluoroscopic control. The patient was placed in a Trendelenberg position with the ipsilateral side 30-degrees up for laparoscopic access. Pneumoperitoneum was then initiated using a Veress needle. Two 12-mm laparoscopic trocars were placed: One at the level of the umbilicus and one in the midline, midway between the umbilicus and the symphysis pubis. Another one or two 5-mm trocars were inserted: One at the lateral border of the rectus muscle opposite the lower 12-mm trocar and the other one for retraction and placed at the anterior axillary line, lateral and distal to the last one (Fig. 1).

Drawing shows laparoscopic trocars distribution for a right-sided laparoscopic pyelolithotomy in an ectopic pelvic kidney.
The free loops of the small bowel were moved out of the pelvis, and the site of the pelvic kidney was then localized and evaluated for any adhesions. For right-side cases, the right colon was dissected off the anterior surface of the kidney. For left-side cases, a transmesenteric incision was performed to expose the posterior peritoneal cover of the anterior surface of the kidney. Injection of saline via the open-tip catheter was helpful to identify the site of the renal pelvis. The perirenal fat was dissected to expose the wall of the renal pelvis, which was then incised using both hot and cold scissors.
The stones were removed using laparoscopic forceps and placed in the peritoneal cavity for later removal. In four patients with inaccessible caliceal stones, the rigid nephroscope was inserted via one of the 12-mm trocars into the collecting system through the pyelotomy incision (Fig. 2). In such a case, the CO2 was connected to the nephroscope, and stone forceps was used to remove the stone from the kidney. After removal of all the stones, the renal pelvic incision was closed by 3-0 polyglactin, using running or interrupted intracorporeal sutures.

A rigid nephroscope is introduced under vision via laparoscopic trocar into the renal pelvis.
The stones were then removed from the peritoneal cavity in a piece of surgical glove via a 12-mm port site. A 20F transperitoneal rubber catheter was placed under vision for postoperative drainage, and the procedure was concluded. All patients received a broad-spectrum antibiotic postoperatively and 2 days after open-tip catheter removal. On postoperative day 3, retrograde pyelography was performed before removal of the ureteral catheter, and the tubal drain was removed one day after. On follow-up visits, all patients had plain radiography and ultrasonography examination of the urinary tract.
Results
A total of 11 patients with pelvic kidneys (7 men and 4 women with a mean age of 36 years [range 25–56 y]), underwent transperitoneal laparoscopic pyelolithotomy. A transmesenteric approach was used to expose the posterior peritoneum covering the anterior wall of the kidneys in eight patients. In the other three patients with right-sided kidneys, the bowel was mobilized to expose the kidneys and their pelvises. All procedures were completed successfully without intraoperative complication or conversion to open surgery.
The stone numbers and locations were: Single (renal pelvic) in five (45.5%) patients, two stones (pelvic and caliceal) in two (18.5%) patients, and three stones (pelvic and/or caliceal) in four (36.5%) patients. The stone size averaged 3.9 cm (range 2.8–5.6 cm) in the largest linear diameter on plain radiography. The mean operative time was 164 minutes (118–210 min). The rigid nephroscope was used to extract one or more caliceal stones in four cases.
The renal pelvis was closed using continuous sutures in four patients and interrupted sutures in the other seven patients. Ten (90.9%) patients were totally stone free after laparoscopic pyelolithotomy (Figs. 3, 4). In one patient, a 9-mm residual stone was missed, and the patient became stone free after a session of SWL, 2 weeks after the laparoscopic procedure.

Preoperative plain and intravenous urography in a patient with multiple large stones in an ectopic left-sided kidney.
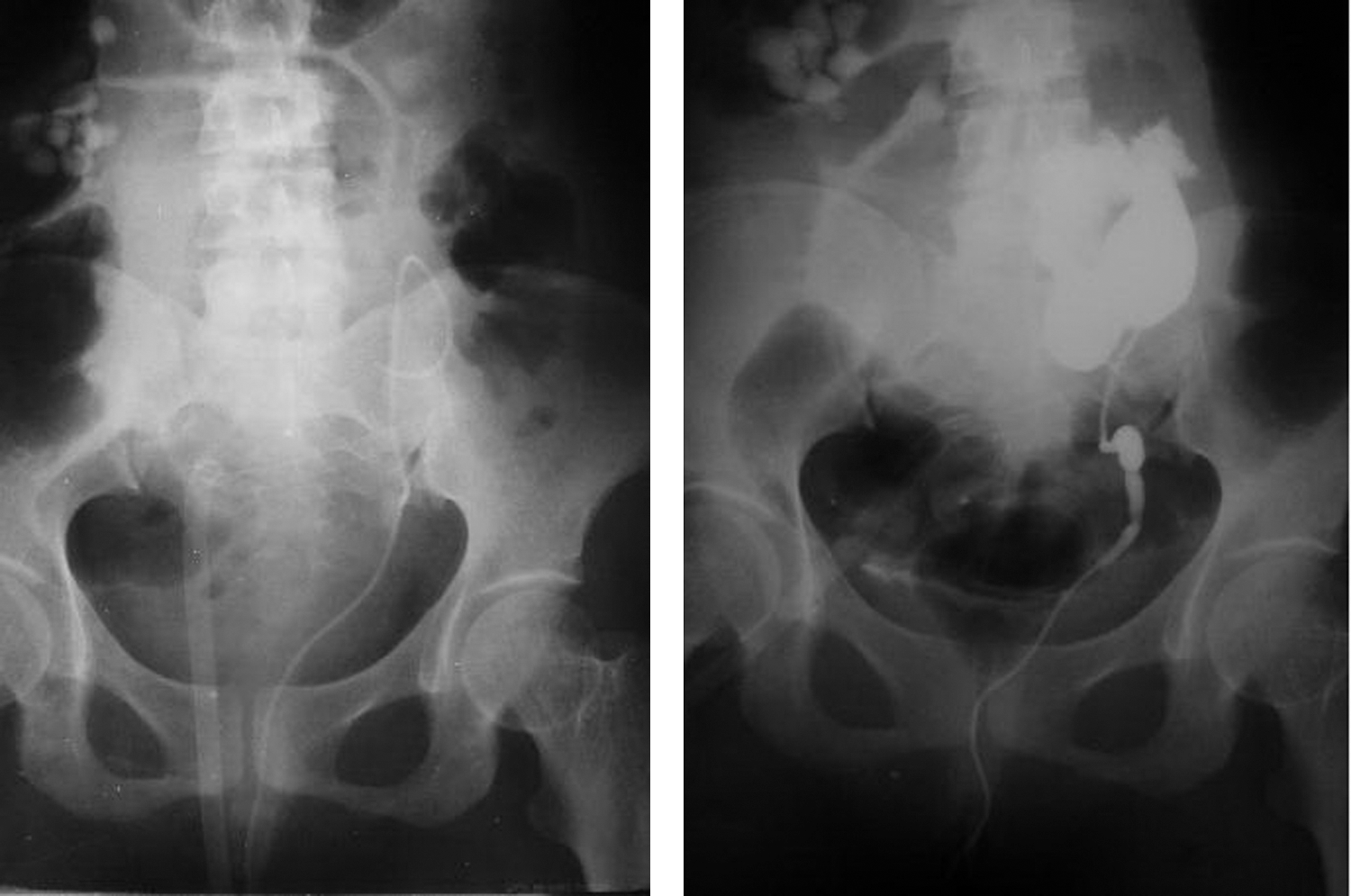
Postoperative plain and retrograde pyelograms for the same patient after laparoscopic pyelolithotomy.
The open-tip ureteral catheter was left for an average of 3.6 days (3–7 d). The mean hospital stay was 4.5 days (range 4–7 d). In two patients, postoperative leakage continued, and in one patient, the ureteral catheter was readjusted under fluoroscopy and left for 3 more days (total of 7 d). In the second patient, the catheter was exchanged by Double-J stent for a subsequent SWL. Within a mean follow-up for 23.7 months (7–38 mos), none of the patients had stone recurrence.
Discussion
Incidence of ectopic pelvic kidney is rare; however, this renal anomaly has higher risks for renal obstruction and stone formation than normal located kidneys. Patients with this condition may need multiple and/or combined endourologic procedures to retrieve their renal stones. This makes open surgery a primary choice to offer a high stone-free rate as well as correction of any associated anomalies in a single procedure. All endoscopic techniques, including laparoscopic approaches, have been described to treat patients with stones in ectopic pelvic kidneys. 8 –11
While SWL enjoys the least invasive approach, it is associated with a significantly lower success rate compared with the rate for normal located kidneys. 1,5 Flexible ureteroscopy is another option, but it is also associated with more technical difficulties because of ureteral kink. 3,12 Percutaneous renal surgery, either alone or with laparoscopic assistance, is the most commonly used technique for treatment of patients with stones in ectopic pelvic kidneys. Although the stone free-rate is acceptable after PCNL in ectopic kidneys, the technique is not free of difficulties and complications that are specifically related to the access. These complications include potential nerve damage. 3,8
Laparoscopy is gaining more roles in management of urinary stone disease. The transperitoneal approach is the most feasible in cases of ectopic pelvic kidneys to keep eyes on related structures and abnormal vessels. Access to the kidney may be achieved by mobilizing the ipsilateral colon or via a transmesenteric incision. 8 In the present study, we preferred to mobilize the colon in right-sided cases, which was easy and allowed good exposure to the whole kidney with no need to use an extra trocar for retraction of the bowel during the subsequent rest of the procedure. In left-sided cases, we chose to proceed via the mesentery with caution, not to injure any significant vessels. The transmesenteric access gave faster exposure of the kidney without complication, and it has become our preferred technique. The endoscopic magnification and low intra-abdominal pressure (10–15 mm Hg) allow identification and avoidance of any pulsating vessels in the mesentery, especially in patients with average body build.
Incorporating laparoscopic and endourologic techniques offers higher efficacy with the advantages of minimally invasive surgery for patients with stones in abnormal kidneys. In the present report, 11 patients with large pelvic and caliceal stones in ectopic pelvic kidneys were treated successfully using laparoscopic pyelolithotomy. In four patients, the rigid nephroscope was used through a 12-mm laparoscopic port to extract the stones from the renal calices. A similar technique has been reported in two separate series in which both a flexible and rigid nephroscope were used with laser to fragment and retrieve intrarenal stones during laparoscopic pyelolithotomy in ectopic pelvic kidneys. 8,9 Both authors used a nephroscope in a classic way allowing irrigation fluid to flow freely into the peritoneal cavity. This fluid is expected to be a limiting factor during the remaining part of the laparoscopic procedure. Also, it would be difficult to aspirate it all at the end of the procedure. Nadu and associates 9 suggested putting the patient in a head-down position for 2 minutes and aspirate the fluid from underneath the diaphragm.
In the present report, we have used CO2 instead of the irrigation fluid via the nephroscope and the stone forceps to extract the stones from the dilated calices. While this would alleviate any expected postoperative intraperitoneal fluid collection, it might “theoretically” mask small stones during fluoroscopic examination. As such, complete preoperative radiologic data about the stone burden would help to ensure stone-free status during laparoscopic pyelolithotomy. Also, there will be a potential risk of gas embolization during use of CO2 via the nephroscope. Using our technique, however, the incision in the renal pelvis is much wider than the nephroscope, which allows free escape of the CO2 into the peritoneal cavity. As such, no gas tension is expected to occur within the kidney. Also, the process of searching for caliceal stones is too short when compared with any fragmentation process and is performed within a noninjured collecting system, which would protect against any CO2 embolization.
The overall results of the laparoscopic approach for management of large and complex renal stones are satisfactory. 9 –11 In the present report, the immediate stone-free rate after laparoscopic pyelolithotomy was 90.9% and reached 100% after one session of an auxiliary procedure (SWL). The technique seems ideal for ectopic kidneys, because it allows handling of the kidney under vision, similar to open surgery, and avoids trauma to the renal parenchyma. Also, a concomitant correction of an associated ureteropelvic junction obstruction can be achieved. 9 More effort is needed, however, to decrease operative time and determine the best way to close the renal pelvis, and determine the type and time of ureteral stent placement. Also, a comparative study with other standard laparoscopic guided PCNL using laser and a flexible nephroscope to treat patients with stones in the ectopic kidney will be warranted.
The mean operative time is still high in comparison with the other minimally invasive modalities. In the present series, the mean operative time was 164 minutes, including the initial cystoscopic part of the procedure. The renal pelvis was closed with 3-0 polyglactin sutures using a continuous method in seven patients and interrupted sutures in four patients. There was no difference from the technical point of view, and either way could be used based on surgeon preference. We elected to use an open-tip catheter as a postoperative ureteral stent to be removed on postoperative day 3 if there was no leakage. This stent worked well in nine patients, while in one patient, the catheter slid down the ureter, resulting in persistent leakage that stopped by readjusting the stent under fluoroscopy. The use of a suitable size and length of Double-J stent would be better after laparoscopic pyelolithotomy. A special design of Double-J stent may be needed, however, to avoid a long segment of the stent within the urinary bladder. In another case with a residual 9-mm caliceal stone, the stent was replaced by a Double-J stent for subsequent SWL.
Removal of the stone as one piece is better than in fragments, especially in kidneys with anatomic configuration that may hinder spontaneous clearance of the stone fragments. Any residual fragment may constitute a nucleus for stone growth, infection, and recurrence. Interestingly, recurrence of stones after laparoscopic-assisted PCNL with a mean follow-up period of 27 months occurred in two of five patients in the series by El-Kappany and associates. 8 Laparoscopic pyelolithotomy with or without nephroscopy allows removal of most of the stones in large sizes and decreases the need for intracorporeal lithotripsy. In the present series, all the patients had one or more large pelvic stones with proximal caliceal dilatation that allowed removal of the caliceal stones without need for lithotripsy. Within a mean follow-up period of 2 years, none of the patients had stone recurrence.
Conclusions
Laparoscopic pyelolithotomy for treatment of patients with large and multiple stones in an ectopic pelvic kidney is feasible. The technique is associated with a high stone-free rate and without any major intraoperative or postoperative complications. Both rigid and flexible nephroscopes can be used via the laparoscopic trocar to help in extracting nonaccessible caliceal stones. Removal of the stones without fragmentation decreases chances of residual fragments and may decrease the chances of rapid stone recurrence. The rarity of the condition limits the possibility for running a randomized study on a large group of patients to reach a more solid statement in this regard.
Footnotes
Disclosure Statement
No competing financial interests exist.