
Abstract
Background and Purpose:
The incidence of incisional hernia after robot-assisted radical prostatectomy (RARP) has not been described previously. We report our prospective data in an attempt to identify factors that may predispose to this important complication.
Patients and Methods:
The information contained in our prospectively collected RARP database was used to assess the incidence and predisposing factors for incisional hernia post-RARP in a single surgeon series of 250 patients.
Results:
The incidence of incisional hernia in our series was 4.8% (12 of 250 patients). Statistical analysis demonstrated a higher rate of incisional hernias in patients for whom the supraumbilical incision for specimen retrieval was closed with a continuous, rather than interrupted suture. Incisional hernia is associated with a significantly longer length of hospital stay.
Conclusion:
Urologists should be aware that incisional hernia is an important postoperative complication after RARP. Closure of linea alba with a nonabsorbable suture using an interrupted technique may help to minimize the incidence of this morbid complication.
Introduction
Patients and Methods
A database of outcomes related to RARP has been maintained at our institution. Patients provided informed consent after institutional ethical approval from The University of Western Ontario (13086E). Information has been collected prospectively on standardized data collection forms. Our database captured preoperative, intraoperative, and postoperative data. All patients were treated and reviewed postoperatively by a single surgeon (SP) with only one patient opting for follow up out of province. The primary aim of the study was to identify factors that predispose to incisional hernia post-RARP.
The technique of RARP with its various modifications has been thoroughly described in previous reports. 1 With the exception of one case that was performed extraperitoneally early in our series, surgery was performed at our institution via a transperitoneal antegrade approach with early division of the bladder neck. RARP was performed with a three-armed robot for the first 72 cases and subsequently with a four-armed device. The location of each of the six ports for the three- and four-armed robots is demonstrated in Figures 1 and 2, respectively.

Placement of ports for three-armed technique.

Placement of ports for four-armed technique.
Initial pneumoperitoneum was achieved in each case at the left upper quadrant by a Hasson technique. 2 The anterior rectus fascia was divided with cautery and the edges sutured with #1 polyglactin (Vicryl,™ Johnson & Johnson Medical Ltd.) sutures that were left untied for later closure. The posterior fascia and peritoneum were divided sharply. A 12-mm blunt tip trocar with inflatable balloon (AutoSuture,™ Covidien Surgical) was placed and carbon dioxide pneumoperitoneum created. A 12-mm port with dilating tip trocar and retractable blades (Endopath,™ Johnson & Johnson Medical Ltd.) was placed supraumbilically for use as a camera port and a further 12-mm port of the same specifications medial to the left anterior superior iliac spine as an assistant port. Two further 8-mm reuseable ports (Intuitive Surgical) were placed at the right and left lower quadrants for use with the robotic arms. All ports were placed under direct vision to prevent unrecognized visceral injury.
At the completion of surgery, the specimen was placed in a laparoscopic retrieval bag, the robot was undocked, and a Carter-Thomason (CooperSurgical, Inc.) stitch passer was used to close the 12-mm assistant port with #1 polyglactin. The vertical incision at the supraumbilical port was extended for specimen extraction and subsequently closed with #1 polyglactin. This was completed with a continuous suture for the first 122 cases. Since then, an interrupted figure of eight technique has been used. If an umbilical hernia was detected clinically preoperatively, the patient was offered repair, and this was performed at the time of the supraumbilical port closure. The preplaced polyglactin was used to close the 12-mm Hasson port. The dermis was closed with continuous 4-0 polyglactin subcuticular suture and a sterile (Tegaderm,™ 3M Medical) dressing was applied.
There were 12 cases in which the patient had a preexisting umbilical hernia. In these cases, herniorraphy was performed by the attending urologist at the time of supraumbilical port closure. In each case, the fascial defect was exposed and the hernia sac excised. Fascial repair was performed with interrupted nonabsorbable sutures. If an inguinal hernia was noted preoperatively or intraoperatively, no attempt was made to perform a repair, although mesh repair concurrent with RARP has been well described with acceptable outcomes. 3
Postoperative care was standardized as far as possible, including an emphasis on prevention of deep vein thrombosis, early mobilization, and optimization of pulmonary function. Length of stay was calculated from the time of admission, which was usually several hours before surgery to the time of discharge from the hospital. All patients were followed at our institution with the exception of one patient who resided out of province and who opted for telephone follow-up and consultation with his local urologist because of the long travel time involved in attending our center for follow-up. At each follow-up visit, the serum prostate-specific antigen (PSA) was recorded, and the patients were asked about any problems that had developed since their last review. Wound healing was confirmed by clinical examination. Erectile function was evaluated using the International Index of Erectile Function. Urethral stricture and bladder neck contracture were diagnosed with flexible urethroscopy when indicated.
The results generated were statistically analyzed with the Fisher exact test for categorical variables and paired Student t tests for nonparametric data using GraphPad Prism 4 software (Graph-Pad Software Inc). Significance was assessed at P<0.05.
Results
Analysis of our database of 250 patients with a mean follow-up of 35 months revealed 12 cases (4.8%) of incisional hernia. The hernias were diagnosed at a mean of 14.8 months after surgery. All but two hernias occurred at the midline supraumbilical port. Both remaining hernias occurred at the left lateral edge of the rectus at the site of the 8-mm robotic port. Six of the 12 hernias needed repair during the follow-up period, with 2 cases performed as an emergency procedure in the postoperative period. The first of these occurred in association with removal of the wound drainage tube from the site of the left 8-mm robotic port. At the time of drain removal, a small piece of fatty tissue was seen protruding from the wound. This subsequently caused significant port site pain, and exploration revealed a small incarcerated section of omentum. The patient made a complete recovery and was discharged on postoperative day 5.
The second patient presented on day 30 postprostatectomy with clinical evidence of small bowel obstruction. CT demonstrated herniation of a small bowel loop through a defect in the linea alba at the supraumbilical port site (Fig. 3). Laparotomy and small bowel resection were performed, and the patient made an uncomplicated recovery with discharge on day 5 after the second surgery. The remaining four patients needing incisional hernia repair were treated electively and underwent mesh herniorraphy.
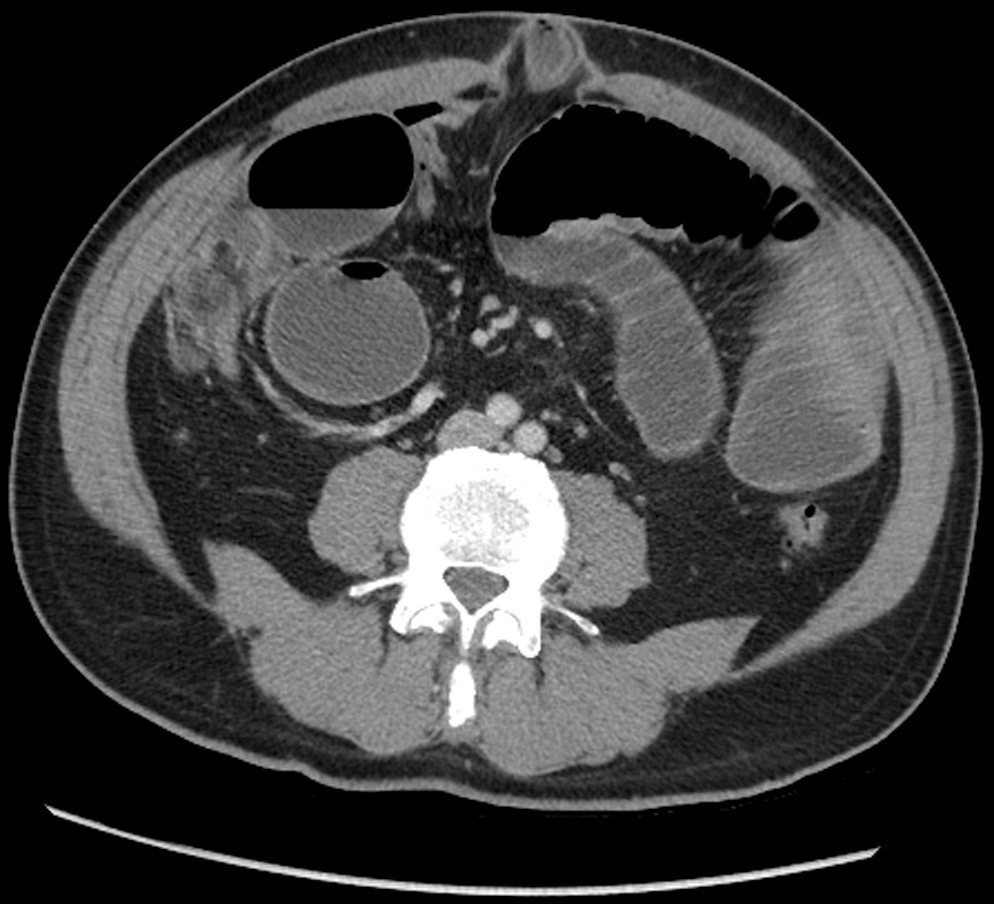
CT demonstrates herniation of the small bowel through the supraumbilical port site with resultant obstruction.
Chronic obstructive airways disease, malnutrition, chronic corticosteroid use, wound infection, renal and hepatic failure have all been associated with a higher risk of incisional hernia. 4 With the exception of one minor wound infection, no patient in our study population was affected by any of the abovementioned conditions. An incisional hernia has not developed in the patient who was treated for the wound infection. None of the patients in whom an incisional hernia developed had a history of diabetes, smoking, previous intra-abdominal surgery, or prolonged postoperative ileus.
Analyses of the subgroup with incisional hernia with regard to preoperative, intraoperative, and postoperative variables are outlined in Table 1. Analysis of pretreatment variables including age, index PSA, transrectal ultrasonography estimated prostate volume, and body mass index demonstrated no statistically significant difference between the two groups. We hypothesized that those with preexisting umbilical hernias, of which there were 12 in our series, may be more prone to the development of incisional hernias after RARP, although the results fail to demonstrate any significant difference in this regard within the limits imposed by a small number of patients for analysis. No significant difference between the two groups was seen with regard to duration of surgery, time needed for port placement/robot docking, and estimated intraoperative blood loss. The first 122 patients, whose incisions were closed with continuous polyglactin, were found to have a significantly higher rate of incisional hernia (P<0.05) in our series when compared with those closed using an interrupted suture technique (Table 2).
P=0.017.
Predictably, patients with incisional hernias had a significantly longer length of stay (4.25 vs 3.11 days, P=0.047). The potential role for bladder neck contracture with delayed incisional hernia was reviewed, although no statistically significant association was demonstrated. Likewise, postoperative urine leak failed to predict an increased likelihood of incisional hernia.
Discussion
The widespread acceptance of RARP as an alternative to ORP results from its ability to provide improved vision, reduced morbidity, shorter recovery time, and equivalent functional and oncologic outcomes. 1 The number of patients who opt for RARP has increased substantially over the past decade. Major adverse effects, including erectile dysfunction and incontinence, are well recognized, although the rates and types of hernia that are associated with RARP are much less well defined. An incidence of inguinal hernia of 7% to 21% 5 –9 after ORP was first described by Regan and associates 10 in 1996. This compares with an incidence in the general population of approximately 5%. Subsequent studies have confirmed these findings, although the exact mechanism remains elusive. The importance of hernia postprostatectomy is reinforced by the high rate of associated additional surgical intervention for repair.
Although the incidence has not been described before this study, incisional hernias contribute significantly to the morbidity of RARP when they occur. The cumulative incidence of incisional hernia in the context of midline laparotomy varies between 9% and 19%. 11 –13 It is therefore not surprising that such hernias are seen in the context of RARP performed via a transperitoneal approach with disruption of the linea alba. This approach theoretically provides a larger working space that facilitates dissection and tension-free vesicourethral anastomosis when compared with an extraperitoneal technique.
Repair of incisional hernias is associated with a rate of recurrence as high as 45%, 14 and as a result, prevention is of paramount importance. Hodgson and colleagues 15 performed a meta-analysis of several methods of abdominal fascial closure and demonstrated a significant reduction in the occurrence of incisional hernia when nonabsorbable sutures were used compared with absorbable sutures with a relative risk reduction of 36% (number needed to treat=50). We propose that the 4.8% rate of incisional hernias seen in our series may be related in part to our use of an absorbable suture material. Our finding of a significantly higher risk of incisional hernia with continuous suturing technique conflicts with the outcomes of the above mentioned meta-analysis.
In recognition of the above literature, we have altered our technique and have commenced using nonabsorbable polyester suture material (Ethibond Excel,™ Johnson & Johnson Medical Ltd.). We plan to review our results in association with this alteration in technique and anticipate a reduction in incisional hernia rates.
With regard to predisposing factors, statistical analysis demonstrated no difference between the two groups with regard to any of the preoperative variables analyzed. Despite this, obesity remains a recognized risk factor for incisional hernia, and we conclude that particular care should be exercised in closing the abdominal fascia in such patients.
Mudge and Hughes 11 demonstrated that 35% of all incisional hernias occur after 3 years in a study that followed patients prospectively over 10 years. Our mean follow-up approaches 3 years, with a minimum follow-up of almost 1 year. It is therefore likely that the rate quoted underestimates the true rate of incisional hernia in this cohort of patients, and we plan to follow our patients for a minimum of 10 years. In addition, this series represents the first 250 cases of RARP performed at our institution. It is possible that the learning curve that is associated with the introduction of this new surgical technique may have influenced the rate of incisional hernia in our study population.
Conclusion
This study emphasizes that despite using a short midline fascial incision, intraperitoneal RARP is associated with incisional hernia. It is our belief that the problem of post-RARP incisional hernia can be better recognized in light of the results presented in this report. We conclude, based on the available literature, that the incidence, morbidity, and cost of hernias may be minimized by fascial closure with nonabsorbable suture material.
Footnotes
Disclosure Statement
No competing financial interests exist.