
Abstract
Purpose:
To report the first long-term experience on the efficacy of bipolar transurethral radiofrequency needle ablation (RFA) in patients with lower urinary tract symptoms that are secondary to benign prostatic hyperplasia.
Patients and Methods:
A nonrandomized prospective cohort of 12 candidates for transurethral resection of the prostate underwent bipolar transurethral RFA in 2004 (mean age 63; prostate volume 34 cc). Patients were evaluated preoperatively and at 3, 12, 36, and 60 months postprocedure. International Prostate Symptom Score (IPSS), quality-of-life (QoL) index, peak urinary flow rate (Qmax), postvoid residual volume (PVR), and need for a second procedure were evaluated at each follow-up interval.
Results:
Significant improvement in urinary symptoms and voiding parameters occurred at 1 year after the procedure. Mean improvements for IPSS, QoL, and Qmax were 12 points, 3.5 points, and 8 mL/s, respectively. Improvement, however, was not sustained in the long term. Nine patients ultimately had treatment failure necessitating a secondary procedure, one at 2 months, five after 3 years, and three by 5 years. Two patients were lost to follow-up. Only one patient had long-term benefit from the procedure.
Conclusion:
In the short term, bipolar RFA produced clinically meaningful improvement in symptom scores and voiding parameters. The majority of patients, however, eventually experienced treatment failure and needed additional surgical procedures. Only 8% of patients had long-term (>5 years) benefit.
Introduction
With bipolar technology, alternating electric currents pass between two electrodes in close proximity and both are usually built into the same radiofrequency ablation (RFA) delivery device rather than a single electrode on a delivery device and a return electrode in the form of a plate placed on a remote location on the skin, as in monopolar RFA technology. Ex vivo testing in kidney and prostate has shown it produces larger and more defined lesions compared with monopolar electrodes. 3,4
A bipolar RFA system is currently commercially available in Australia, where it has reimbursement, although it is not actively marketed in any way by its manufacturing company. To date, there have been no published data in the use of this technology. In this study, the Olympus CelonURO™ bipolar RFA system was used. This system has the benefit of real-time impedance feedback in which it constantly adjusts the power flow to the tissue impedance, enabling optimal energy deposition while preventing overdosing and carbonization. While the tissue response to bipolar RFA appears to be superior to that of monopolar RFA, durable clinical improvements compared with monopolar systems are yet to be determined.
This is the first study that prospectively evaluated the men who underwent the CelonURO™ bipolar radiofrequency-induced thermotherapy (RFITT) for lower urinary tract symptoms (LUTS) and evaluated its long-term efficacy in terms of the changes in LUTS, voiding parameters, and the need for secondary procedures were documented.
Patients and Methods
Men with symptomatic BPH who were candidates for surgery and without a history of surgical treatment to the lower urinary tract were enlisted into the study. A total of 12 men provided informed consent to undergo treatment with bipolar RFA of the prostate in 2004.
At presentation, all patients completed the International Prostate Symptom Score (IPSS) and quality-of-life (QoL) score. The peak urinary flow rate (Qmax) and ultrasonographic postvoid residuals (PVR) were measured. These parameters were reassessed at 3 months and 1, 3, and 5 years.
On the day of the procedure, a transrectal ultrasound probe measured prostate size. All patients underwent general anesthesia and were given intravenous gentamicin at the time of induction.
They underwent bipolar RFITT using the CelonUR Olympus system by one surgeon (HW) in a single center. The bipolar probe is connected to the generator box and can be passed through the working channel of a standard 22F cystoscope sheath. The probe is 2-mm in diameter, and its geometry is outlined in Figure 1. Under cystoscopic guidance, the prostate was punctured just proximal to the verumontanum, and under direct vision, it was ensured that both electrodes were advanced through the mucosa and for an additional distance up to transverse line markers to minimize the risk of mucosal thermal injury (Figs. 2 –4). Power was set for treatment of each lesion at 7 watts.

Schematic of bipolar radiofrequency needle.
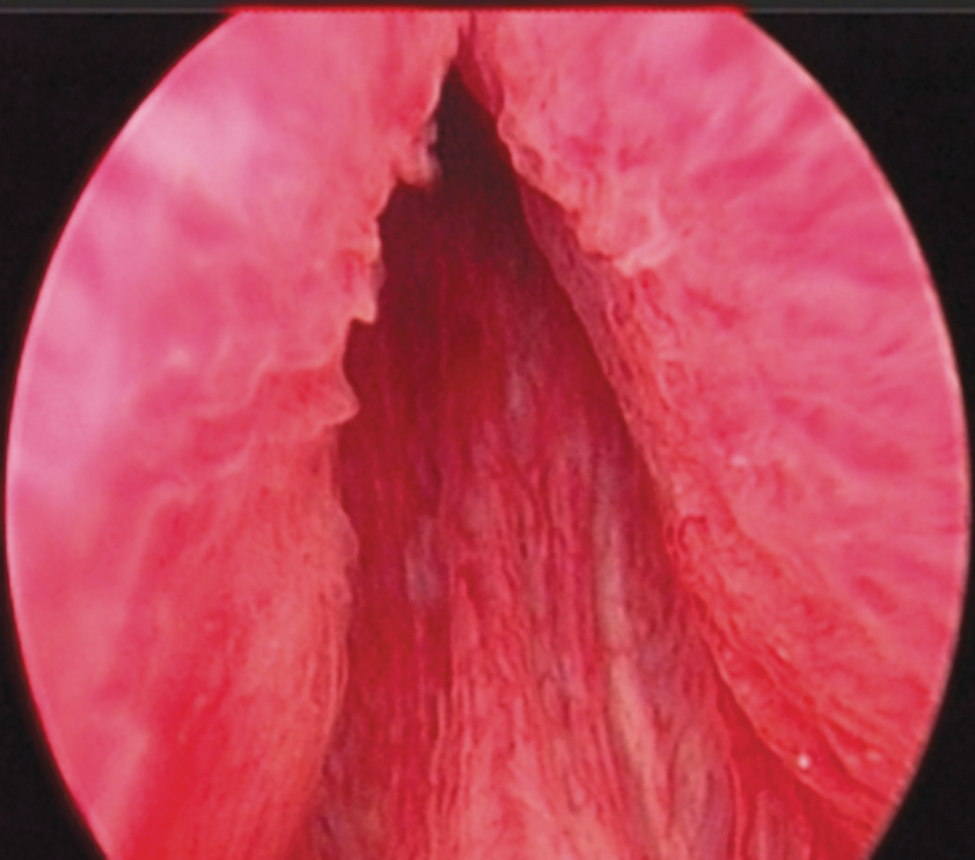
Preparation for puncture. The cystoscope is positioned to enable the first puncture just proximal to verumontanum.

Bipolar electrode. Both electrodes are visible, and the probe needs to be advanced so that both are completely within the prostate tissue.
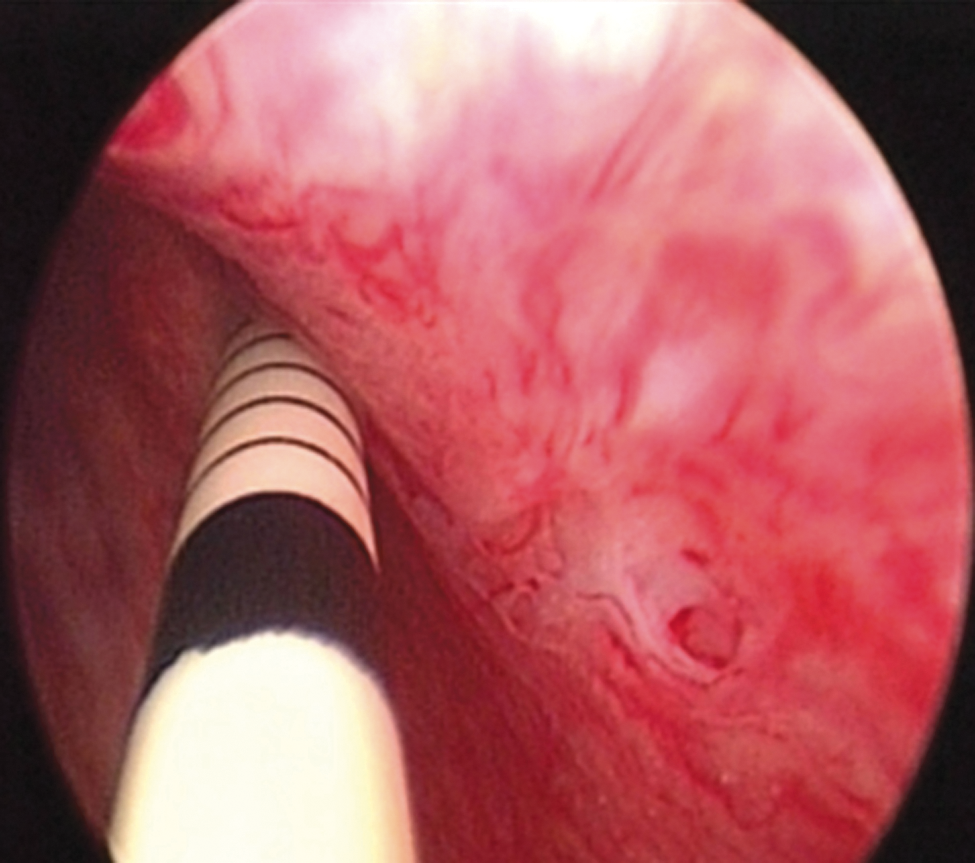
Correctly positioned bipolar probe. Horizontal marker lines indicate that the probe has been advanced to an appropriate degree.
Coagulation was induced for 1.5 to 2 minutes until the impedance monitor ceased delivery of power automatically. If the probe was inserted beyond the prostate capsule or into the bladder, inappropriate impedance would be recognized by impedance outputs on the generator box. Indication of completed coagulation was by an acoustic monitor that rapidly rose in pitch as each treatment was completed. The prostate was then repunctured approximately 1 cm away from the previous puncture in a caudal direction. These subsequent and more proximal punctures were made according to the prostate size allowance, and this could be estimated from preoperative transrectal ultrasonographic measures and knowledge of the dimensions of the RFA probe. The number of insertions depended on the prostate size and was continued until just distal to the base of the bladder. An indwelling catheter was left at the end of the procedure, and a trial of void day was undertaken 1 day postprocedure.
In the postoperative period, the men were monitored for complications or adverse events. The men were then reviewed at 3 months and 1, 3, and 5 years postprocedure. At these times, the IPSS and QoL score as well as PVR and Qmax measures were repeated. Patients in whom recurrent symptoms developed that warranted another surgical procedure were regarded as having treatment failure and were not included in the long-term analysis results.
All patients gave written informed consent to participate in the study, and analyses were performed using deidentified data. The technology was approved by the Therapeutic Goods Administration in Australia for use as RFA of the prostate in the same category as TUNA.
Results
Mean baseline characteristics were age 63 years (range 53–77 y), IPSS was 23 (range 16–27), and QoL score was 5 (range 3–6). The mean Qmax was 7 mL/s (range 4–11 mL/s), and PVR was 182 mL (range 22–601 mL). The average prostate volume on transrectal ultrasonography was 34 cc (range 20–66 cc) (Table 1).
IPSS=International Prostate Symptom Score; Qmax=peak urinary flow rate; PVR=postvoid residual; LOC=length of catheterization.
The mean operative time was 20 minutes (range 12–34 min), and average number of lesions created were 6 (range 3-12). All patients had a successful trial of void, day 1 postprocedure. There were no significant adverse postoperative events, including no reports of hematuria, urinary tract infections, incontinence, or retention. While erectile function was not formally assessed, no man raised any concern about loss of erectile function. Ejaculatory function was specifically asked of each man, and none reported a change from antegrade ejaculation to a loss or reduction in emission with orgasm.
One patient was regarded as having treatment failure at the 3-month review, necessitating TURP 2 months post-RFITT. Two patients were lost to follow-up at the 12-month review. At 3 years, five of the remaining nine patients had symptoms that were significant enough to need a secondary procedure. The remaining four patients were reviewed at 5 years. Three of these men had symptoms that were significant enough for them to request intervention, resulting in only one patient with long-term benefit from bipolar RFA.
Changes in urinary symptoms
At the 3-month postprocedural review, the IPSS had decreased by 9 points, giving a mean score of 14. Symptoms continued to improve, and at 12 months, the IPSS was down to 11. Despite small study numbers, Wilcoxon signed rank sum test showed this mean decrease in IPSS of 12 points was significant (P=0.01). After 3 years, however, the mean IPSS score markedly increased to 20 (Table 2).
IPSS=International Prostate Symptom Score; QoL=quality of life; Qmax=peak urinary flow rate; PVR=postvoid residual.
The QoL score also initially showed improvement. At baseline, the mean value was 5 (s=1.5). At the 3-month review, this had decreased down to 1.5 (s=1.7). This improvement was maintained at the annual follow-up, but QoL relating to voiding behavior started to decline after this. At the 3- and 5-ear follow-up, the mean QoL score was 3.
Voiding parameters
The initial mean peak flow was 7 mL/s. This improved to 13 mL/sec at 3 months, and 15 mL/sec at 1 year. On the Wilcoxon signed rank sum test, this improvement in flow rate of 8 mL/sec was significant (P=0.01). The initial PVR was 182 mL. While this initially decreased to 72 mL at 3 months, the improvement was not sustained, with the mean PVR at 1 year being 158 mL.
Need for a second procedure
At 3-month review, one patient had experienced recurrence of symptoms significant enough to warrant a second procedure. He underwent a diathermy TURP. After 3 years, this had increased to include another five patients, and at 5 years, another three patients warranted surgical intervention. Secondary procedures were either greenlight laser prostatectomy or diathermy prostatectomy (TURP).
One patient, however, did appear to experience relative longevity with treatment. At 5 years, he reported an IPSS of 12, QoL of 1, and Qmax of 14 mL/sec.
Discussion
TURP has been used to treat patients with benign prostatic hyperplasia since the 1920s and is still considered by most the gold standard treatment. It continues to hold this title because of the longevity of its results. Recent reviews put the reoperation rate for TURP at 8% to 15% over 10 years. 5 TURP, however, has the potential for significant morbidity, which has been reported to be as high as 9%. 5,6 These limitations drive the desire for a safer, cost-effective, minimally invasive surgical treatment options for BPH.
RFA has been one of the principal minimally invasive surgical options that has been used. Initially, RFA electrodes were monopolar. A recent meta-analysis of outcomes from unipolar RFA by Bouza and associates 2 found that TUNA initially reduced the IPSS and QoL score by 50% to 60% compared with pretreatment values. This improvement, however, was not sustained, and a trend toward deterioration in the initial results was evident after 3 years. This resulted in a significant number of patients needing re-treatment, with as many as 13% in the first 2 years after treatment. The high re-treatment rates are balanced against the potential advantages of TUNA in that it appears to be safe and with minimal significant complications. Also, TUNA potentially “buys time” for persons who seek to benefit from technologic advancements in the future.
Bipolar RFA theoretically had the potential to overcome the short duration of outcomes experienced with monopolar TUNA. In vitro testing had shown bipolar RFA produced larger and more defined lesions. 3,4 Initially, this study did demonstrate that early outcomes with bipolar RFA were promising, with a marked reduction in IPSS of 50% accompanied by an acceptable improvement in flow rate (twofold). Maximum benefit appears to develop with time, with better results observed at 1 year compared with 3 months. These early results are comparable to the initial outcomes seen with monopolar RFA, TURP, and laser procedures for BPH.
Unfortunately, these improvements in symptoms were not durable, and the long-term results are poor. After 5 years, 8 of 9 remaining patients had had a second procedure. Second procedures offered were either photoselective vaporization prostatectomy or standard TURP. Of the remaining patient not needing a second procedure, the outcome measures at 5 years were better than the initial baseline results but worse than the 1-year follow-up results.
Study limitations include small sample size (ie, 12 patients) and the potential learning curve that is associated with any new technology. Although this procedure is technically easy to perform for an experienced endoscopic surgeon, it is not known whether, with more experience, more durable results may be achieved. Since the Celon Uro has been commercially available, there have been no hardware or software updates in response to clinical results.
Conclusion
Our study is the first documenting long-term outcome of the bipolar rRFA of the prostate. The results demonstrate that bipolar RFA produces acceptable short-term improvement in voiding symptoms with minimal complications. The results, however, are not durable: Recurrent LUTS developed in 92% of patients or they had undergone a secondary procedure by 5 years. Only one patient appeared to have satisfactory longevity with the procedure. This finding is consistent with the existing data from the monopolar RFA treatment. Although not directly compared with monopolar treatment, there does not appear to be any significant advantage in this series.
Footnotes
Acknowledgment
The Celon-Uro generator was provided on loan from Olympus AG (Germany). The bipolar electrodes were also provided without cost.
Disclosure Statement
Henry Woo is a consultant to American Medical Systems and Neotract Inc. No competing financial interests exist for the other authors.