
Abstract
Purpose:
To comprehensively review the available evidences in the literature on the use of laparoscopic pyeloplasty (LP) vs open pyeloplasty (OP) for the repair of ureteropelvic junction (UPJ) obstruction in children.
Materials and Methods:
Published studies until the end of October 2010 were searched from Medline, Embase, Web of Science, Ovid, and Cochrane databases. The literature search, quality assessment, and data extraction were independently performed by two reviewers. A systematic review and meta-analysis were performed by using Review Manager 4.2.8 software.
Results:
Of 1403 studies, one randomized controlled trial (RCT), two prospective comparative studies, and six retrospective observational studies were eligible for inclusion criteria, comprising 694 cases of LP and 7334 cases of OP. The OP has significantly reduced operative time (weighted mean difference [WMD]=59.00; 95% confidence interval [CI]=41.15 to 76.85; P<0.00001) and higher stent placement rate (odds ratio [OR]=5.97; 95% CI=3.17 to 11.26; P<0.00001) compared with LP, whereas the duration of hospital stay was shorter in the LP group (WMD=−0.40; 95% CI=−0.77 to −0.03; P=0.03). No difference was observed between LP and OP regarding complications (OR=0.78; 95% CI=0.46 to 1.34; P=0.37) or success rate (OR=1.76; 95% CI=0.71 to 4.36; P=0.22).
Conclusions:
LP is a minimally invasive, safe, and effective therapy method for UPJ obstruction in children, with shorter hospital stay and excellent outcomes, and without additional risk of postoperative complications. Because of the publishing bias, a series of RCTs are necessary to explore the efficiencies of LP in the management of UPJ obstruction in children.
Introduction
Although the laparoscopic approach has developed worldwide and become a preferred method for UPJ obstruction repair, 6 particularly in adults, 7 it has not yet reached the same degree of popularity among pediatric urologists. Currently, the selection of pyeloplasty approach in children with UPJ obstruction is mostly based on the surgeons' discretion and experience. Nevertheless, the growing experience with reconstructive urologic procedures, combined with the perceived decreased invasiveness, has led to an increasing use of LP for UPJ obstruction in children. 8,9
Despite a large number of studies that have been performed in patients with UPJ obstruction, the true effectiveness and potential advantages of LP in children remains controversial, and many published studies in this field deal with a small series of patients. Therefore, we systematically reviewed the literature and performed the present meta-analysis to assess the effectiveness and potential advantages of LP in relation to conventional OP in the treatment of children with UPJ obstructions. The current study was undertaken from March 3, 2010, to October 28, 2010; during the study period, new published articles were also evaluated.
Materials and Methods
Literature search
Because the current study was a
Study selection criteria
Because of the paucity of available evidence that addressed the study question, our search was not restricted to randomized controlled trials (RCTs). Controlled clinical trials and comparative studies (including case-matched studies) were included as well. Although no language restrictions were imposed initially, the search was limited to studies published in the English language for the full-text review and final analysis. Eligibility criteria included all available studies that compared LP with OP for the repair of UPJ obstructions in the pediatric population and with quantitative data on outcome parameters. The pediatric population was defined as age younger than 18 years when the patient underwent LP or OP.
During our literature search and selection, the articles were excluded if the range of patients' age was beyond 0-18 years, or they did not provide sufficient data for calculation of a quantitative aggregation in children. Only the standard LP was considered; LP with hand or robot assistance or laparoscopic single-site pyeloplasty was not included. Meanwhile, conference abstracts were excluded because of the limited data presented in them. The citations, abstracts, and full text of all potentially relevant studies were independently evaluated and selected by two reviewers (MH and TQS), and any disagreements were resolved by consensus.
Quality assessment of included articles
Each included article was appraised by two reviewers (MH and TQS), who assessed the methodologic quality of selected studies independently. A critical review checklist of the Dutch Cochrane Centre was used to appraise the RCTs (
Data extraction and analysis
Two reviewers (MH and TQS) independently assessed selected studies, and extracted and tabulated data from each article with a predefined data extraction form. Data regarding the following factors were considered: Study methodology, participant features, intervention characteristics, definition of complications, and outcome measures. Outcome parameters for assessment were operative time, postoperative complications, duration of hospital stay, success rates, and stent placement rates. Studies with insufficient data for use in odds ratio (OR) analysis and 95% confidence interval (CI) or studies not providing adequate data to obtain mean values and standard deviation (SD) for continuous variables were excluded from the relevant calculations.
Statistical analysis
Meta-analyses were performed for the five primary outcome parameters: Operative time (in minutes), postoperative complications (in events per group), duration of hospital stay (in days), success rate (in events per group), and stenting rate (in events per group). The Review Manager 4.2.8 software (The Cochrane Collaboration, Oxford, UK) statistical package was used to analyze the ORs for dichotomous variables and weighted mean differences (WMDs) for continuous variables. The fixed effect models were used to identify heterogeneity between the studies, and statistical heterogeneity was assessed via the I 2 index. P values of<0.05 and I 2 <30% were considered to indicate statistical significance, respectively. The CI was established at 95%. The presence of publication bias, if any, was evaluated using funnel plots.
Results
Characteristics of retrieved evidences
The initial search strategy retrieved 1403 publications from all above databases using the key words “pyeloplasty” and “ureteropelvic junction obstructions.” After screening all titles and abstracts, the number of studies was reduced to 48 by limiting the inclusion criteria as comparative studies regarding LP and OP. After independent review, eight articles were excluded because of unavailability of the surgical data in LP or OP groups, and nine were excluded because they were review articles and did not allow the calculation of outcome parameters. Eleven articles were excluded because they did not provide sufficient data to perform a quantitative analysis, and four were excluded because the same authors published several reports on the same patients, and only the best-quality study was considered.
Finally, 16 publications dealing with comparison of standard LP (without hand or robot assistance) and OP for the management of UPJ obstruction were retrieved for more detailed evaluation. 9 –24 Of these publications, three were excluded because the surgical procedures were undertaken in adults 11,16,20 ; four were excluded because they were difficult to calculate the quantitative aggregation in children. 14,19,22,23 Subsequently, nine full articles were considered to be eligible for inclusion in the analysis, including one RCT, two prospective comparative studies, and six retrospective observational studies (Fig. 1). The full period for investigation and data extraction was from March 3, 2010, to October 28, 2010. A summary of the studies' methodology, participant features, intervention characteristics, measured outcomes, and the use of stents and drainage is provided in Tables 1 to 4.
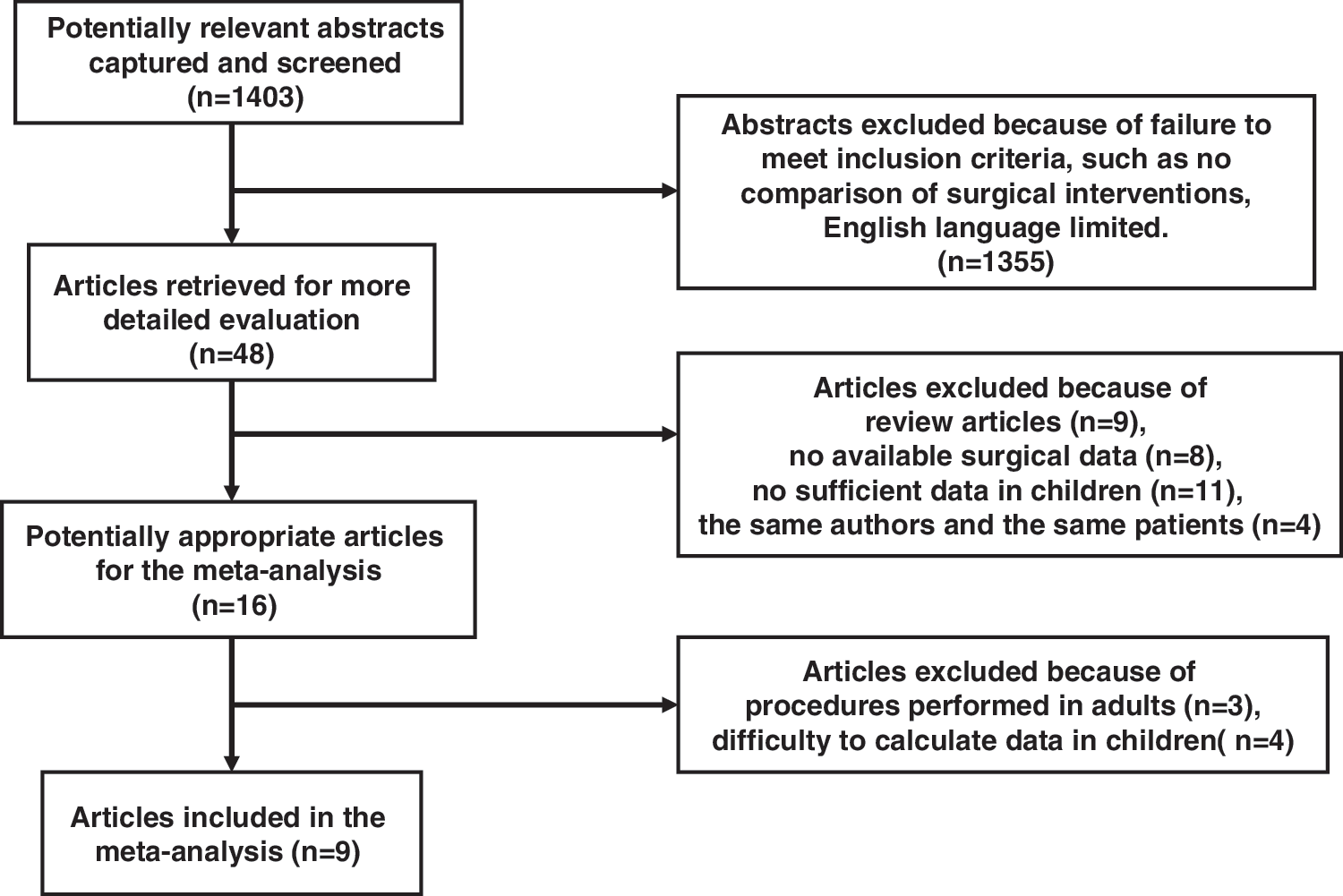
Article selection flowchart.
Flank incision in 42 and dorsal lumbotomy in 25.
97.2±36.0 for flank incision and 87.6±34.8 for dorsal lumbotomy.
The total number in two groups: left 20, right 11.
LP, infant (1 month–2 years), 2.2±2.6; preschool (2–6 years), 2.3±2.2; grade school (6–10 years), 2.4±1.7; preadolescent (10 –13 years), 2.0±1.0; adolescent (13 to <19 years), 2.1±1.2.
OP, infant (1 month–2 years), 2.1±2.1; preschool (2 –6 years), 2.2±1.9; grade school (6 –10 years), 2.3±1.3; preadolescent (10 –13 years), 2.4±1.5; adolescent (13 to <19 years), 3.0±1.8.
LP = laparoscopic pyeloplasty; OP = open pyeloplasty; PHIS = pediatric health information system; M = male; F = female; L = left; R = right; RCT = randomized controlled trial; B = bilateral; NA = Nonavailable.
42 for flank incision and 25 for dorsal lumbotomy.
144 for flank incision and 148 for dorsal lumbotomy.
3.6 for flank incision and 3.3 for dorsal lumbotomy.
LP, infant (1 month–2 years), 2.2±2.6; preschool (2 –6 years), 2.3±2.2; grade school (6 –10 years), 2.4±1.7; preadolescent (10 –13 years), 2.0±1.0; adolescent (13 to<19 years), 2.1±1.2.
OP, infant (1 month–2 years), 2.1±2.1; preschool (2 –6 years), 2.2±1.9; grade school (6 –10 years), 2.3±1.3; preadolescent (10 –13 years), 2.4±1.5; adolescent (13 to <19 years), 3.0±1.8.
Retro=retroperitoneal; Trans = transperitoneal.
Including pyelonephritis.
Including abdominal wall palsy and ileus.
49 for flank incision and 47 for dorsal lumbotomy.
UL = urinary leakage; WHO = worsening of hydronephrosis; SI = stenosis infection; UTI = urinary tract infection; WI = wound infection.
Salle type stent.
42 for flank incision and 25 for dorsal lumbotomy.
29 for flank incision and 25 for dorsal lumbotomy.
All 13 for flank incision.
The number of nephrostent or Double-J stent.
Pyelostomy transanastomotic stent.
Characteristics of patients
One RCT, two prospective comparative studies, and six retrospective observational studies were eligible for inclusion criteria and selected for this analysis, comprising 694 cases of LP and 7334 cases of OP in the pediatric population. A description of patients in the two groups is summarized in Table 1. Meta-analysis was performed for age in the two comparative arms, and only two studies with sufficient data to obtain mean values and SD for continuous variables were included for the relevant calculations. 13,15 As shown in Fig. 2, the results revealed that the mean age of LP was significantly older by 50.90 months (WMD=50.90; 95% CI=41.23 to 60.58; P<0.00001), but with unacceptable statistical heterogeneity (I 2 =93.1%).
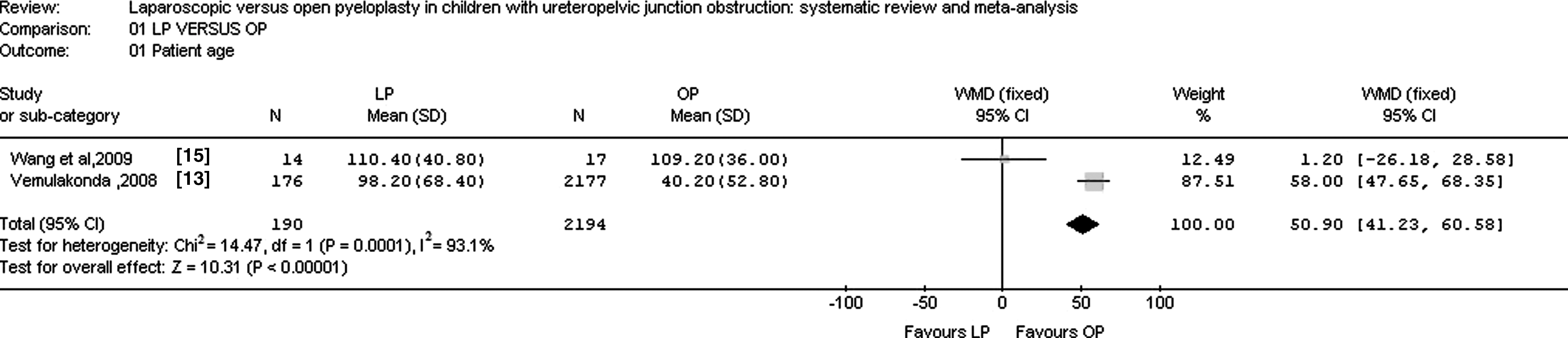
Meta-analysis of the patients' age between laparoscopic pyeloplasty (LP) and open pyeloplasty (OP) (all available data). The lower and upper confidence interval (CI) values refer to 95% CIs. WMD=weighted mean differences.
Operative time
Seven of the included studies reported that the operative time of LP was significantly longer than that of OP, 10,12,15,17,18,21,24 whereas the learning curve for this minimally invasive technique existed. Moreover, meta-analysis of the two studies 15,17 that reported data in mean±SD values revealed that the operative time of LP was significantly greater by 59.00 minutes (WMD=59.00; 95% CI=41.15 to 76.85; P<0.00001, Fig. 3).

Meta-analysis of operative time between laparoscopic pyeloplasty (LP) and open pyeloplasty (OP) (all available data). The lower and upper confidence interval (CI) values refer to 95% CIs. WMD=weighted mean differences.
Complications
Seven studies reported postoperative complications (Table 3). 10,12,15,17,18,21,24 The top four complications of patients who underwent LP were urinary leakages (14 in 192 cases), urinary infections (with or without fever, 6 in 192 cases), stenosis (2 in 192 cases), and bleeding (2 in 192 cases), respectively. Meanwhile, the top four complications after OP were urinary leakages (11 in 220 cases), urinary infections (with or without fever, 9 in 220 cases), wound infections (5 in 220 cases), and abdominal complications (including abdominal wall palsy and ileus, 5 in 220 cases). Other complications after OP included worsening of hydronephrosis after stent removal in two patients, stenosis in two patients, bleeding in two patients, and pain in one patient. Analysis of the pooled data revealed that the total incidence of all above mentioned complications in the OP group was not significantly different from those of the LP group (OR=0.78; 95% CI=0.46 to 1.34; P=0.37, Fig. 4); however, the incidence of wound infections tended to be higher in the OP group than in the LP group (5 cases vs 0 case).
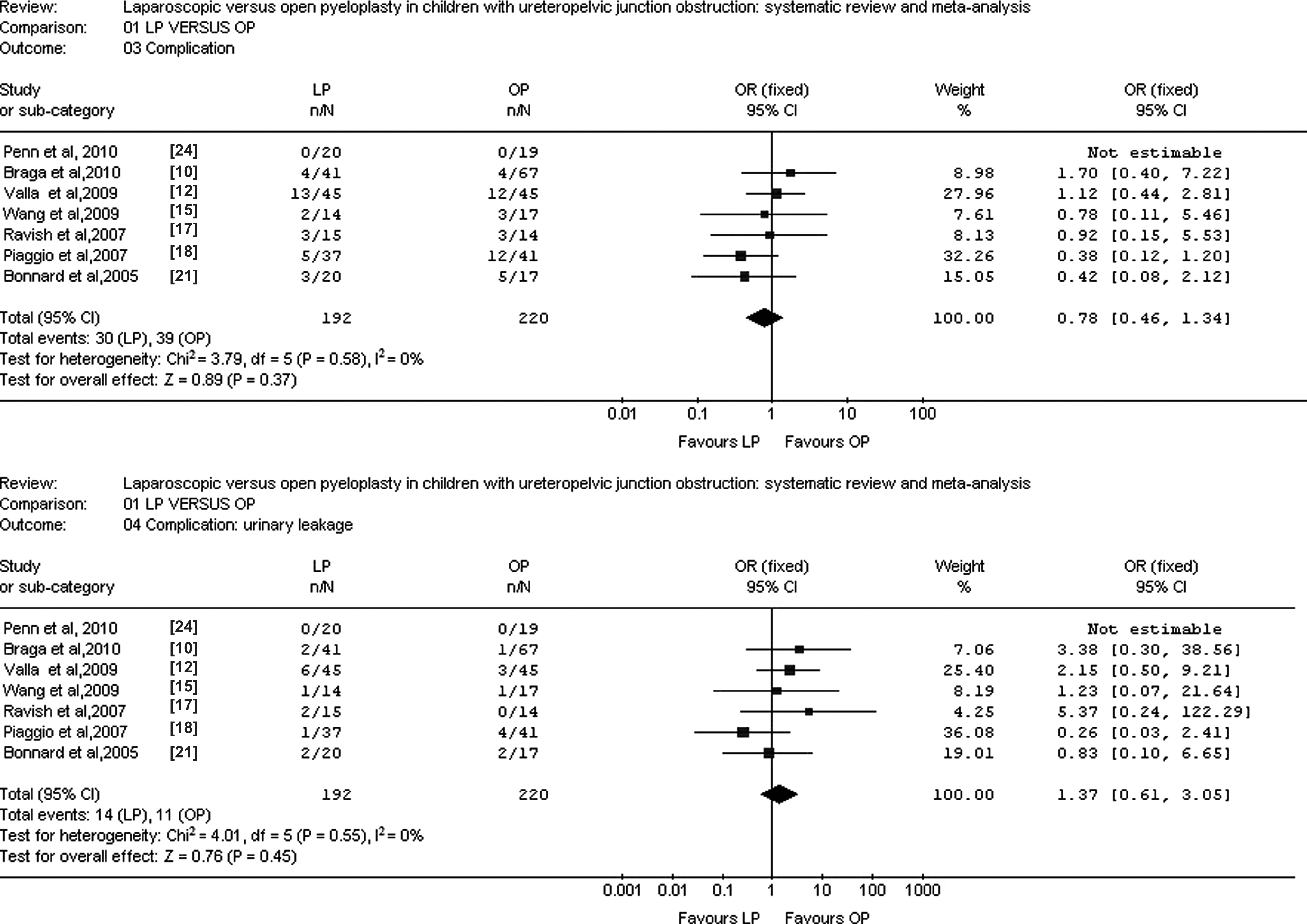
Meta-analysis of postoperative complications between laparoscopic pyeloplasty (LP) and open pyeloplasty (OP) (all available data). The lower and upper confidence interval (CI) values refer to 95% CIs. OR=odds ratio.
Duration of hospital stay
Three studies providing mean±SD values were included (Fig. 5), 13,15,17 showing a significantly shorter mean duration of hospital stay (0.40 d) for LP (WMD=−0.40; 95% CI=−0.77 to −0.03; P=0.03), but with unacceptable statistical heterogeneity (I 2 =95.8%). Exclusion of the study by Vemulakonda and coworkers 13 from the analysis significantly improved heterogeneity to 13.8% (Fig. 5) and resulted in no significant change in the final result. A 3.70-day difference in mean duration of hospital stay remained statistically significant in favor of laparoscopy (95% CI=–4.72 to –2.68, P<0.00001). Conclusions remained the same when only studies with moderate bias or all studies were included in this analysis.

Meta-analysis of duration of hospital stay between laparoscopic pyeloplasty (LP) and open pyeloplasty (OP) (all available data). The lower and upper confidence interval (CI) values refer to 95% CIs. WMD=weighted mean differences.
Success rates
According to the reviewed literature, success rates were measured in seven of the studies. 10,12,15,17,18,21,24 In most studies included in the meta-analysis, success was defined as symptom resolution and improved ultrasonographic or renographic parameters during the follow-up period, such as marked reduction of hydronephrosis on ultrasonography or improvement in the drainage curve on diuresis renography. Analysis of the pooled data revealed that the success rates were not significantly different in the OP group compared with the LP group (OR=1.76; 95% CI=0.71 to 4.36; P=0.22, Fig. 6).

Meta-analysis of success rates between between laparoscopic pyeloplasty (LP) and open pyeloplasty (OP) (all available data). The lower and upper confidence interval (CI) values refer to 95% CIs. OR=odds ratio.
Stent placement rates
Five studies reported the placement of a Double-J® stent in both LP and OP groups (Fig. 7). 10,15,17,18,24 Analysis of the pooled data revealed that the stent placement rates were significantly higher in the LP group compared with the OP group (OR=5.97; 95% CI=3.17 to 11.26; P<0.00001, Fig. 7), but with unacceptable statistical heterogeneity (I 2 =63.8%).
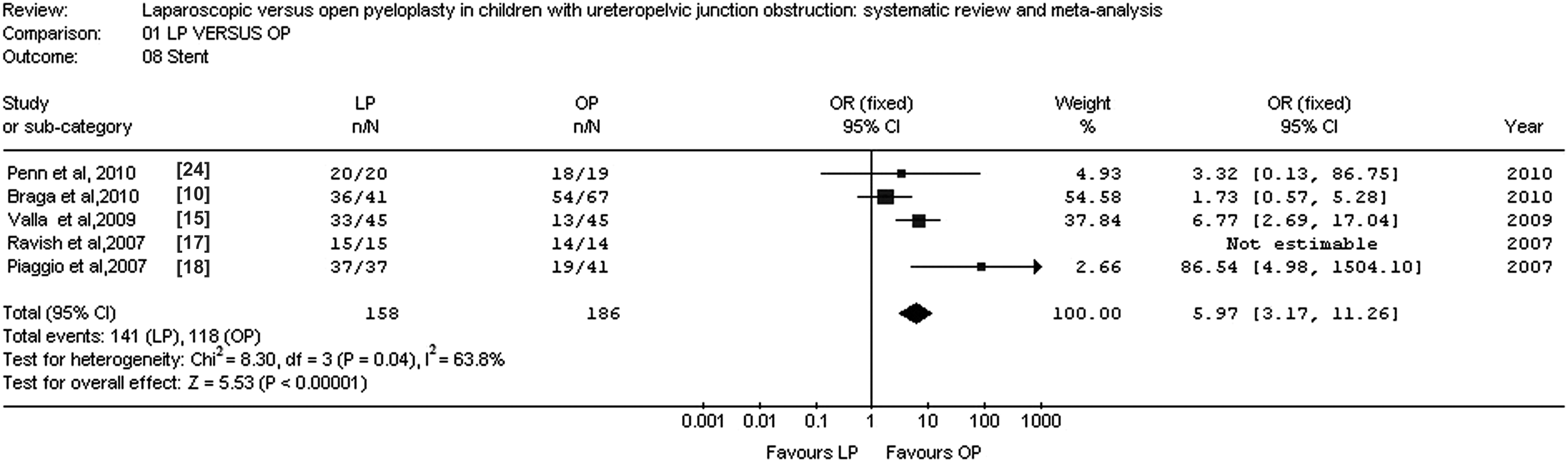
Meta-analysis of stent placement rates between between laparoscopic pyeloplasty (LP) and open pyeloplasty (OP) (all available data). The lower and upper confidence interval (CI) values refer to 95% CIs. OR=odds ratio.
Publication bias analyses
We analyzed the possible publication bias by generating funnel plots of the trials used for all of the evaluated comparisons of outcomes. No clear bias was apparent. As an example, we present the funnel plot of success rates showing no obvious asymmetry (Fig. 8).

Funnel plot regarding success rates. On the X axis, the observed risk differences (RD) are shown for each trial; on the Y axis, the standard error (SE) for each risk difference is shown as a proxy for study size. The plot did not show large asymmetry, which would indicate missing trial results in a certain area.
Discussion
Up to now, only a few studies have compared the LP (without hand or robot assistance) and OP for the management of UPJ obstruction in the pediatric population younger than 18 years. After searching the online databases, nine comparative articles were retrieved for this systematic review and meta-analysis. In these included articles, three were prospective studies, 15,17,24 in which 99 patients were alternately assigned to undergo LP or OP (49 vs 50 cases). The other six were retrospective comparative studies, 9,10,12,13,18,21 in which children were allocated to either operative group driven by surgeons' preference for laparoscopy or open surgery. Two of these studies 9,13 did not report sufficient information and should be viewed with great caution with regard to generalizing their results.
The optimal age is one of the concerns for the application of LP in children. It is generally believed that it is difficult to perform LP in small children with the risk of pelvic perforation when introducing the trocars; excellent intracorporeal laparoscopic suturing skills are imperative in limited spaces. 12 In this systematic review, only two studies presented the patient's age as mean±SD, 13,15 and the analysis showed that the patients who underwent LP were significantly 50.90 months older than those who OP. In the other seven studies, some authors proved that the patients in the open group were younger than those in the LP group. For example, Valla and associates 12 and Piaggio and colleagues 18 reported more young patients (younger than 1 year) in the OP group. The other authors, however, reported the patients' ages in the LP group were similar or even less than those of the OP group. 10,15,17,21,24 We believe that with the development of laparoscopic instruments, young patients are also suitable for LP in experienced hands.
Another concern encountered in the repair of UPJ obstruction is the surgical experience or the learning curve. Linear regression analysis demonstrated an inverse correlation between laparoscopic operative time and surgeon experience (estimated based on cumulative number of cases); in contrast, the operative time for OP remained stable through time. 10 The cumulative experiences with laparoscopic procedures could also mean reasonably reduced conversions to OP, potentially lower complications, and a fairly good success rate. 25,26 The learning curve was significant in the study by Bonnard and coworkers 21 in which the mean operative time was decreased from 4 to 3 hours, and two patients in the laparoscopy group needed conversion to open surgery at the beginning of their experience. Bansal and colleagues 11 showed that the total operative time was shortened along with the improved experience of LP, and the average time reduced to 202 minutes for the last five patients. Once the learning curve was overcome, the laparoscopic operative time could be comparable to those of open counterparts. 10 Zhang and associates 20 eventually reported a shorter median operative time in the laparoscopic group compared with the open group (80 vs 120 min, P<0.001).
To attempt a fairer comparison with the traditional open approaches, most laparoscopic cases should be performed by experienced surgeons to adjust for the potential learning curve effects of LP. In this study, although our data showed that the operative time for LP was significantly longer by 59.00 minutes, only one study reported that both LP and OP were performed by the same experienced surgeon with the same surgical team (Wang), 15 which would positively bias the results in favor of LP and reduce external validity.
In this systematic review, seven studies reported the transperitoneal or retroperitoneal approach, the dismembered or nondismembered fashion, the number and size of trocars, and the insertion of a ureteral stent. 10,12,15,17,18,21,24 Arguments still rage concerning which laparoscopic approach to advocate, either laparoscopic transperitoneal or retroperitoneal pyeloplasty. There are only a few studies with controversies comparing both techniques in the literature. 27 –29 Abuanz and coworkers 30 conducted a retrospective nonrandomized study and revealed that both approaches showed satisfactory comparable outcomes without significant difference in the success rate, while the retroperitoneoscopic approach was associated with a longer operative time and a greater conversion rate than transperitoneoscopy. Some authors speculated that it was probably related to the limited working space, especially in infants, which made suturing more difficult. 21 Sedlacek and associates, 31 however, recommended that the transmesocolic LP was a standard approach for the left-side UPJ obstruction repair, allowing microsurgical performance in all pediatric age groups. In this systematic review, however, because of the limited data in included studies, it is difficult for us to compare the difference between transperitoneal and retroperitoneal LP.
To the best of our knowledge, there were few reports that compared the therapeutic results of dismembered and nondismembered LP. 32,33 Even though time-consuming, Anderson-Hynes dismembered pyeloplasty remains the most efficacious operative technique. According to Szydelko and colleagues, 33 however, laparoscopic nondismembered Y-V pyeloplasty appeared to be a safe, attractive alternative to Hynes-Anderson dismembered pyeloplasty in patients without dorsally crossing vessels. 33 In addition, the type of ureteral stent (Double-J, Salle, or others) and drainages used in different groups and studies may impact the results. Double-J stents and drainages were routinely placed and remained indwelling for several weeks in some studies, while stent placement was performed according to surgeon preference, or depending on operator convenience. Valla and associates 12 reported that more cases encountered anastomotic complications (leakages and stenosis) in both laparoscopic and open surgery groups of nonstented anastomoses, and needed a secondary anesthesia for stent placement with cystoscopy.
In this meta-analysis, we noted a higher proportion of patients with stents in the LP group. Because stent removal is associated with secondary anesthesia, we suspect that the LP procedure will add to the cost and morbidity for patients with UPJ obstruction. Because of the limited data in included studies, however, the comparison of cost between LP and OP was not performed in this meta-analysis. We believe that stent placement is an important variable to report for the LP procedure, especially when costs and morbidity are considered.
This meta-analysis revealed that the incidence of overall complications was similar in the OP group compared with the LP group (P=0.37). These complications included anastomotic urinary leakage, urinary tract or wound infections, and stenosis. A small number of patients had worsening of hydronephrosis after stent removal, abdominal complications (including abdominal wall palsy and ileus), bleeding, and pain. Some researches revealed that LP was associated with more anastomotic leakage than OP, 8,18,34 which may be related to differences in tissue handling and the quality of suture. In this meta-analysis, the urinary leakage and urinary tract infection were measured in seven identified studies, 10,12,15,17,18,21,24 with no significant difference, but the wound infection rate tended to be higher in the OP group.
Our analysis revealed that the success rate was not significantly different between the LP and OP groups (P=0.22). Piaggio and colleagues 18 even showed a higher success rate for LP in patients older than 14 months. 18 Some studies did not explicitly state how the diagnosis of success was reached in each of these cases. In addition, the great majority of studies showed the same limitation of laparoscopic surgery; ie, shorter follow-up compared with traditional open procedures (as shown in Table 3). Valla and coworkers 12 believed that surgery was considered successful if symptoms were improved, pelvic/caliceal dilatation decreased on ultrasonography, or renal drainage/function improved renographically. The success rates, however, were not clearly described by Tanaka and associates 9 and Vemulakonda and colleagues. 13 The lack of a “success” definition and the difference of follow-up may potentially create internal and external validity problems influencing the outcome. In this systematic review, we found that the mean hospitalization was significantly shorter in the laparoscopic group. However, Tanaka and coworkers 9 reported that the laparoscopic approach decreased the length of stay in patients older than 10 years, the preadolescent and adolescent groups, but not in any of the younger groups. As a result, we should be careful to interpret faster convalescence and earlier hospital discharge associated with LP, because these findings might not necessarily apply for all age groups.
Conclusions
With this systematic review and meta-analysis of articles from the medical literature, we approve that LP is a safe and effective procedure for the management of UPJ obstruction in the pediatric population. The shorter hospital stay, excellent outcomes, and without significant additional risk of postoperative complications of the laparoscopic procedure indicates potential benefits over traditional open procedures. In current clinical practice, LP can be used as an alternative to open surgery according to the surgeon's discretion and laparoscopic experience. Because of publishing bias, however, a series of RCTs are necessary to explore the efficiencies of LP in the management of pediatric UPJ obstruction.
Footnotes
Acknowledgment
This work was supported by the National Natural Science Foundation of China (No. 30200284, No. 30600278, No. 30772359, No. 81071997, No. 81072073), Program for New Century Excellent Talents in University (NCET-06-0641), Scientific Research Foundation for the Returned Overseas Chinese Scholars (2008-889), and Fundamental Research Funds for the Central Universities (2010JC025).
Disclosure Statement
No competing financial interests exist.