
Abstract
Purpose:
To evaluate the radial dilation force and basket opening dynamics of three small (<1.5F) stone baskets.
Materials and Methods:
Boston Scientific OptiFlex (1.3F), Cook N-Circle Nitinol Tipless Stone Extractor (1.5F), and Sacred Heart Medical Halo (1.5F) baskets were tested for radial dilation force in 10 repetitions using a floating block atop a stationary block secured to a digital scale. The floating block, attached to a plastic frame and base, pressed down on the scale to measure the radial dilation of the open basket while being passed through the cylindrical opening between the blocks. These same baskets were tested in triplicate for basket width in 0.5- to 2-mm length increments using a mechanical caliper under optical light microscope visualization to evaluate the linearity of basket opening and length at which target basket width (5 mm) was reached.
Results:
The Sacred Heart Medical Halo had the best radial dilation (2.97±0.22 g), followed by the Cook N-Circle (1.29±0.04 g), and finally Boston Scientific OptiFlex (1.19±0.12 g). The N-Circle was the only basket to exhibit linear opening, while the Halo exhibited an exponential curve. The OptiFlex exhibited a polynomial curve, with linear opening across the midrange of the basket length. From these curve equations, the target basket width (5 mm) was calculated. The N-Circle and the OptiFlex reached the target basket width at a basket length of 9.4 mm and 9.6 mm, respectively. The Halo reached the target basket width at a basket length of 11.5 mm.
Conclusions:
The radial dilation force differs significantly among commercial baskets and may affect ureteral stone extraction. Linear basket opening may provide the physician more control in stone retrieval.
Introduction
The relevance of radial dilation force and linear basket opening/closing dynamics has been demonstrated in previously published work looking at baskets of a variety of shapes and designs including tipless and helical. 3,4 In these evaluations, it was found that radial dilation and basket opening/closing dynamics differ significantly among baskets that are commercially available. Each of these physical properties may play an important role in different clinical situations. For example, a high radial dilation force would be desirable in cases where the stone is located in an edematous or strictured ureter. A linear opening dynamics would provide greater control of the basket and maintain the tip within the field of view.
The objective of this study was to evaluate three new nitinol stone extraction baskets of a smaller caliber (≤1.5F) than those previously tested (≥1.9F). 3,4 A comparative study on basket dynamics such as this may help predict clinical performance of baskets under certain conditions during caliceal and ureteral stone extraction. 5,6
Materials and Methods
Stone baskets that were evaluated included the Boston Scientific OptiFlex™ (1.3F), Cook N-Circle® Nitinol Tipless Stone Extractor (1.5F), and Sacred Heart Medical Halo™ (1.5F). Four baskets of each manufacturer were tested. Evaluations included radial dilation force, basket opening/closing dynamics, and length to reach target basket width (TBW) of 5 mm. Methods of testing for radial dilation are described in detail in a previous publication. 3
Two Teflon blocks (1.0×0.55×0.325 inches) were positioned with the lower block sitting on a digital scale (400×0.1-g capacity) and the upper block secured to a plastic frame and base (Fig. 1). The digital scale was calibrated to 0 with the lower block in place, and then the upper block was lowered onto the bottom block. A 0.01-inch gap was maintained between the blocks using a digital micrometer. Alignment pins secured the lower block in relation to the upper block. Each basket was passed through the cylindrical hole and opened to its fully extended length. The basket was then slowly pulled through the hole, and the maximum force reading was recorded. Ten repetitions of radial dilation force testing were performed for each basket.

Experimental setup for evaluating radial dilation force.
Length vs width measurements were taken to evaluate basket opening/closing dynamics, including linearity of opening and closing and also to determine length at a target basket width of 5 mm. A single operator performed measurements of basket width as the length of the basket was extended in increments of 0.5 to 2 mm starting from the closed position. All measurements were performed using a digital caliper under optical light microscopic visualization (Fig. 2). Graphs were created of basket length vs width and a best fit curve of the data was calculated. A best-fit curve was then fitted to the data. From the calculated trendline equations, the TBW was determined. Statistical analysis of data included analysis of variance-single factor tests and t tests assuming unequal variances for comparing data between baskets.
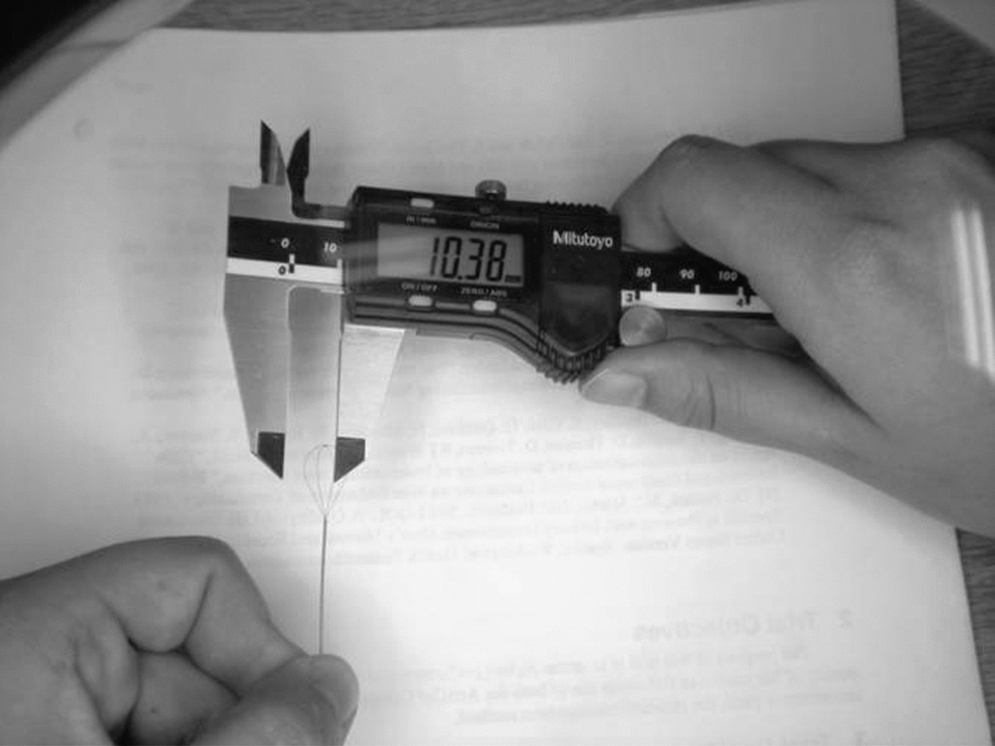
Experimental setup for evaluating opening/closing dynamics.
Results
The Medical Halo 1.5F basket had the strongest radial dilation force, P<0.001 (Fig. 3). Opening/closing dynamics are presented in Figures 4, 5, and 6. The OptiFlex 1.3F exhibited a polynomial curve with very gradual change in basket width in the initial and final lengthening of the basket and a linear opening for the middle portion of the handle excursion. In contrast, the Medical Halo 1.5F exhibited an exponential curve, with little change in basket width with initial movement of the basket handle followed by a rapid increase in basket width. The N-Circle 1.5F exhibited linear opening/closing dynamics. Finally, the length to reach the TBW of 5 mm was significantly greater for the Medical Halo (11.5 mm, P<0.0001) than the N-Circle (9.4 mm) or OptiFlex (9.6 mm) baskets.
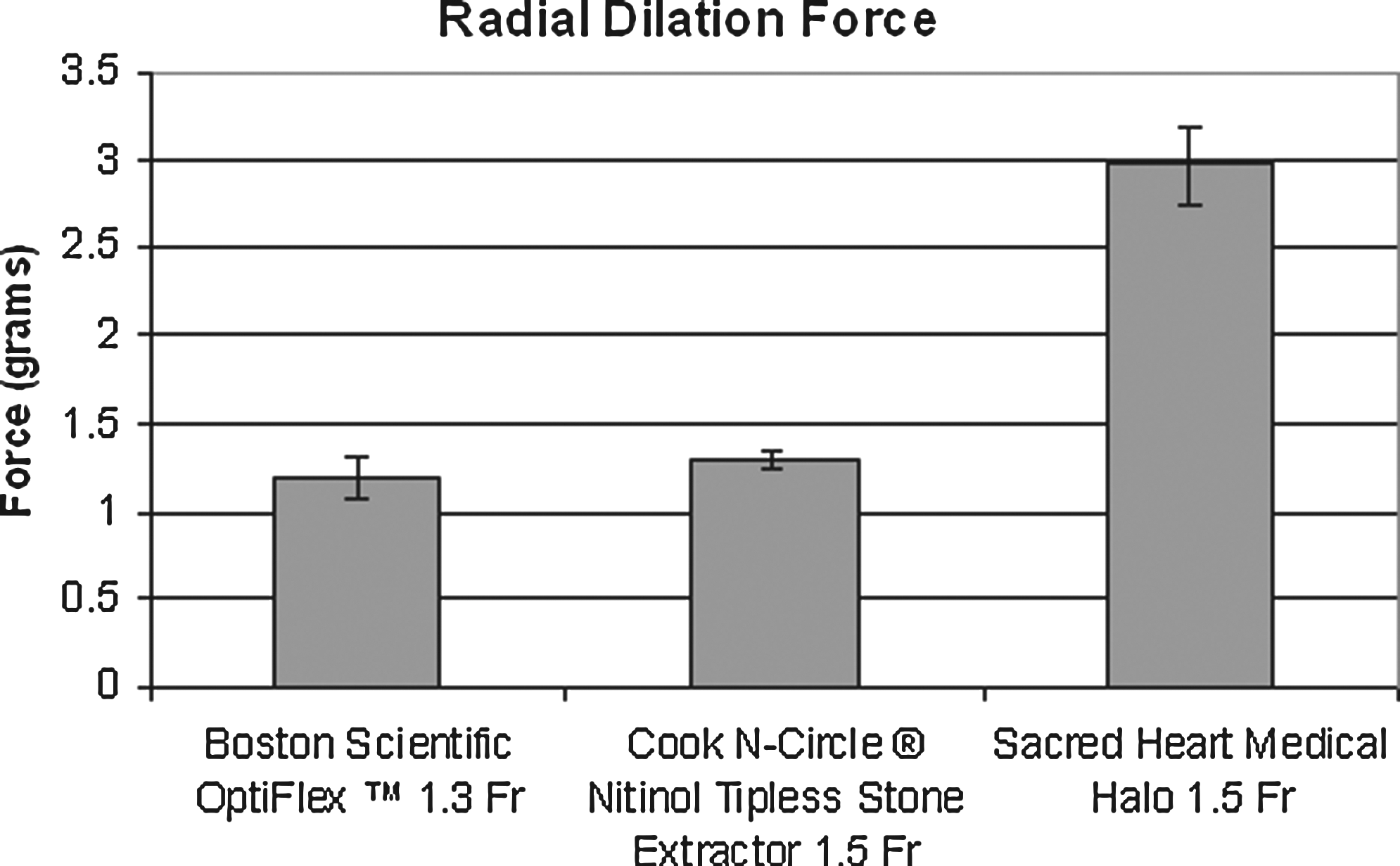
Radial dilation force.

Boston Scientific OptiFlex 1.3F exhibited polynomial opening dynamics when basket width was plotted against basket length.
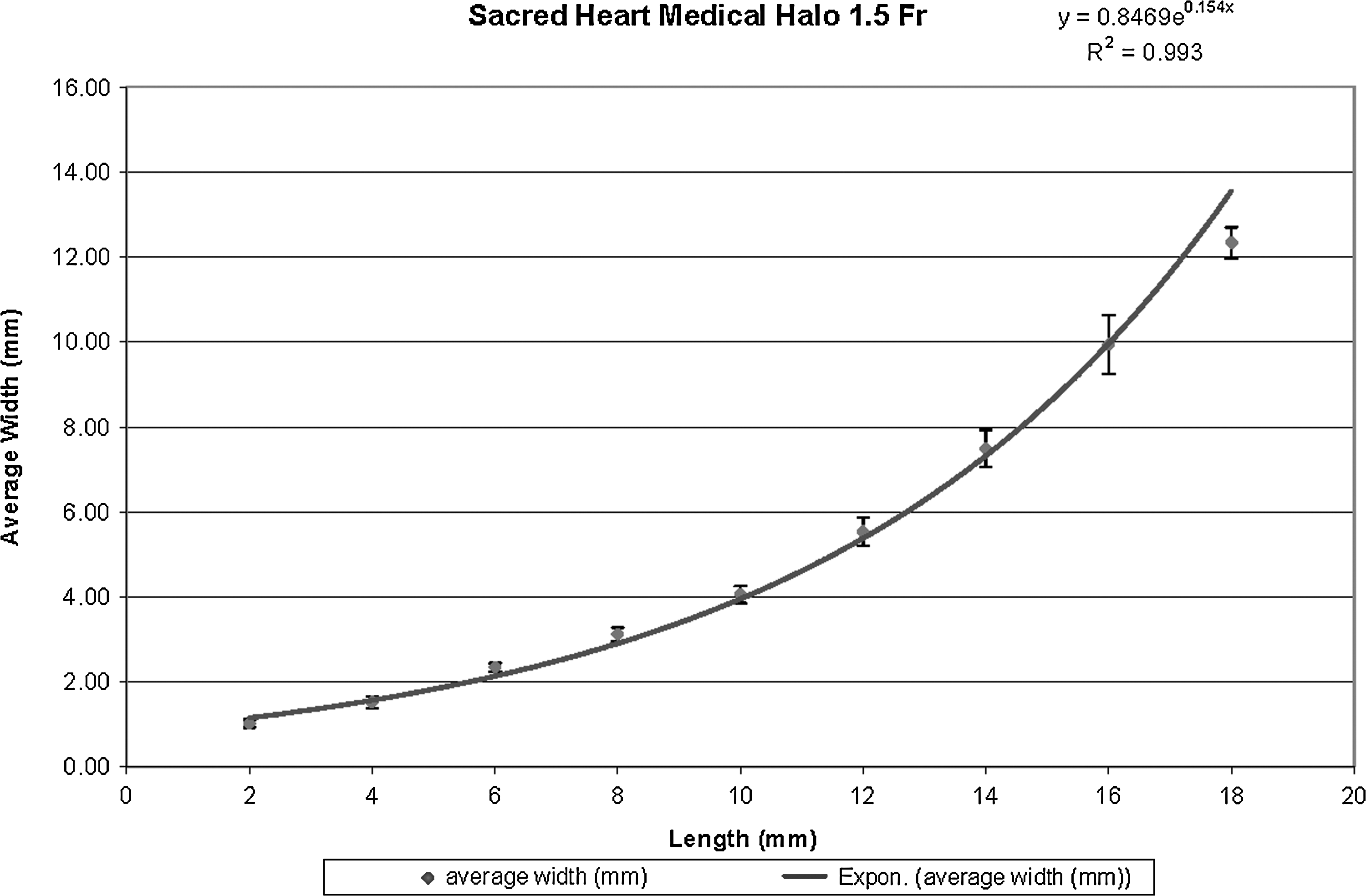
Sacred Heart Medical 1.5F exhibited exponential opening dynamics when basket width was plotted against basket length.
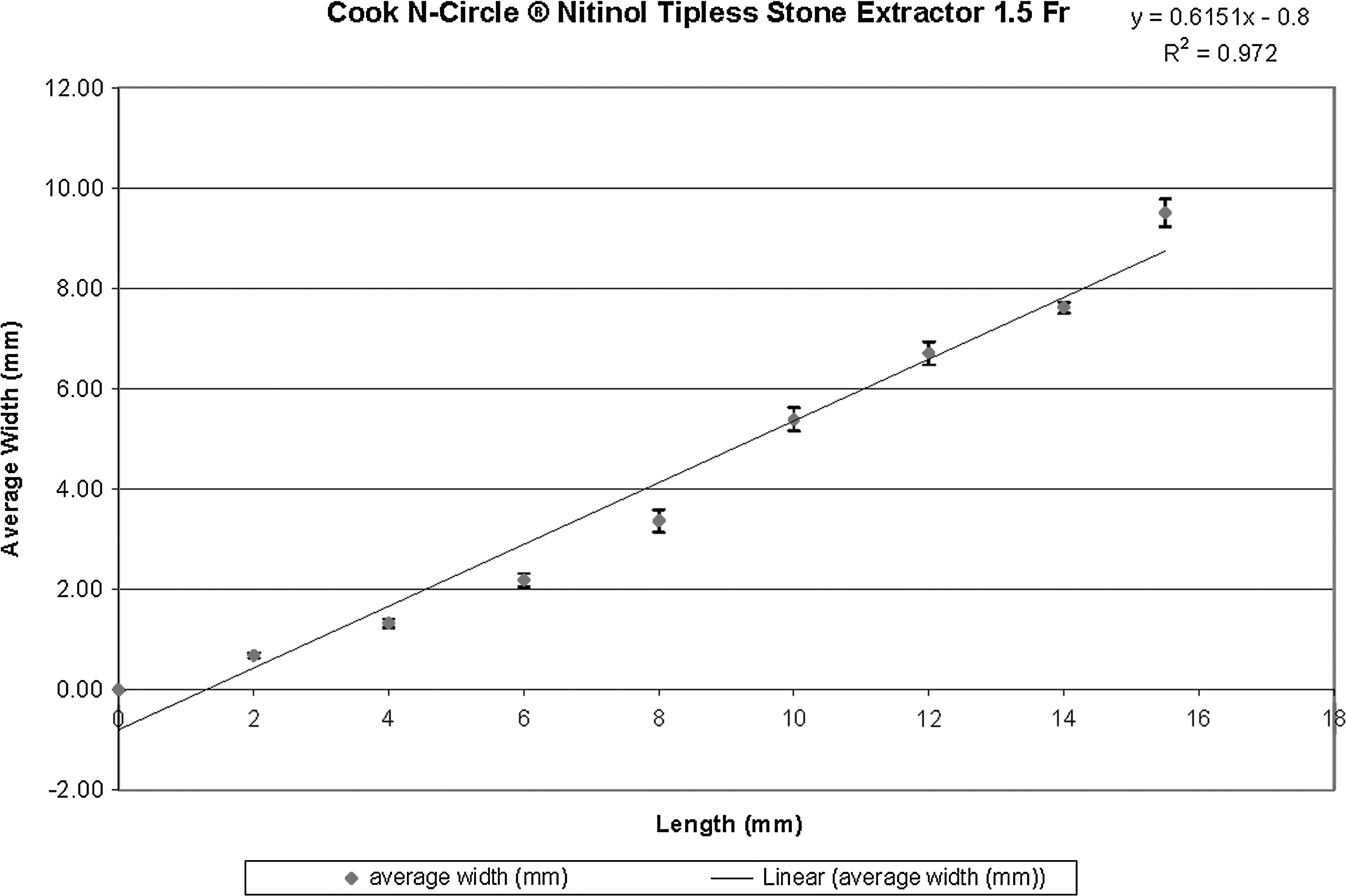
Cook N-Circle Nitinol Tipless Stone Extractor 1.5F exhibited linear opening dynamics when basket width was plotted against basket length.
Discussion
Previous studies have compared the radial dilation force and basket width dimensions with tipless and helical baskets. 3,4 Our objective was to re-evaluate these parameters for three next-generation baskets that are ≤1.5F in outer diameter. The Halo 1.5F had the strongest radial dilation force of the baskets tested in this evaluation, suggesting that it may be more likely to open if faced with a stone in an edematous or strictured ureter. It is important to note that these radial dilation forces are markedly lower than those recorded for baskets 1.9F or larger. Measurements of radial dilation have successfully predicted the performance of stone baskets in an in vitro ureteral model. 5
The Halo demonstrated exponential opening dynamics and needed the longest length to reach a TBW of 5 mm, the minimum necessary to capture a 5-mm stone. We hypothesize that a shorter TBW and linear opening dynamics would allow the tip of the basket to remain in view and provide the greatest control to the surgeon during opening and closing. While the N-Circle was the only basket to demonstrate linear opening/closing dynamics, the OptiFlex demonstrated polynomial opening/closing dynamics, with linear opening across the majority of the basket excursion and slower opening at each extreme (initial opening and final opening). 4
As technology advances and the endourologist's tools continue to become miniaturized, ongoing reevaluation of form and function is necessary. 7,8 We have recently noted a marked increase in reports of stone retrieval device failures to the Food and Drug Administration, which may be related to increased use or perhaps to the development of smaller albeit more fragile devices. 9 Indeed, the deformation of baskets with multiple passes through a port seal and multiple deployments for stone extraction is a new variable that needs further study for this small class of stone baskets.
While small ≤1.5F baskets provide advantages with regard to ureteroscope deflection and irrigant flow, it is important that features important for clinical utility, such as radial dilation, opening dynamics, and durability, are not compromised. Benchtop testing provides one method to evaluate and predict clinical performance. Although these studies systematically compare baskets with standardized in vitro testing, they do not provide “clinically proven” benchmark values for how much radial dilation force is needed in a clinical setting; indeed, further validation in a clinical or animal study is warranted.
Conclusion
As stone baskets become smaller, there is a similar reduction in radial dilation force that may challenge ≤1.5F stone baskets to perform in tight spots. It is unclear to what extent this will pose a limitation to clinical practice, although in this clinical situation, one might consider using a larger basket. Furthermore, baskets that incorporate linear opening/closing dynamics may facilitate efficient stone capture and release while maintaining the basket in the field of view. Further research in the clinical setting and surgical simulation settings will lead to a better understanding as to how these measured basket characteristics correlate to successful stone extractions. Recognizing these differences in basket performance may lead to the development of novel basket configurations.
Footnotes
Disclosure Statement
Dr. Monga is a consultant for Cook Urological, Boston Scientific, and Olympus-ACMI. The other authors have no conflicts of interest to declare.