
Abstract
Purpose:
To introduce a novel, two-port laparoscopic technique for treatment of hydrocele in children, which allows completely extraperitoneal closure of the patent processus vaginalis (PPV) and does not necessitate laparoscopic suturing skills.
Patients and Methods:
We describe a consecutive series of 56 boys with a median age of 36 months (range 12–144 mos) who presented with a presumably communicating hydrocele. Laparoscopic repair of these hydroceles was performed between July 2009 and June 2010. During surgery, a 5-mm laparoscope and a 3-mm grasping forceps were inserted through an identical umbilical incision (10 mm). The hydrocele sac orifice was closed extraperitoneally by circuit suturing around the internal inguinal ring.
Results:
All cases were preoperatively diagnosed to be unilaterally based on physical examination and ultrasonography. During surgery, 17 of the 56 (30%) patients presented a contralateral PPV. A total of 73 laparoscopic procedures were achieved, with a success rate of 100%. The mean operative time was 25±6 and 36±5 minutes for unilateral and bilateral operations, respectively. During a median follow-up period of 6 months (range 1–12 mos), neither recurrence nor other postoperative complication was encountered.
Conclusions:
Our limited experiences suggest that the two-port, totally extraperitoneal laparoscopic technique could be a safe, effective, and reliable alternative for management of pediatric hydrocele.
Introduction
Once diagnosed, a hernia is recommended to be surgically treated as soon as possible. In contrast, hydrocele repair is preferred to be performed after the patient is 1 year of age, because some hydroceles can spontaneously resolve by the first few months of life. 1 For many decades, conventional open surgery has been widely used in hydrocele/hernia repair in children, which typically involves creation of a groin incision, exposure of the inguinal canal, and high-ligation of the PPV.
Recently, laparoscopic surgery has been increasingly used to manage pediatric inguinal hernias. 2 –7 This minimally invasive technique has the advantages of diminished postoperative pain, faster recovery, and better cosmesis compared with the conventional open procedure. 8 –10 Most importantly, this procedure easily allows contralateral exploration and simultaneous closure of the contralateral PPV, avoiding additional wounds. Despite extensive studies on laparoscopic hernia repair, relatively few have been performed to evaluate the applications of laparoscopic surgery for hydrocele.
In this study, we described a technique of laparoscopic extraperitoneal hydrocele repair that necessitates two ports inserted through one 10-mm umbilical incision and a 2-mm skin puncture wound. We reviewed the outcomes of 56 boys with symptomatic hydrocele undergoing laparoscopic repair at a single institution to assess the technical feasibility and efficiency.
Patients and Methods
We retrospectively reviewed a consecutive series of 56 boys with a markedly dilated scrotum, who underwent laparoscopic repair at the department of urology of the Third Affiliated Hospital of Sun Yat-sen University in China between July 2009 and June 2010. Data were collected from medical records and personal interviews. The principal outcome parameters included age, side of hydrocele, operative time, presence of contralateral PPV, length of hospital stay, and postoperative complications.
The patients had a median age of 36 months (range 12–144 mos). All cases were preoperatively diagnosed to be unilateral based on a physical examination and ultrasonography; 34 (61%) were right-sided, and 22 (39%) left-sided. Ultrasonography as a noninvasive tool is commonly used to examine the affected testis and to rule out a tumor or other conditions. Three patients had previous open surgery for repair of contralateral hernias. During the operation, 17 of the 56 (30%) patients were found to have a contralateral PPV.
All operations were performed under general anesthesia with tracheal intubation. The patients were placed in the Trendelenburg position (20-degree head-down tilt). The surgeon operated by standing on the contralateral side of the symptomatic hydrocele, and the assistant was on the ipsilateral side. The monitor was positioned at the patient's feet. A 10-mm umbilical incision was made, and a 5-mm trocar for the laparoscope was inserted into the peritoneal cavity through the umbilicus via an open (Hasson) technique.
After carbon dioxide insufflation to create a pneumoperitoneum with a pressure of 8 to 12 mm Hg, a 5-mm, 30-degree laparoscope (Stryker, Kalamazoo, MI) was introduced. A 3-mm trocar was advanced along the left side of the 5-mm cannula via the same umbilical incision (Fig. 1). The two trocars were placed under direct vision, avoiding injury to the abdominal organs. The corresponding skin of the opening of the processus vaginalis was marked by means of the laparoscope. At the marked site, a 2-mm skin incision was made, through which an 18-gauge vascular access needle (Vasocan, Braun Melsungen AG, Melsungen, Germany) was introduced to the preperitoneal space over the vas deferens and spermatic vessels, followed by injection of 10 mL of physiologic saline to this space for the preperitoneal dissection. The needle was then withdrawn.

Two ports inserted through an identical umbilical incision, one for a 5-mm laparoscope and the other for a 3-mm grasping forceps.
A 7-0 silk suture was threaded through an 18-gauge Vasocan hollow needle without an outer plastic sheath, and its free arm was passed through with a 2-0 nonabsorbable polyester thread (Fig. 2). Through the previous skin incision, the Vasocan needle with the two stitches was introduced along the preperitoneal space on one side of the processus vaginalis defect and passed into the intra-abdominal space (Fig. 3A). One end of both the sutures was left outside the skin. Within the peritoneal cavity, the silk suture in the hollow needle was grasped and separated from the 2-0 polyester suture by a grasping forceps inserted from the 3-mm umbilical port. The polyester suture was left in the peritoneal cavity, while the needle with the silk suture was withdrawn outside the peritoneum but below the abdominal wall (Fig. 3B). The needle was reintroduced along the opposite side of the processus vaginalis defect into the intra-abdominal space, where the silk suture formed a U-shaped loop. The intraperitoneal end of the polyester thread was brought into the formed loop, and then pulled out of the abdomen when the needle was withdrawn (Fig. 3C).

Suturing instruments used. A 7-0 silk suture was threaded through an 18-gauge Vasocan hollow needle without an outer plastic sheath (left), and its free arm was passed through with a 2-0 nonabsorbable polyester thread (right).
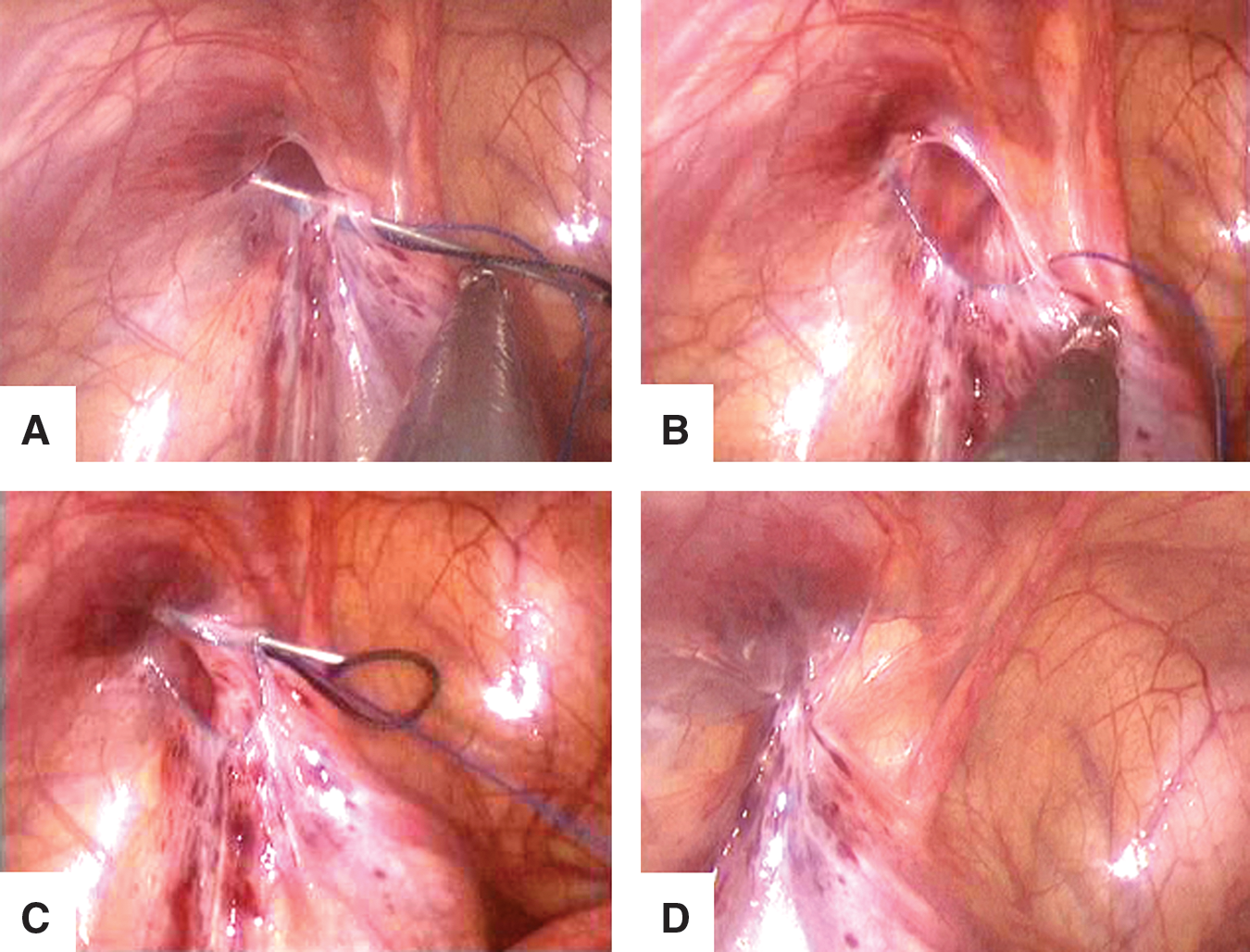
Laparoscopic extraperitoneal repair of hydrocele in a 2-year-old boy.
After the abdomen was desufflated, fluid in the scrotum, if any, was pushed back into the peritoneal cavity. Both ends of the 2-0 polyester suture encircling the internal ring defect were tied extracorporeally, allowing a complete extraperitoneal ligation of the PPV (Fig. 3D), and the knot was buried subcutaneously. A schematic diagram for the laparoscopic closure of the PPV is depicted in Fig. 4. If a contralateral PPV was present, it was simultaneously closed using the same procedure.
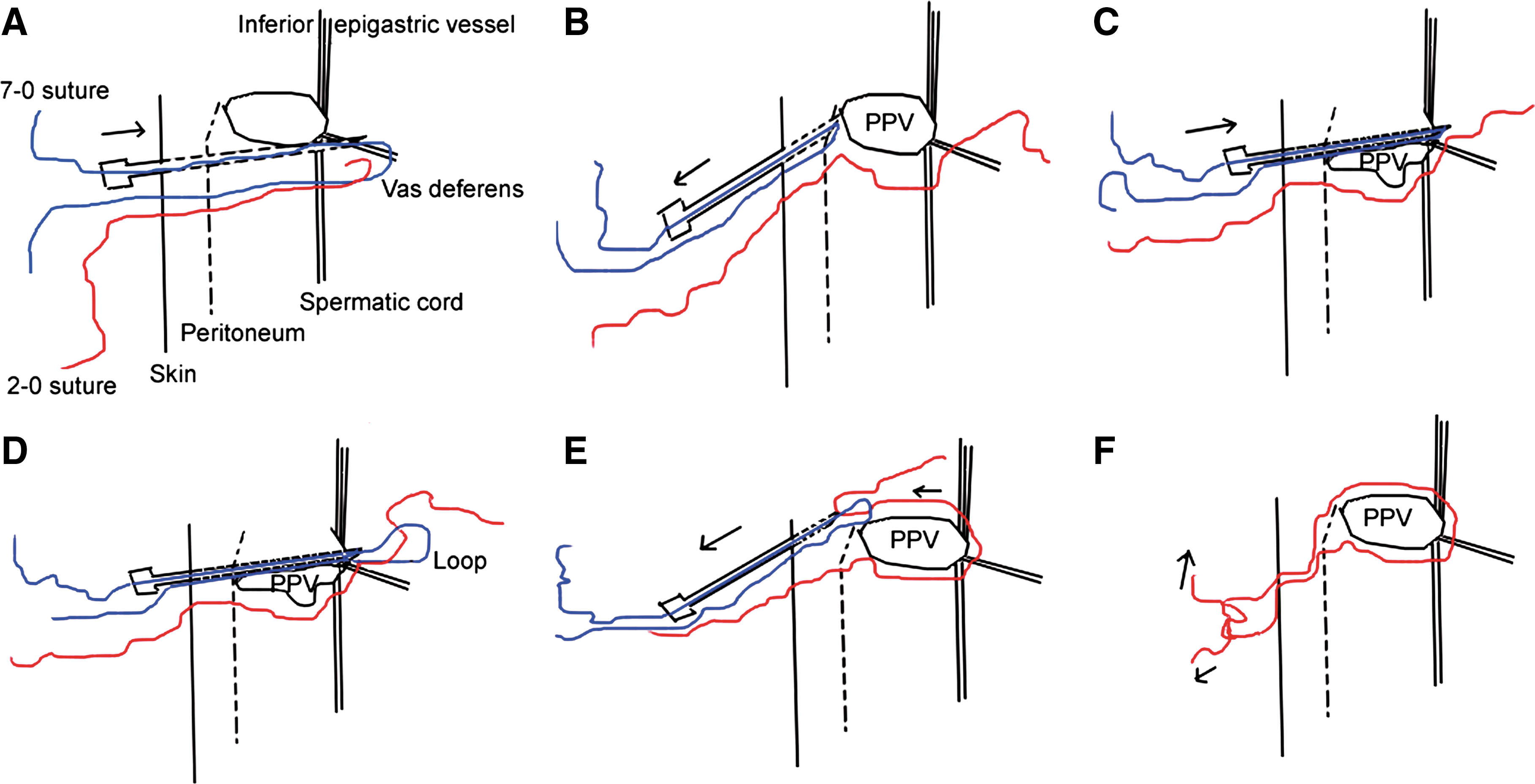
Schematic illustration of the laparoscopic technique for extraperitoneal ligation of the patent processus vaginalis (PPV).
In our series, 12 (21%) patients had a noncommunicating hydrocele. For them, the drainage of fluid from the cyst was achieved using an 18-gauge catheter needle after high-ligation of the PPV. The umbilical wound was closed with absorbable stitches, while no stitch was needed for the skin incision.
Twenty-five of the 56 (45%) patients received oral acetaminophen (15 mg/kg) for postoperative pain control. The patients were followed for a median time of 6 months (range 1–12 months), and no one was lost to follow-up. Postoperative complications (ie, incisional hernia, scrotal hematoma, testicular atrophy, and recurrence) were evaluated.
Results
Table 1 summarizes the clinical characteristics of the series and surgical results of laparoscopic repair. A total of 73 laparoscopic procedures were performed, and the clinical success rate was 100%. The mean operative time was 25±6 and 36±5 minutes for unilateral and bilateral operations, respectively (Table 1). All of the patients could be discharged within 24 hours after surgery. The duration of abdominal pain or discomfort never exceeded 24 hours. The mean number of days taken to return to normal activities after surgery was 43.2±5.1 hours. During the follow-up period, neither recurrence nor other postoperative complication was observed.
PPV=patent processus vaginalis.
Discussion
Hydrocele is a common condition in children, usually as a result of PPV. Most idiopathic hydroceles can resolve without surgery within the first year of life because of spontaneous closure of the PPV. 1 An operation will be needed if the hydrocele persists for a longer time. Our patients underwent surgery at a median age of 36 months (range 12–144 mos). Age at presentation seems to have no effect on resolution, because satisfactory results were achieved in all our patients.
The principle for surgical correction of pediatric inguinal hernia and hydrocele is the same, which consists of complete ligation of the PPV. In recent years, laparoscopic inguinal hernia repair has become more and more popular, because of minimized invasiveness, simultaneous closure of the contralateral PPV, and better cosmetic results. 11,12 Many laparoscopic procedures have been proposed, which vary considerably in their approaches to the internal ring (intraperitoneal, extraperitoneal), use of ports (three, two, one), endoscopic instruments (two, one, or none), sutures (absorbable, nonabsorbable), and techniques of knotting (intracorporeal, extracorporeal). 5
These techniques are continually evolving, with a trend toward increasing use of extracorporeal knotting and decreasing use of working ports and endoscopic instruments. A relatively higher recurrence rate has been documented in laparoscopic hernia repair using intracorporeal suturing technique. 13,14 Recurrence may be related to the skip areas during placement of purse-string sutures as well as the tension resulting from intracorporeal knotting, particularly in closure of large defects. The use of extracorporeal knotting has been proposed to reduce the rate of recurrence. 7,15 The present technique is an extracorporeal approach, which overcomes the need for intracorporeal suturing and knotting. During the median follow-up period of 6 months, there was no recurrence observed in our series.
Although a simpler, single-port laparoscopic-assisted technique has been introduced to close inguinal hernia and yields a near-zero recurrence rate, 16,17 here we used a two-port technique—one port for laparoscopy and the other for grasping forceps—which is similar to that described previously. 7,18 Hydrodissection is used in the present technique to separate the peritoneum from the vas and vessels and allow the needle to pass through the preperitoneal space. This approach, however, cannot ensure a complete separation of the peritoneum, and some gaps may be present, therefore raising the possibility of recurrence. Grasping forceps not only makes intraperitoneal handling easier, but also helps the needle pass through the preperitoneal space without skipping any area during placement of the suture so that the inguinal ring is totally encircled. Moreover, the application of grasping forceps seems not to increase the risk of intra-abdominal complications, and indeed, no serious intraoperative and postoperative complication was observed in this setting.
To achieve a better cosmetic outcome, we placed the two ports through the same 10-mm umbilical incision. The mean operative time for unilateral repair is similar to that achieved with the single-port technique, 16 while slightly less operative time for bilateral repair is obtained in the present procedure.
A laparoscopic technique makes it possible to simultaneously close a contralateral PPV, thereby preventing a second operation and reducing both economic burden and procedural risks to patients. In our series, 30% presented with an asymptomatic contralateral PPV, which is comparable to the results of others. 13,15 A noncommunicating hydrocele was observed in 21% of our patients. For them, simple needle aspiration after high-ligation of the PPV was performed. No recurrence occurred within a limited follow-up period. Our use of the drainage technique after laparoscopic repair instead of hydrocelectomy, the standard treatment for hydrocele, is based on the assumption that pediatric hydroceles are mainly the result of a congenital PPV. Moreover, aspiration is a minimally invasive approach that is simple, inexpensive, and safe. 19 We cannot preclude the possibility, however, that some cases may be caused by other unknown factors rather than by the PPV. Thus, a longer follow-up was needed to definitely evaluate the efficacy of this technique in treating noncommunicating hydroceles in children.
Conclusions
We described a novel, two-port laparoscopic technique for extraperitoneal repair of hydrocele in children. This technique is easy to perform and does not necessitate laparoscopic suturing and intracorporeal knot-tying skills. Satisfactory outcomes coupled with a near-zero recurrence rate are achieved.
Footnotes
Disclosure Statement
No competing financial interests exist.