
Abstract
Purpose:
The aim of this study was to analyze the sphincteric/perisphincteric lesions and modifications in incontinent patients with iatrogenic damage to the external urethral sphincter after radical prostatectomy (RP).
Patients and Methods:
We evaluated 169 patients with postprostatectomy urinary incontinence who were referred from 28 German hospitals from December 2004 to March 2009. Inclusion criteria were refractory grade III stress urinary incontinence and duration of incontinence of at least 12 months. Patients underwent clinical, ultrasonographic examination, urethrocystoscopy, and if technically possible, urethrocystomanometry. Sphincteric defects were classified and evaluated with regard to type and localization.
Results:
Mean duration of incontinence before evalulation was 44.8 (12–156) months. Distribution of the previous prostatectomy technique was 66.9% retropubic RP, 27.8% laparoscopic RP, 3.5% perineal RP, and 1.8% robot-assisted RP. A transection of the sphincter was seen in 65.1% (110/169) of cases, a sphincter penetration in 46.2% (78/169) of cases. A combination of both sphincter injuries was seen in 37% (63/169) of patients. In 87% (147/169) of the cases, the sphincter defect was localized to the lower circumference, and in 13% (22/169) of cases, to the upper circumference. A stricture of the vesicourethral anastomosis was found in 45% (76/169) of cases.
Conclusions:
Direct iatrogenic damages to the urethral sphincter are a potential reason for postprostatectomy urinary incontinence. They seem to follow a particular local distribution pattern, indicating that apex preparation and building of the urethrovesical anastomosis show an increased risk for these sphincter injuries. Cystoscopic evaluation of the sphincteric region in incontinent patients after surgery may be a valuable tool for examination.
Introduction
The literature on incontinence after RP suggests a wide variation in the definition of and methodology for assessing incontinence. Loughlin and Prasad 7 suggest to focus on three important factors: (1) Methodologic instruments and definitions of postprostatectomy incontinence; (2) potential intraoperative factors that may influence risk of postprostatectomy incontinence; (3) potential preoperative factors that influence postprostatectomy continence. 7
Currently accepted assessment tools for urinary incontinence include pad test, questionnaires, and urodynamic testing for a complete evaluation of postprostatectomy incontinence. 8 –10 Urinary incontinence after RP can be a result of sphincteric incompetence or bladder dysfunction. In most cases, it is caused by intrinsic sphincter deficiency. 11 Groutz and colleagues 12 assessed the pathophysiology of incontinence after RP. In their study, intrinsic sphincter deficiency was the most common urodynamic finding and dominant cause of incontinence, occurring in 73 (88%) patients. Impaired bladder contractility and bladder outlet obstruction were found by linear passive urethral resistance relation in 82% and 16%, respectively, but were considered to be clinically relevant in only 32% and 6% of cases, respectively. In addition, the authors concluded that low urethral compliance, presumably from urethral scarring, was a significant cause for the incontinent situation of the patients. No endoscopic evaluation of the sphincteric region in terms of a urethrocystoscopy was performed, however, to support these findings.
Using transurethral ultrasonography, Strasser and coworkers 13 contributed sonomorphologic data and anatomic histologic results strongly suggesting that the rhabdosphincter constitutes the main component of the continence mechanism in postprostatectomy patients. They describe the rhabdosphincter as an omega-shaped muscular loop ventral and lateral to the membranous urethra and prostate that is separated from the smooth muscular layer of the membranous urethra presenting as a hypoechoic structure surrounding the membranous urethra at its ventral and lateral aspects. They visualized that during contraction, the rhabdosphincter retracts the urethra, pulling it toward the rectum and compressing its lumen. In addition, the authors concluded that measurement of maximal urethral pressure has little clinical relevance when assessing etiology of urinary incontinence from RP.
At our institution, we treat patients with refractory postoperative urinary stress incontinence from damage of the urethral sphincter using autologous skeletal muscle-derived cells. 14 Urethrocystoscopy is an important part of this procedure.
Our patients originate from a variety of different urologic departments from all over Germany. Most of them had previously undergone RP. This large number of post-RP incontinent patients allows us to evaluate and classify sphincter lesions as the major culprit of incontinence after this surgical procedure.
Patients and Methods
Patients
From December 2004 to March 2009, a total of 169 men aged 48 to 82 years (mean 68 y) who complained of stress urinary incontinence after RP and who came from all parts of Germany, representing 28 different surgical centers (urology departments), were sent to our institution. No patient had received any additional surgery of the urethra or bladder after RP. In only 49 patients, tumor classification after radical surgery was traceable and revealed pT1 in 4.1% (2/49), pT2 in 53% (26/49), pT3 in 38.8% (19/49), and pT4 in 4.1% (2/49) patients. Of those tumors, at least 15 were classified as pT2c, 10 as pT3a, and 8 as pT3b, thus indicating that the predominant tumor stage was locally advanced in 67.3% (33/49) of cases. None of the patients had received radiotherapy after RP. Inclusion criteria for this analysis were grade III stress urinary incontinence, duration of incontinence of at least 12 months. Urinary incontinence had to be therapy refractory, defined as the persistent need for aids postprocedure. Earlier sling procedures were a contraindication for referral. Stress urinary incontinence grade III was clinically defined as urine loss while lying down without physical activity.
Methods
Urinary incontinence was assessed in all patients following the most recent European Association of Urology 15 (EAU) Guidelines on Urinary Incontinence for general assessment of unrinary incontinence in men, including medical history and physical examination, urine analysis, postvoid residual urine, frequency/volume chart, pad test, and serum creatinine value if there was a suspicion of renal disease. Current urinary tract infection was excluded before invasive diagnostics; information regarding recurrent urinary tract infections in the medical history was inconsistent and often not documented. Urodynamic testing by urethrocystomanometry was planned for all patients and performed when possible. The examinations were concluded by the endoscopic evaluation of the urethra and urethral sphincter. We used a urethrocystoscope with a 12 grade visual appearance for accurate description and localization of all possible sphincteral defects and abnormalities and anatomic alterations. We also evaluated the rhabdosphincter during contraction for visual confirmation of contractility of the muscle.
Final diagnosis was based on clinical judgment considering patient history, voiding diary, and the respective, above described examinations.
Results
Duration and previous treatment of incontinence
Mean duration of incontinence before presentation to our institution was 44.8 months and ranged from 12 to 156 months. All patients had undergone previous approaches to treat urinary incontinence without sustained effect. Those approaches included: Pelvic floor exercise, anticholinergic medications, serotonin/noradrenaline reuptake inhibitor such as duloxetine, electromotive drug administration, applications of bulking agents. At least all patients had used aids, such as special incontinence pads, special diapers, or urinal condoms. Patients reported frequent use of incontinence pads; mean use was 5 pads per day and at least one pad per night. Use of special diapers or urinal condoms was reported by 9 patients. None of the patients had previously agreed to receive an artificial urinary sphincter even when suffering of urinary incontinence for almost 4 years.
Urethrocystomanometry
Because of a high-grade concomitant subvesical stricture, it was not possible to perform a urethrocystomanometry in 43.2% (73/169) of patients before endoscopic evaluation. All patients (56.8%; 96/169) who were subject to this examination had shown a decreased outlet resistance; in 33.3% (32/96) of cases, the bladder had a reduced capacity. All patients had a positive stress test. Patients with a concomitant subvesical stricture were shown to have a relevant additional obstruction.
Endoscopic results/evaluation
Evaluation of the urethra, the urethral sphincter, the vesicourethral anastomosis, and the bladder neck and documentation of defects in the sphincter/sphincter region were performed within a standard urethrocystoscopy.
Type of sphincteric defect
We observed two types of sphincteric defects. A transection (Fig. 1) of the sphincter was seen in 65.1% (110/169) of cases and sphincter penetration (assumed: while suturing) in 46.2% (78/169) cases (Fig.1). Sphincter trauma from a combination of both damages was seen in 37% (63/169) patients. In few cases, the intact suture was seen years after surgery as a scar of the entire circumference of the sphincter.
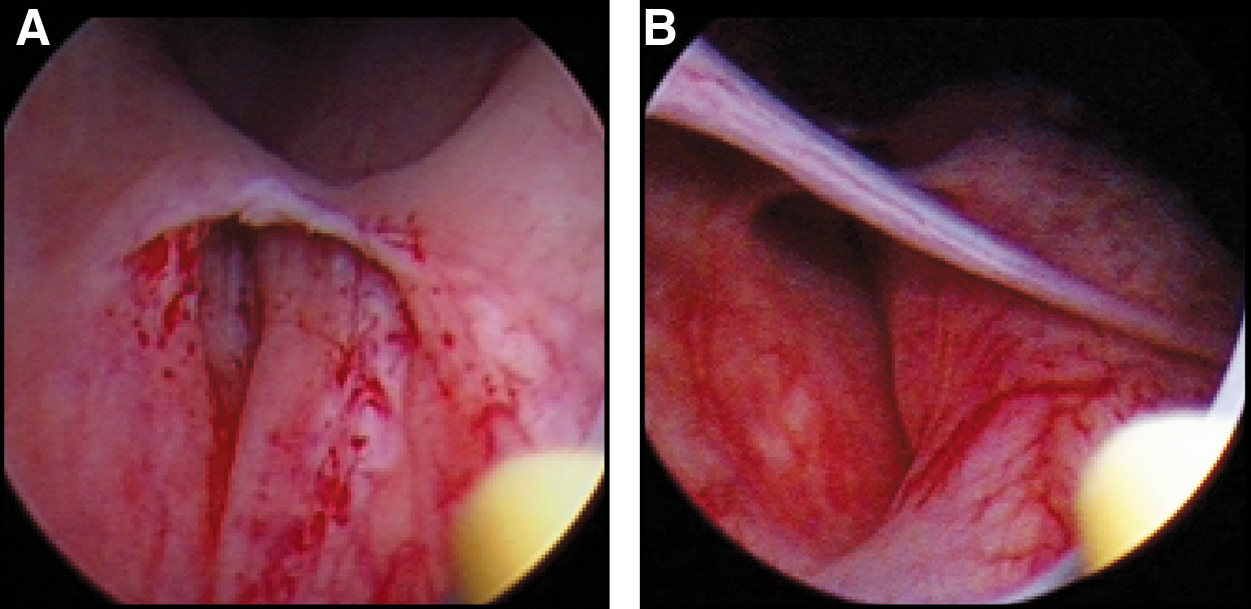
Sphincter penetration (assumed while suturing) is seen 12 months after surgery. In
Localization of sphincteric defect
Because of the incision technique during the dissection of the proximal urethra, a higher rate of sphincter damages was observed in the lower circumference (Table 1).
Concomitant subvesical strictures and localization in relation to the sphincter
In almost 85% of the cases, a concomitant subvesical stricture could be detected. Table 1 gives an overview of the observed localizations of those subvesical strictures.
Histomorphologic changes in the perilesional tissue
Resection of scar tissue of the anastomotic region was performed in 28.4% (48/169) of cases. In 6.3% (3/48) of patients, a local recurrence of prostate cancer was detected, whereas in the remaining patients, chronic inflammatory scar tissue was identified.
Techniques of RP
Table 2 gives an overview of the distribution of the different techniques of RP in the investigated patient group. Retropubic prostatectomy was shown to be the dominant procedure, followed by laparoscopic prostatectomy and robot-assisted prostatectomy.
Patients had undergone radical prostatectomy from 1993 to 2008, a span mostly dominated by open surgery but also characterized by important, emerging new developments in surgical techniques.
RP=radical prostatectomy.
Discussion
The topic of post-RP urinary incontinence is extensively discussed in current literature. Most adequately, the respective investigations concerning bladder and urethral sphincter function are based on urodynamic findings that compare urodynamic status before RP and during longitudinal follow-up. In a prospective analysis of 54 patients with clinically localized prostate cancer who were undergoing radical retropubic prostatectomy, Giannantoni and colleagues 16 interpreted impaired detrusor contractility, decreased bladder compliance, and intrinsic sphincter deficiency as de novo dysfunctions in a substantial proportion of patients as a consequence of bladder denervation in about 30% of cases after RP.
Porena and associates 17 analyzed 10 prospective and 9 retrospective studies comparing postoperative with preoperative urodynamic data at follow-up periods of 6 to 32 and 12 to 60 months and enrolling 13 to 82 and 24 to 146 patients, respectively. They conclude that postoperative bladder decentralization, inflammation and/or infection, geometric bladder wall alteration associated with preexisting hypoxemia with/without neuroplasticity have to be seen as important causes for postoperative detrusor dysfunction and subsequent incontinence. Consistent preoperative urodynamic data are often missing because they are not a preoperative standard, however. Thus, it remains difficult to assess the exact role of surgery in causing those functional abnormalities.
In an urodynamic study with fluoroscopic monitoring of 74 patients, Chao and Mayo 18 interpreted incontinence after RP as a result of sphincter weakness in the majority of cases. In their study, 57% of the patients had sphincter weakness alone, 39% had detrusor instability and/or decreased compliance combined with sphincter weakness, and only three (4%) patients had detrusor instability alone. In addition, the authors observed anatomic strictures relevant to postoperative voiding alterations in 24% of patients, which is in accord with the results presented here.
In the cohort presented here, the mean time to referral of about 3.5 years is high. The reported patients explicitly had denied an artificial sphincter as a surgical approach after failure of conservative therapies previously and alternative approaches were few in the past, thus giving a possible explanation for the prolonged waiting time.
Although not being considered the optimal way to assess sphincteric intactness, urethrocystoscopic view is an important tool to investigate the sphincter region after RP. Because this examination is invasive and may be disturbing for the patient, it is not recommended as a standard postoperative procedure but suggested as a supplemental tool within the two-stage assessment for diagnosis of complicated incontinence (including postprostatectomy incontinence) following the current EAU guidelines on urinary incontinence. 15 At our institution, we treat patients in a specific setting with autologous muscle-derived cells; initial endoscopic evaluation is a fundament of the diagnosis/treatment process and therefore very selectively allows us to evaluate sphincter defects. 14 Thus, endoscopic evaluation and a preselected group of patients with sphincter damage were the main pillars of this investigation.
A limitation of the study is that no preoperative urethrocystoscopy had been performed before RP, because this was neither a prospective nor a comparative study. Patients originated from different parts of Germany and had been operated on in a time span of 15 years. Therefore, this study remains descriptive in nature; a definitive comparison of the sphincter status preoperatively and postoperatively is not possible, and the characterization of the sphincter damage as iatrogenic, although highly probable, can only be assumed. Being familiar with the different techniques and taking into account the possible risks of radical prostatectomy, however, this assumption seems justified.
Our experience suggests that sphincter deficiency may be a result of three different types of damage: The respective defects may originate from a direct damage of the sphincter during preparation in terms of a incision or transection, from grasping of the sphincter while performing the suture for the vesicourethral anastomosis, or from indirect sphincter alteration through pre- or postsphincteric urethral strictures. The damage seems to result rarely from a single but frequently from a combination of the above traumas.
Strasser and colleagues 19 described distinct morphologic defects of the rhabdosphincter in patients with postprostatectomy or post-transurethral resection of the prostate stress incontinence compared with a control group of continent patients using three-dimensional transrectal ultrasonography. Interestingly, they could show interruption of muscle fibers ventrally by scar tissue in the majority of patients, which is not in accordance with the results presented here, because we show the majority of sphincter damages in the lower circumference of the sphincter. The authors from Austria did not distinguish between the different types of surgery leading to the damage of the sphincter; thus, it is critical to compare the results of their study with the results presented here. In contrast to our study, which represents at least 28 different surgeons and 4 different surgical prostatectomy approaches, Strasser and coworkers 19 did not provide information about the number of different surgeons. Therefore, assuming one or few surgeons, an individual lesion pattern cannot be excluded in their study. Because functional data of the rhabdosphincter are few and controversial, however, we do not think that our results contradict an assumed anatomy of an omega-shaped rhabdosphincter. In contrast, it may support the thesis that despite the endosonographically visualized hypoechoic structure surrounding the membranous urethra at its ventral and lateral aspects, the lower part may have a particular functional contribution, because damage in that region is associated with incontinence.
In a multivariate analysis, Eastham and associates 20 examined risk factors associated with incontinence in 581 patients who were undergoing radical retropubic prostatectomy and stated that the risk of urinary incontinence after RP is related to the age of the patient and to the used surgical technique. In particular, resection of the neurovascular bundles, techniques of bladder neck preservation or reconstruction seem to be of importance and are in the focus of modifications in newer techniques of RP. 21 Steiner 22 emphasizes so-called no touch or avoidance surgical principles as being the basis for continence-preserving RP. This technique primarily focusses on the preservation of the entire circumferential musculature of the rhabdosphincter, the fascial investments (the pubourethral ligaments anterolaterally and median fibrous raphe posteriorly), and the innervation of both the rhabdosphincter by way of the intrapelvic branch of the pudendal nerve (somatic) and the mucosal and smooth muscle components by way of the urethral branch of the inferior hypogastric plexus (autonomic). The probability to irreversibly damage the sphincter has to be calculated, however. Most frequently this is expected in the beginning of the learning curve of a particular surgeon, but may happen as an unpredictable complication along an entire surgical career.
Our study reflects the experience of at least 28 different surgeons performing RP using the currently accepted techniques. Retropubic prostatectomy was shown to be the dominant procedure followed by laparoscopic prostatectomy and robot-assisted prostatectomy. This does not represent, however, the current distribution of applied techniques in the country, because numbers of robot-assisted prostatectomy have significantly increased since. We did not have information such as experience of the particular surgeon, number of RP procedures per year of the surgeon, number of RP per year of the surgical center, stage in the learning curve of the surgeon/center with regard to the respective technique (laparoscopic, robot-assisted). Thus, a distinction between operational prostatectomy procedures and various sphincter defects within this cohort remains very critical.
About 90% of the observed sphincter damages were seen, however, in the lower circumference in close relation to the dorsal anastomosis sutures (6 o'clock); thus, it may be assumed that apex preparation and building of the urethrovesical anastomosis have an increased risk for sphincter injuries.
During the apical dissection, it is strongly recommended to preserve as much as possible of the circumferential muscle fibers of the rhabdosphincter, its fascial attachments, and the autonomic innervation of the smooth muscle and mucosal components and the somatic nerve supply to the rhabdosphincter component of the external striated urethral sphincter. 23 –25 Yet, suboptimal apical dissection resulting in positive resection margins should always be avoided when trying to preserve the sphincter, particularly in men with more aggressive prostate cancer. In this study, it was not possible to obtain complete, detailed, and relevant information regarding the histology of each patient. A relatively high percentage of locally advanced tumors was assumed, which may have had important impact on the surgical procedure, leading the respective surgeons toward more extensive (apical) dissection, probably resulting in sphincter damage and consecutive urinary incontinence.
It is assumed that external striated urethral sphincteric weakness appears to be the most common reason for postprostatectomy stress urinary incontinence as described by Ficazzola and Nitti 26 who studied 60 consecutive patients with incontinence after prostatectomy and found that 90% of these patients had intrinsic sphincter deficiency with a positive predictive value of 95%. An irreversible injury with scarring of the affected muscle tissue as shown in this study is likely to be the result of iatrogenic sphincter damage. To optimize the procedure of RP and avoid sphincter damage implementing the strategy of avoidance while performing the vesicourethral anastomosis, Libertino and coworkers 27 could show feasibility of a method creating a sutureless anastomosis.
Conclusions
Direct iatrogenic damages to the urethral sphincter are a potential reason for postprostatectomy urinary incontinence, although they are very seldomly communicated. They are likely to follow a particular local distribution pattern, indicating that apex preparation and building of the urethrovesical anastomosis show an increased risk for these sphincter injuries. Cystoscopic evaluation of the sphincteric region in incontinent patients after surgery may be a valuable tool for examination.
Footnotes
Disclosure Statement
No competing financial interests exist.