
Abstract
Background and Purpose:
Robot-assisted laparoscopic radical prostatectomy (RALRP) is the most expensive, yet most common, surgical treatment for patients with prostate cancer. Furthermore, its popularity continues to grow despite the lack of evidence for functional and oncologic superiority over other treatments. As a result, we modified operating room (OR) processes to determine if the times and costs that are associated with RALRP in an academic setting could be reduced.
Patients and Methods:
Four modifications in OR processes were implemented: Trainee adherence to time-oriented surgical goals; use of a dedicated anesthesia team; simultaneous processing by nursing and urology house staff during case turnover; and identification and elimination of unused disposable instruments. Total surgical, anesthesia, and OR turnover times were measured. Payroll, surgical supply, OR time, and anesthesia costs were also measured. One hundred RALRP cases before and after the modifications were implemented were compared.
Results:
Patients undergoing RALRP were similar both before and after the modifications were implemented. Total surgical, anesthesia, and turnover times were reduced by 17.4 (6.8%, P=0.041), 4.5 (19.1%, P=0.006), and 12.1 (28.1%, P=0.005) minutes, respectively. Payroll, surgical supply, and OR costs were reduced by $330 (25%), $609 (15.7%), and $1638 (27.7%), respectively. There was no fiscally significant change in anesthesia costs.
Conclusions:
Using simple modifications, it is possible that RALRP efficiency can be improved by decreasing its associated times and costs. These modifications were implemented in an academic setting but may be used in any institution. These modifications represent an initial attempt to improve RALRP cost-competitiveness with other treatment modalities.
Introduction
There are several factors that increase the costs of RALRP. These include capital expenses, surgical supplies, and increased operative times. 9 The latter may be because of the additional complexity in both the amount of equipment and the steps to set up the OR. Furthermore, the training requirements and frequent turnover of trainees in urology and anesthesia may increase operative times in academic settings. Because the use of RALRP is expensive, yet continues to grow, there is a need to improve its cost-competitiveness. While the capital expense and service contract associated with RALRP are generally fixed, the efficiency with which the robot is used on a day-to-day basis is variable. In this study, we implemented simple modifications in OR processes to determine whether the times and costs associated with RALRP could be reduced.
Patients and Methods
At our institution, RALRP has been performed since October 2005. A second robot was purchased in November 2007. RALRP was performed using a previously described technique 10 with one of two systems—the da Vinci or the da Vinci S model (Intuitive Surgical Inc, Sunnyvale, CA). With the collaboration of the departments of urology, anesthesiology, nursing, and the OR support staff, four modifications in OR processes were implemented between February and April 2009. The 100 consecutive RALRP patients before (pre-February 2009) and after our modifications (post-April 2009) were compared.
Modifications
First, surgical trainees (senior resident, fifth or sixth year, or fellow) and attending urologists agreed to adhere to time-oriented goals for each portion of an RALRP case (Fig. 1). For example, a specified amount of time was allotted for individual steps, such as dissection of the seminal vesicles. If a particular step of the case was not completed by the trainee within 60% of the maximum amount of time (ie, the checkpoint) for that step, the attending surgeon would operate until the case could be brought back to schedule. The proportion of 60% per step for trainees was chosen based on their level of training (which tended to be senior residents or fellows, because more junior trainees might have needed longer precluding timely completion of an RALRP) and the educational needs of the trainee, as perceived by the attending urologists.
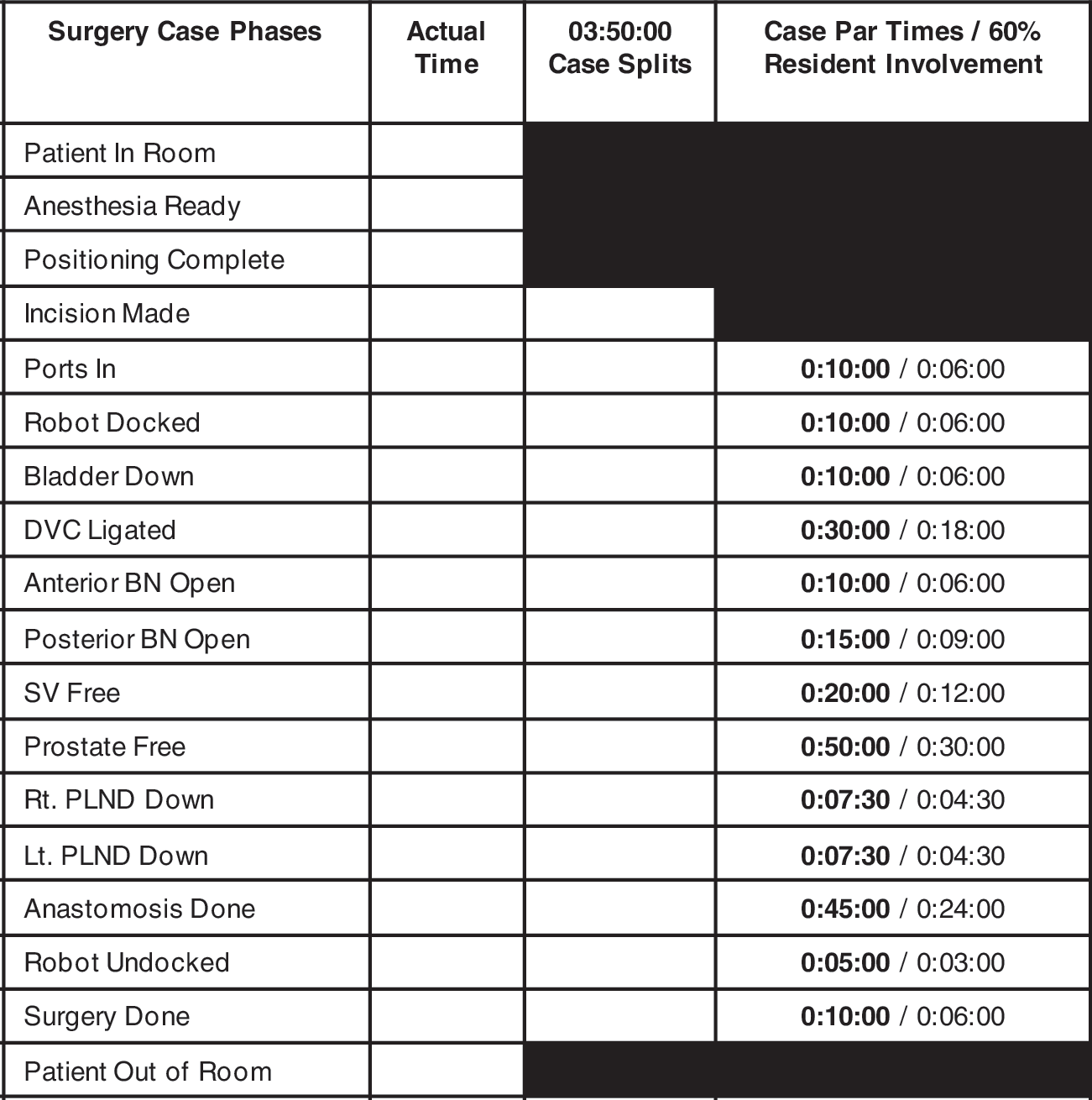
Time-oriented goals for each portion of robot-assisted laparoscopic radical prostatectomy. In this model, a maximum amount of time was assigned to individual surgical steps. For each step, the trainee was allowed to operate for up to 60% of the maximum time. If the trainee was able to complete the step within this limit (ie, the checkpoint), he was allowed to continue to the next step. If not, the attending urologist would replace the trainee at the console until the case could be brought back to schedule. For example, a maximum time of 20 minutes is allotted for dissection of the seminal vesicles. If the trainee completed this step within 12 minutes, he would continue on to the posterior dissection. This model allows for a total surgical time (measured from the time the port incisions were made to the time when the ports sites were closed) of 230 minutes, 135 minutes of which was trainee time. DVC=dorsal venous complex; BN=bladder neck; SV=seminal vesicles; PLND=pelvic lymph node dissection.
Throughout the study, the bedside assistant was either a separate resident (junior, either second or third year) or dedicated surgical nurse assistant (who only participated during the cases that took place during the last month of the study, October–November 2009). The bedside assistant's roles included: Retraction, suction and irrigation, Foley catheter manipulation, placement of pedicle clips, and retraction of sutures during the anastomosis. Neither junior resident nor nurse assistant participated at the console. This arrangement allowed the surgeon and the trainee to swap out from the console without having to rescrub to assist at the bedside.
Second, a dedicated group of four anesthesiologists and four certified registered nurse anesthetists were identified. These persons were experienced with RALRP and facilitated fast turnover time. They were scheduled with regularity on robotic cases to reduce variability and increase experience with the unique elements of patient positioning and robot setup involved in preparing for RALRP.
Third, nursing and urology house staff sped OR turnover by performing tasks simultaneously. For example, nursing staff opened supplies for a subsequent case at the same time the patient was brought into the OR. Previously, house staff members were allowed to bring the next patient to the OR only after all the instruments were opened and ready to be used.
Fourth, nursing and urology house staff endeavored to identify and eliminate unused disposable equipment. These included attempts to eliminate both robot-specific and general supplies, including the elimination of a third robotic needle driver, a second suction-irrigator device, and irrigation saline. Of note, robot-assisted surgery had been performed within the institution since 2006, so the initial learning curve of the RALRP had taken place already.
OR times
Three nonoverlapping measures of OR duration were measured that corresponded to three of the implemented modifications (described above): (1) surgical time (measured from the time the port incisions were made to the time the ports sites were closed); (2) anesthesia time (measured from the time the patient entered the room to the time the anesthesia team was ready for positioning); and (3) turnover time (measured only on days during which two RALRP cases were performed using the same robot in the same OR; measured from the time the first RALRP case left the OR to the time the second RALRP case entered the OR).
OR costs
Four categories of OR costs were assessed: Payroll, surgical supplies, OR time, and anesthetic costs. For the payroll, surgical supplies, and anesthetic categories, direct costs were measured. Direct costs represented those expenses that were generated by each of these departments while providing care necessary to perform a specific RALRP. The capital expense of purchasing the robot and the cost of the annual service contract were not included, because these would not be influenced by our modifications in OR processes. OR time cost was based on the indirect costs of building and equipment depreciation. These were used to calculate the expense of running the OR itself per unit of time that would be influenced by our modifications. This cost was based on the time the OR was actually in use and thus incorporated only surgical and anesthesia times, but did not incorporate turnover time. As well, only hospital costs, not patient charges (ie, billings) were measured.
Statistical analysis
The Student t test and Pearson chi-square or Fisher exact) tests were used to compare continuous and categorical variables, respectively. SPSS™ (IBM, Illinois) was used to perform the analyses.
Results
A total of 200 RALRP cases were reviewed: The 100 cases before the modifications took place over a 6-month period (August 2008–January 2009) and the 100 cases after the modifications took place over an 8-month period (April–November 2009). The patient groups were similar in age, body mass index, prostate-specific antigen level, Gleason score, stage, and prostate size (Table 1). They were also similar across other factors related to surgical time and costs, including whether a nerve-sparing procedure and/or pelvic lymph node dissection was performed. Furthermore, the positive surgical margin rate was also similar between the groups (11.8% vs 10.4%, P=0.761, before and after the modifications, respectively).
BMI = body mass index; PSA=prostate-specific antigen.
Times
After implementation of the case checkpoint system, the mean total surgical time was reduced from 256.2 to 238.8 minutes, indicating a 6.8% reduction (P=0.041). We did not, however, demonstrate a change in the proportion of RALRP cases being completed within the 230-minute checkpoint system total surgical time. With the implementation of a dedicated anesthesiology team, there was also a reduction in mean anesthetic time from 23.7 to 19.2 minutes, indicating a 12.1% reduction (P=0.005) (Table 2).
Among the 200 cases, 110 took place on days during which 2 RALRP cases were performed on the same day (ie, 55 days of 2 cases per day). As a result, 55 observations of turnover time were available for review. Among these, 26 and 29 two-case days were identified before and after the simultaneous nursing and urology house staff modification was implemented, respectively. For these, there was a reduction in turnover time from 43.0 to 30.9 minutes (P=0.005).
Costs
The comparison of each cost category before and after the modifications were implemented is reported in Table 3. After the implementation of all modifications, we noted a reduction in costs for all categories except anesthesia costs, which increased slightly from $696 to $725 per case, indicating a 4.2% increase. For the remaining categories, costs were reduced by $1638, $609, and $330 for OR, surgical supplies, and payroll costs, respectively. The total cost reduction was $2548 (21.7%). The OR time savings of 21.9 minutes (17.4+4.5 minutes, for surgical and anesthetic time reductions, respectively) and associated cost savings of $1638 correspond to $74.8 per minute of OR time saved.
All costs are reported in US dollars.
Discussion
The objective of this study was to determine whether simple modifications in OR processes would be able to improve the times and costs that are associated with RALRP. We demonstrated that both of these measures could be reduced by implementing modifications in the OR that aim to improve efficiency. In this study, these modifications were: Adherence to a time-oriented case checkpoint system among surgical trainees and attending urologists; use of a dedicated anesthesia team for all RALRP cases; simultaneous processing by nursing and urology house staff during case turnover; and identification and elimination of unused disposable equipment. While this study demonstrated these approaches in an academic setting, we believe that any (or all) of these modifications can be easily implemented in other institutions as well.
While our surgical times are long (both pre- and postmodification), they represent two separate endeavors: Treatment of the patient and teaching of the surgical trainee. Still, our surgical times are consistent with previously reported data. 3,11 By implementing a time-oriented case checkpoint system, we reduced the total surgical time by more than 17 minutes. This reduction was statistically significant, but we also believe it to be clinically significant. There are two reasons for this. First, it represents an improvement in surgical time while preserving the commitment to surgical trainees. A surgical trainee participated at the console in all 200 RALRP cases in this study. In our training program, senior residents had participated in approximately 20 to 30 RALRP cases as the bedside assistant before their involvement on the console. Before the implementation of our modifications, the involvement of the trainee at the console was nonstandardized and varied. During that period, the exact time the trainee spent on the console was not measured, but at no point did a trainee complete an entire RALRP case. Subsequent to the modifications, the involvement of the trainee was standardized and regimented.
Second, a reduction in surgical time was also reflected by a reduction in OR costs. Indeed, the largest reductions in costs after these modifications were implemented were seen in the category of OR costs, which were reduced by $1638 (or almost 28%). We believe that modest differences in surgical times should not be discounted, because they may represent significant cost savings. Furthermore, savings in time allow for additional procedures to be performed in the same OR that would have otherwise remained unused and thus its associated costs are offset by an additional source of income.
After using a dedicated group of anesthesiologists for all RALRP cases, we observed a reduction of more than 19% in the time needed for them to prepare the patient. We defined anesthesia time as the duration between the time the patient enters the room to the time anesthesia is complete and the patient is ready to be positioned. To our knowledge, this is the first study to describe this in the RALRP literature. We believe that using a core group of anesthesiologists improves familiarity with anesthetic considerations that are unique to RALRP, such as steep Trendelenberg positioning and intraoperative monitoring during laparoscopy. Such familiarity should lead to increased speed and efficiency.
Our study is also unique by describing case turnover time data. These data are not a direct surgical measure but are an important element of OR efficiency, nonetheless. By instituting simultaneous nursing and urology house staff processing of patients, this modification was able to reduce the time between same-day consecutive RALRP cases by more than 12 minutes (28.1%). We believe that this reduction will also be reflected in reduced OR costs. Before our modifications, the second RALRP case was brought to the OR only when cleaning was completed and all surgical supplies were opened and ready to be used. With the assistance of the nursing staff, this procedural protocol was changed to allow subsequent patients to be brought to the OR as soon as the cleaning staff had processed the room, but before all equipment had been opened. Successful collaboration with nursing and OR administration was critical to implementing this modification. Of note, there were no instances of cancelled cases because of insufficient equipment supplies that may have been recognized only after the patient was in the room and the anesthetic initiated.
Overall, our surgical costs are higher than those previously reported, 6,7,12 especially given that we only included costs associated with providing surgical services. We did not include, for example, the costs of postoperative hospital stay, because we only included costs that we believed would be influenced by the modifications implemented. We did, however, demonstrate a reduction in the costs associated with RALRP after the implementation of our modifications. The most significant cost savings were observed in the domain of OR costs. OR costs were the greatest expense in performing RALRP, and this is consistent with other studies, 6,12 which also show that OR costs account for the greatest proportion of those incurred when offering RALRP.
The next most significant cost savings were seen in the reduction of surgical supplies ($609 or 15.7%). We attribute this directly to our modification of identifying and eliminating unused and/or unnecessary disposable supplies. A major component of this was the elimination of general equipment, such as unused irrigation fluid and surgery-specific tools such as a laparoscopic vascular stapler for the dorsal venous complex. The reduction observed in payroll costs we attribute to the reduction in total surgical time and turnover time. Interestingly, we did not observe a reduction in anesthetic costs but noted a nominal increase of $29 (4.2%) per case. We do not believe this amount is fiscally significant.
This study used modifications to improve the times and costs of performing RALRP. The modifications used in this study were not chosen arbitrarily but were based on needs that were identified by all three participating groups—the departments of urology, anesthesia, and nursing. Because the most significant costs of RALRP are generally fixed (eg, the capital expenses of the robot purchase and service contract), we chose to modify processes and procedures related to the daily use of the robot that remain variable. Enacting a time-oriented case checkpoint system allowed us to preserve the role of education in our institution. As well, incorporating the roles of anesthesiology and nursing in processing patients during anesthetic preparation and turnover between cases is a critical element in evaluating surgical efficiency in modern ORs.
Our four modifications aimed at increasing RALRP efficiency are only a few of several possible strategies. Using the expense of operative time, Steinberg and associates 9 described the costs of learning RALRP and found that the average learning curve was 77 cases and cost $217,034. Any approach to shorten the learning curve will increase efficiency, because previous experience with laparoscopy or RRP has been shown to do this. 13 While we used a time-based system for trainees, Rashid and colleagues 14 used a scoring-based system in their study of resident RALRP training that showed that trainees improved their scores over time. Several training programs have been described for robot-assisted surgery in different specialities. 15 Preclinical training with animal models may also be beneficial. In an animal-based study, Hanly and coworkers 16 showed that preclinical animal training with same-member health-care teams led to progressively improved setup times and decreased operative times. They also reported that while the cost of animal training was $10,355, by delaying clinical use of the robot, they were able to save $52,895.
Our study is not without limitations. First, all four of our modifications were implemented at approximately the same time. As a result, we cannot attribute with accuracy reductions in times or costs to individual strategies. Second, while it is possible that the improved surgical times may be a reflection of the greater experience of the surgeon acquired over the duration of the study, we believe that this is less likely. RALRP has been performed in our institution since October 2005, but our study only included patients from August 2008. As such, we believe that the learning curve of the attending surgeon had already taken place. Third, we do not report long-term follow-up data for these patients. As a result, we cannot comment on whether RALRP patients after the modifications suffered poorer functional or oncologic outcomes that might nullify the immediate improvements in efficiency documented in this study. We do note, however, that surgical margin rate did not appear to be adversely affected. Fourth, while we report our own hospital costs, it is recognized that costs may vary considerably, depending on institution and geographical location. 12 Finally, while our study does not suggest cost-competitiveness with other surgical approaches, such as LRP or RRP, it does show that cost and time reductions are possible.
Conclusions
Because RALRP is the most common form of surgery for prostate cancer, yet remains the most expensive, there is a need to improve its efficiency. This study demonstrated that using simple modifications in OR processes, the times and costs associated with day-to-day use of RALRP may be reduced. Such modifications can be implemented in any hospital setting. This study represents only an initial attempt at lowering the costs and improving the efficiency of RALRP. Integration of multiple departments is critical to achieve success in this regard.
Footnotes
Disclosure Statement
Dr. Nadler is a consultant/advisor for Intuitive Surgical. The other authors have no conflicts of interest to declare.