
Abstract
The emergence of robot-assisted surgical technology has permitted application of laparoscopic pyeloplasty to the pediatric age group to a much wider degree than previously possible. The challenging learning curve for conventional laparoscopic pyeloplasty, particularly in infants, has hindered its widespread application. Robot-assisted pyeloplasty in children has been clearly shown to provide an equally effective, safe, and reasonably efficient means to repair ureteropelvic junction obstruction with more rapid hospital discharge and less postoperative analgesic requirements. Precise port placement, adjusted to the child's anatomy and size, delicate anastomosis, and use of postoperative stent appear to be important elements for successful repair. The procedure has become reproducible and in some centers is exclusively used over open repair. The specific procedural steps are detailed and the potential limitations and complications are reviewed, as well as the limited available data in the literature.
Introduction
Indications and Contraindications
The indications for robot-assisted pyeloplasty in a child are identical to those for any pyeloplasty and, at present, there are few age restrictions, except perhaps the very small newborn. Children from 5 kg and up have been treated successfully using the current system, and there is little reason to restrict its use. The relative advantages of robot-assisted surgery may not be as apparent in the infant as the teen, but there is no clear way to draw an age cutoff. Reoperative cases, while challenging to select and perform with any method, are well suited to robot-assisted surgery. The optimal indication for pyeloplasty in a child remains controversial, but the author's practice has been to recommend this in children with symptomatic ureteropelvic junction (UPJ) obstruction, declining relative uptake on a diuretic renogram, progressive hydronephrosis, or lack of substantive improvement in the first 2 years of life, and parental preference. UPJ obstruction with renal calculi is an ideal use for the robotic system. 1 Renal malformations are unlikely to cause problems as long as the anatomy can be defined preoperatively. We have performed pyeloplasties in several children with horseshoe kidneys, intrarenal pelvices, and duplication anomalies.
Contraindications are few and may be the small newborn with severe obstruction of a solitary kidney. Multiple previous intra-abdominal procedures may limit transperitoneal access, and retroperitoneal access in the smaller child is difficult.
Preoperative Workup
Patients have nearly always undergone diuretic renography to document the level of uptake in the affected kidney, ultrasonography (US) to demonstrate the anatomy of the renal pelvis and the absence of distal ureteral dilation. Infants have typically undergone voiding cystourethrography, although this may be optional in the older child. The need for further imaging is dependent on the clinical scenario and the ability to define anatomy by US and renal scan. If there is uncertainty as to the renal and ureteral anatomy, magnetic resonance urography or even intravenous urography may be used.
Retrograde ureteropyelography is also an option to define ureteral anatomy if there is any question, and this is always performed if a retrograde stent is to be placed (see below). It is unlikely to reveal any critical factors.
Preoperative Preparation
Patients are placed on a clear liquid diet for 24 hours before surgery and given a laxative or suppository to debulk the rectosigmoid. Antibiotics are administered at anesthesia induction.
A bladder catheter is placed, and the patient is positioned on the table with a wedge under the ipsilateral flank and then securely taped to the table. This permits rotation of the table to provide for the abdomen to be horizontal with the floor for port placement and then tilted to allow renal exposure. The degree of tilt is adjusted after the first port is placed to permit direct vision of the renal area.
Instrumentation
Pediatric robot-assisted pyeloplasty only needs four robotic instruments. Routine use of an assistant port is unnecessary, although a single laparoscopic Maryland grasper or needle driver is used to pass the needles into the working field. Robotic instruments may be 8 or 5 mm, depending on the size of the child; we use the 5-mm instruments up to age 7 or 8 years. Those used are a Maryland dissector, hook cautery, scissors, and needle driver. When using the 8-mm instruments, the monopolar scissors are used along with the bipolar Maryland. With the introduction of the 8.5-mm binocular endoscope, the 12-mm endoscope is no longer the only option. These instruments are all reusable for their allotted lifetime (15 to 20 uses for the 5-mm and 10 for the 8-mm instruments).
Surgical Steps
Pyeloplasty should be a very consistent, stepwise procedure, adherence to which will improve the likelihood of success. The initial decision is whether a stent will be placed retrograde, in which case it is placed with a withdrawal string to permit removal without cystoscopy, usually 2 weeks postoperatively. Some children will not be very tolerant of this, and most parents can predict this, in which case the stent is placed antegrade during the procedure.
For retrograde preplacement of the stent, cystoscopy is performed with retrograde ureteropyelography. Optimally, the stent is placed just up to the UPJ so that the renal pelvis remains dilated. This may not be always accomplished, but facilitates identification of the pelvis and UPJ.
The patient is then positioned with a wedge on the ipsilateral side and strapped to permit full rotation of the bed. This allows positioning of the patient to optimize exposure of the pelvis under direct vision before the last port is placed. Particularly in small children, port placement is critical, and the lower port must be located far enough away from the UPJ to permit full range of motion. If too close, the articulation will not be permitted to function fully.
Access
Access is attained using an open technique at the inferior edge of the umbilicus. The fascia is divided progressively until the peritoneal space is clearly seen. At this point only is a box-stitch of 3-0 or 2-0 absorbable suture placed, which facilitates cannula placement and closure. The endoscope cannula (12 or 8.5 m) is placed, and pneumoperitoneum is created to a pressure of 12 mm Hg and a flow of 6 L/min. The peritoneum is then inspected with the endoscope to ensure no injuries have occurred.
The second port is placed in the midline between the umbilicus and xyphoid using a preplaced fascial box-stitch and the noncutting cannula obturator. With the first two ports in place, the operating table is rotated with the ipsilateral side up to permit renal exposure. A laparoscopic grasper is used to push the small bowel away to reveal the renal pelvis, if possible. The degree of rotation is adjusted to optimize exposure. On the left, this is usually transmesenteric, while on the right, the hepatic flexure of the colon will usually need to be mobilized. Often, the bulging renal pelvis is readily visible to guide visualization. The axis between the umbilicus and the UPJ serves as the central axis for the robotic instruments, and the third port is then placed accordingly (Figs. 1 and 2).
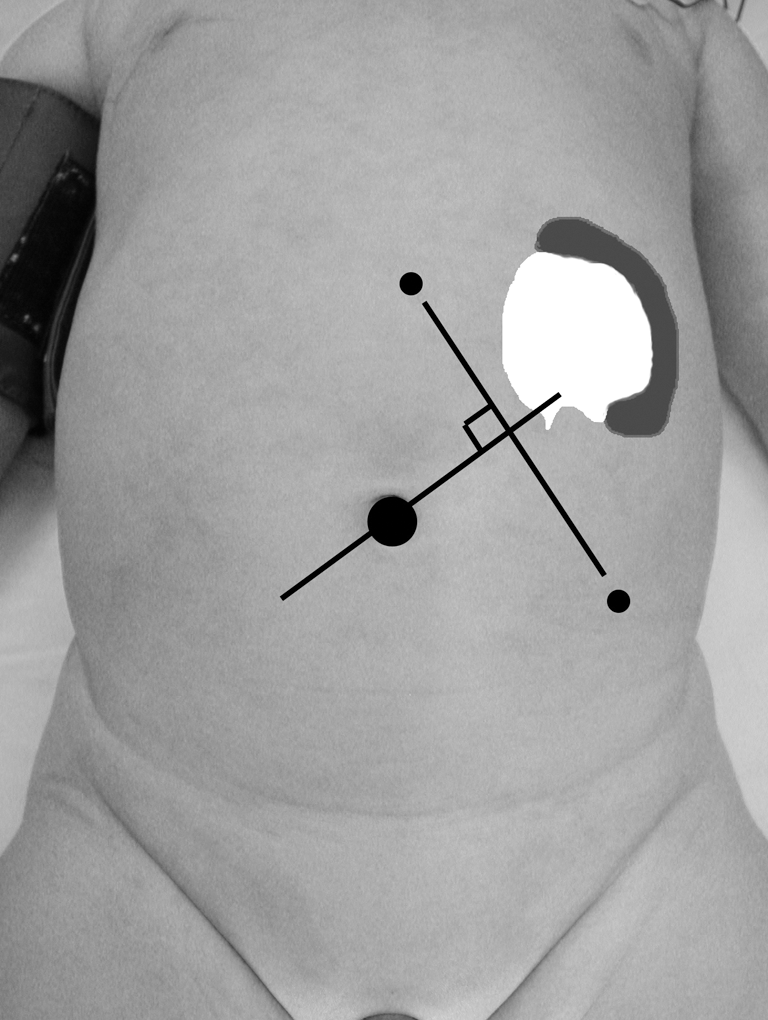
Illustration of port placement for left-sided pyeloplasty in an infant with a smaller renal pelvis. The line of the endoscope, from the umbilicus to the inferior renal pelvis, is the operative axis, and the two working ports are arrayed symmetrically about this with the upper port being in the midline. These port positions are selected with the pneumoperitoneum created and the patient tilted to the degree necessary for exposure. The dilated renal pelvis is usually visible.
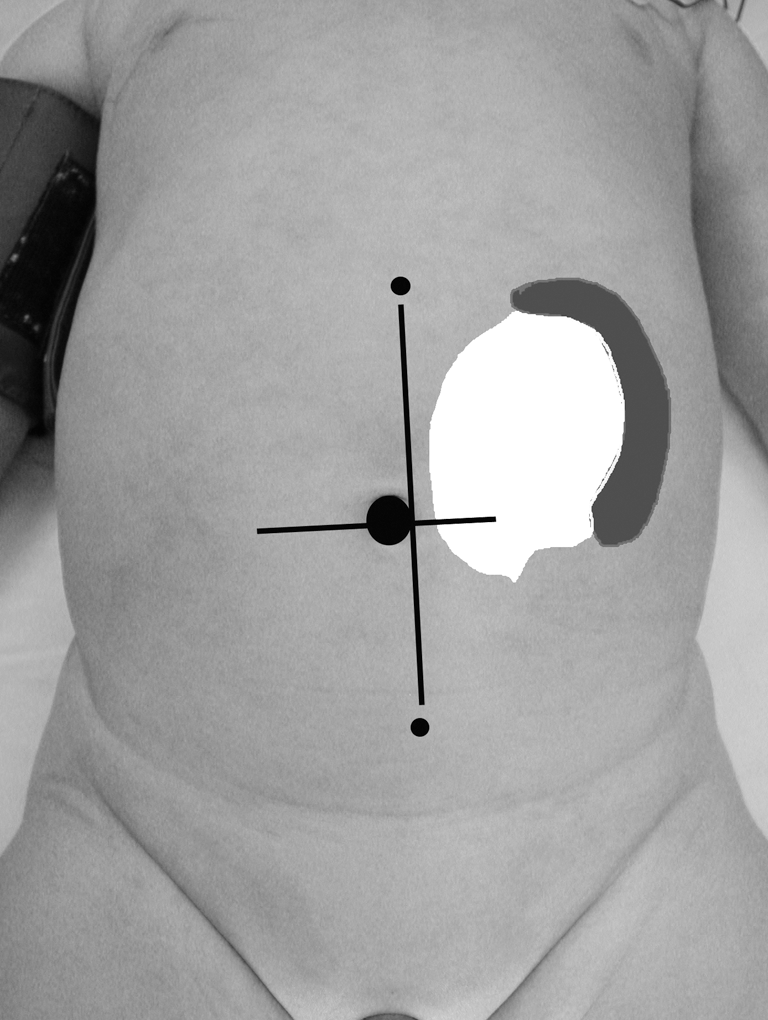
Illustration of port placement when the renal pelvis is larger and inferior, necessitating inferior and medial positioning of the inferior port. This can be placed in the midline, if necessary, or even on the opposite side unusually.
Exposure of UPJ
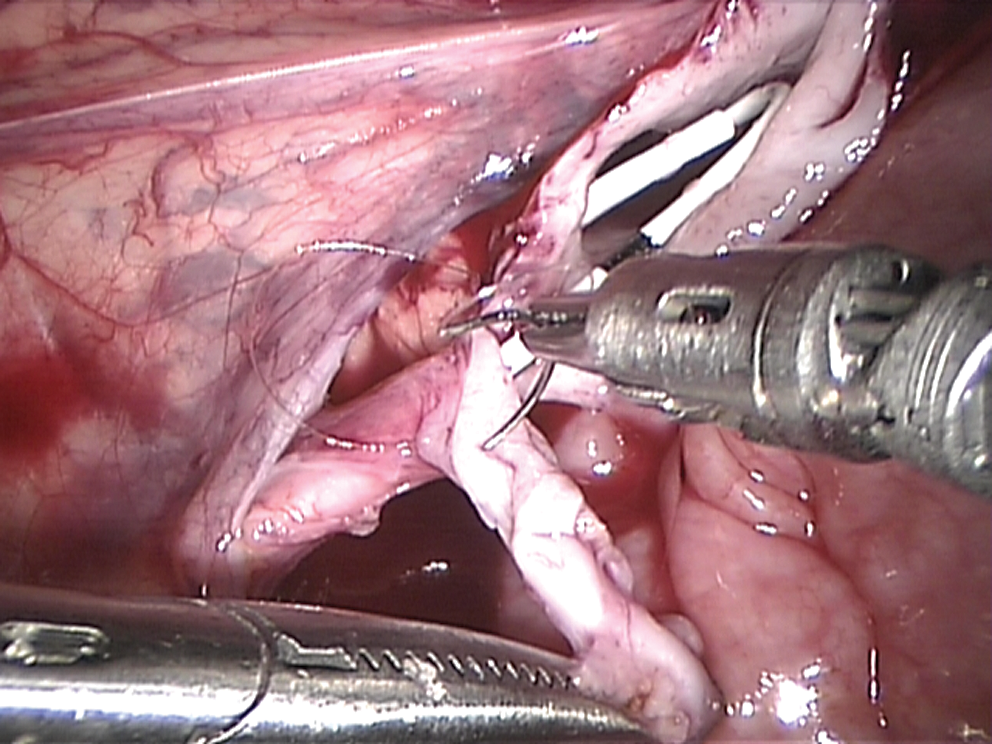
Exposure of the UPJ on the left is usually transmesenteric with a small incision in the mesenteric peritoneum near the inferior aspect of the pelvis. If this is not visible, the ureter may often be identified and traced superiorly to the UPJ, or the lower pole of the kidney is used to locate the UPJ. Blunt dissection around the ureter and pelvis permit lifting of the ureter, which will usually expose the UPJ as well. Continued blunt dissection of the loose adventitial tissue around the ureter is performed until it is free (Fig. 3). A careful search for any crossing vessels is performed. Any small vessels attached to the UPJ will need to be controlled with cautery and transected. Further blunt dissection of the pelvis is then performed to expose a sufficient amount for the repair. Only in the unusual case of a massively dilated pelvis is any significant amount of pelvic resection performed. The anticipated line of the pyelotomy is marked with cautery.
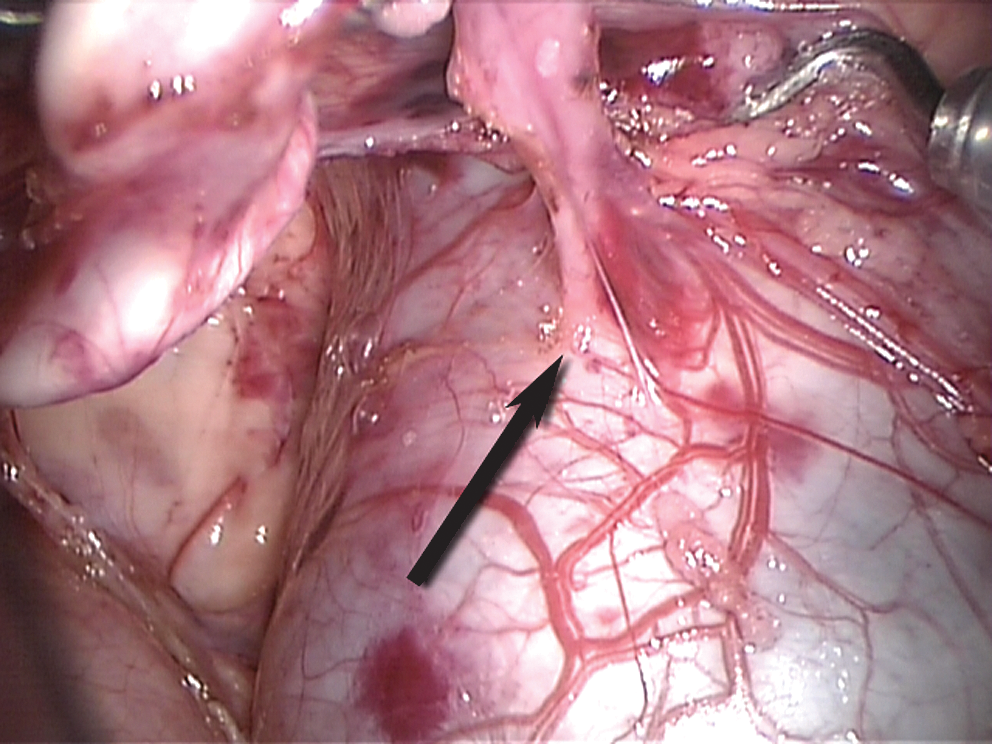
Operative image showing the stenotic right ureteropelvic junction (UPJ) after dissection (arrow). The preplaced stent is just below the UPJ narrowing and the renal pelvis remains distended.
Placement of hitch-stitch
To expose and stabilize the pelvis and UPJ, a hitch-stitch is placed in the renal pelvis. In most children, a 3-0 monofilament suture is passed on an SH needle through the abdominal wall lateral to the midclavicular line just below the costal margin. It is then grasped internally and passed through the pelvis just anterior to the medial edge. It is then passed back through the abdominal wall and tension adjusted to optimize exposure, and the two ends are clamped externally.
In a larger child with a thick abdominal wall, the hitch-stitch may be placed by tying a braided absorbable suture to the pelvis and then attaching this to the anterior abdominal wall. If two passes of the needle are taken in the abdominal wall, the suture will usually hold until it may be tied, as long as tension is not excessive.
Pyelotomy
The pelvis is incised with the scissors without cautery use in an oblique fashion from inferior lateral to superior medial. This should follow the line marked before placing the hitch-stitch, which will distort the anatomic orientation. One can always release the tension on the hitch-stitch if there is uncertainty about orientation. Usually urine will drain and may need to be aspirated. Suction is performed using a 5-mm laparoscopic suction device through one of the working ports.
Some have advocated leaving the ureter partially attached through the superior aspect of the incisions, but this can make manipulation more difficult. The author's preference is to leave the pelvic portion of the UPJ attached and use it as a handle while working with the ureter, thereby avoiding any touching of the anastomotic area.
Ureteral spatulation
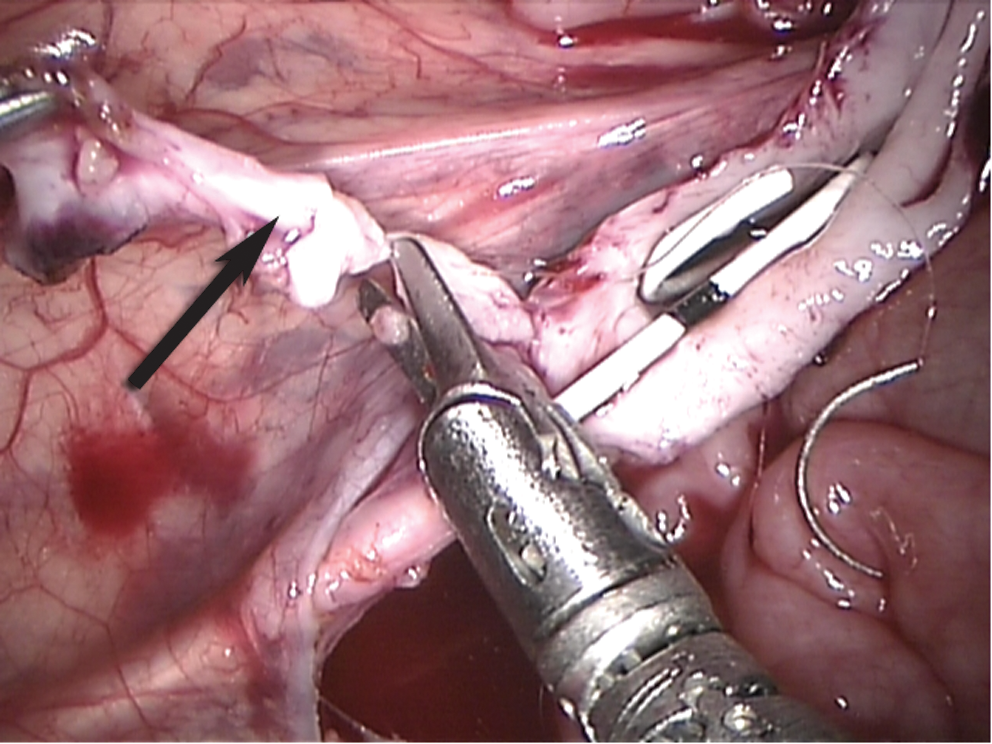
The ureter is spatulated on the lateral aspect to open the area of stenosis and provide a wide anastomotic line. Care is taken to avoid spiraling the cut. Generally, this is done through the narrowed UPJ, but may be carried out inferior to the UPJ completely (Fig. 4). The ureter should open widely and admit the closed scissors. No cautery is used. If a stent is in place, it can be used to guide the incision.
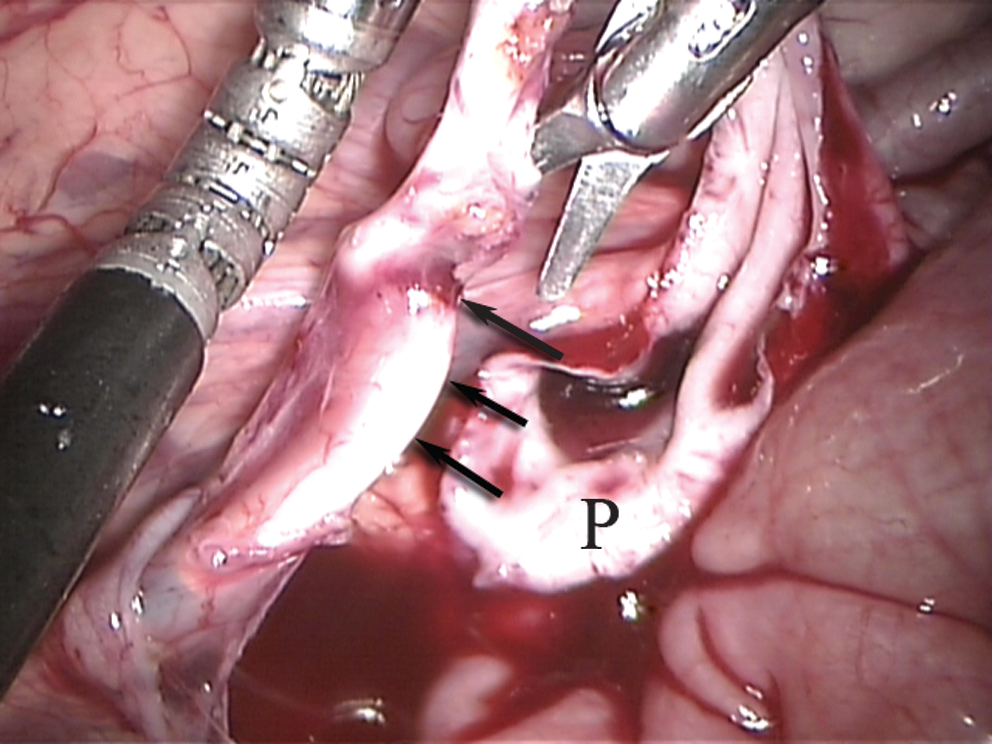
Spatulation of the lateral aspect of the proximal ureter as indicated by the arrows. The opened renal pelvis (P) is adjacent.
Back-wall anastomosis
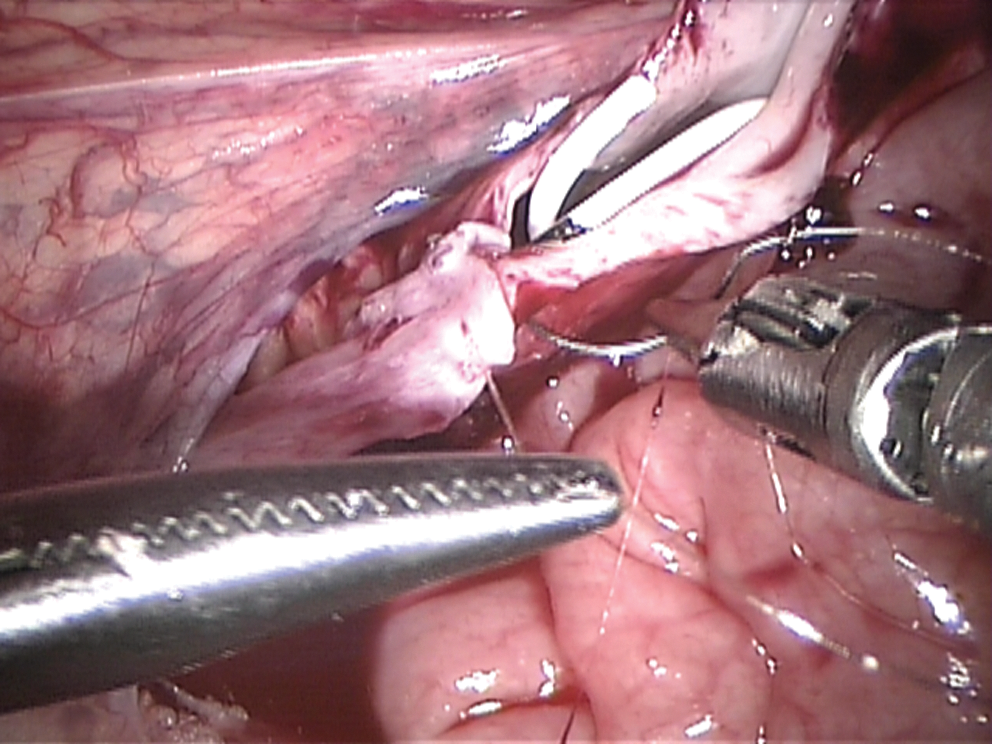
A running anastomosis with absorbable monofilament suture is performed by starting at the inferior apex of the spatulation (Fig. 5). If there is any tension, the ureter should be mobilized further. Interrupted sutures may be used for the initial stitches of the anastomosis, if desired. Generally, it is preferable to perform the back wall of the anastomosis first, although the orientation of the ureter and pelvis will determine the most efficient sequence. If a stent is in place, it can be used to expose the ureter and pelvis during the suturing. Care is taken to avoid touching any part of the anastomotic line with anything except the needle of the suture (Fig. 6). Once most of the back wall is completed, the redundant pelvis and UPJ are resected from the ureter to leave a widely pointed superior tip that will be the superior aspect of the pyeloureteral anastomosis (Fig. 7).

The initial anastomotic stitch at the apex of the spatulation (arrow) to the most dependent portion of the renal pelvis.
Suturing the back wall of the anastomosis with the stent placed in the renal pelvis. The renal pelvis still attached to the ureter is used as a handle to permit atraumatic manipulation of the ureter.
Removal of the redundant portion of the renal pelvis (arrow) just before completion of the back wall of the anastomosis.
Stent placement or positioning
If a stent has been preplaced, it is positioned into the renal pelvis at this point and advanced so that the proximal coil will hold itself in.
If a stent has not been placed, antegrade placement is now performed. For small stents (4.7F or less), a 16-gauge angiocatheter is passed through the anterior abdominal wall near the site of the hitch-stitch. With the stent preloaded, a guidewire is passed through the angiocatheter and guided into the proximal ureter by the operator. The wire is advanced several centimeters and followed by the stent. It should pass fairly smoothly. If not, a smaller guidewire or an angled wire may be used. The stent is passed through the angiocatheter and into the ureter. For larger stents, the angiocatheter is removed once the wire is passed down the ureter and with a small knick in the skin, the stent passed through the abdominal wall and guided into position.
Some prefer to have the bladder partially full of urine or urine with blue dye to confirm position, or have used intraoperative US to confirm stent position, 2 but we have found the usual estimates of stent length to be satisfactory (stent length is age +10 in cm). Confirmatory radiography may be performed.
Anterior anastomosis
After stent positioning, the anterior wall of the anastomosis is completed (Fig. 8). It has proven to be better to run the suture line from the apex of the spatulation superiorly in all cases to avoid a mismatch of the pelvis and ureter (Fig. 9). Some have suggested testing the anastomosis for leaks, but this seems unlikely to be necessary with a stent in place.
Completing the anterior wall anastomosis of the ureter to pelvis. The renal pelvis is still open and will now be closed.
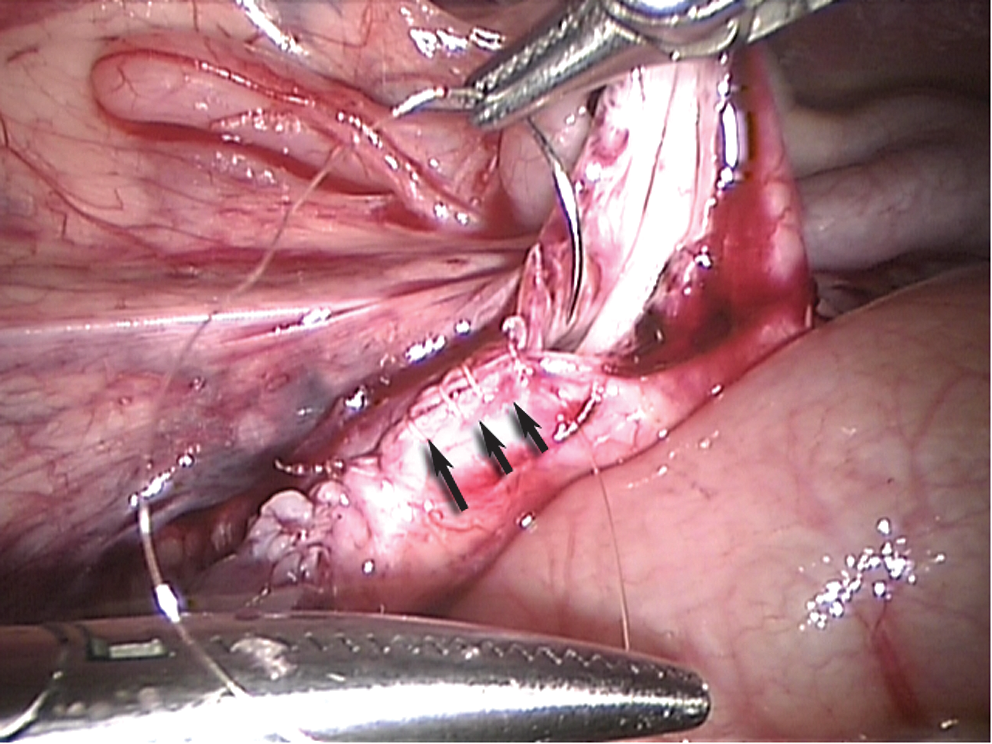
Closure of the pelvis superior to the ureteral anastomosis. The suture line is indicated by the arrows.
Closure
The hitch-stitch is cut and removed, any pooled urine or blood is aspirated, and the anastomosis inspected for bleeding or kinking. The retroperitoneum can be closed on the left, but this is not essential. An inspection of the field is made to ensure that there have been no inadvertent injuries to the bowels or liver on the right. The robot is disengaged, and the patient is turned to the flat position. Any fluid in the deep pelvis can be aspirated, and the ports are removed under vision with closure by way of the preplaced fascial box stitches. The pneumoperitoneum is evacuated through the umbilical port, and this site is closed and checked for a tight closure. Local anesthetic is instilled in each port site, and the subcutaneous tissues are closed with a 4-0 absorbable suture and the skin with a 5-0 subcuticular suture. Dry dressings are applied.
Retroperitoneal approach
Retroperitoneal pyeloplasty with the robotic system has been performed and reported with good results. 3 The author has used this rarely, and while it may be reasonable for older children, it is very difficult with the current system in younger children and does not offer a substantial advantage. In one case, an anterior crossing vessel was not identified as the cause of the obstruction leading to persisting postoperative obstruction and functional loss. Perhaps with a more flexible and smaller system, this method would become more efficient.
Postoperative Care
The bladder catheter is left in place overnight in most cases. If the child appears well, is eating and comfortable, and the parents prefer, discharge on the same day can be possible. Generally, patients will remain overnight until having oral intake, voiding, and comfortable with oral analgesics. This is very much age dependent.
If a stent with an extraction string is in place, the stent is removed in 2 weeks. Anticholinergics may occasionally be useful for comfort. If the stent is inadvertently dislodged prematurely, no effort is made to replace it unless symptoms should develop. If no extraction string is present, the stent is removed cystoscopically at 4 weeks postoperative. A follow-up US is obtained at 4 weeks after stent removal to ensure that the dilatation is no greater than preoperative. In cases in which intermittent obstruction was present with symptoms, the degree of hydronephrosis will often exceed the preoperative degree, but if no symptoms are present, no intervention is undertaken initially. Follow-up functional imaging using diuretic renography is usually reserved for 9 months postoperative, and this is performed to ensure adequate drainage and to assess the functional response to surgery. If the relative uptake of the kidney was less than 40% preoperatively, this is always obtained, even if there is clear improvement in hydronephrosis. For the asymptomatic child with relatively intact uptake and significant decompression after surgery, functional imaging is unlikely to be of benefit nor will it likely change management. Continued US is performed at progressive intervals, depending on the rapidity of improvement of the hydronephrosis. Reports have indicated that there is a low likelihood of problems if the initial diuretic renogram is within normal limits, but ongoing US follow-up appears more cautious.
Antibiotic prophylaxis is continued until the first US and if there is minimal dilatation, it is discontinued.
Management of Intraoperative Complications
The most significant intraoperative complications are those of laparoscopic access or inadvertent bowel injury during the procedure. 4 The key to such complications is prevention, followed by recognition. Prevention is best ensured by constant monitoring of all working instruments, particularly the cautery. The instruments should never leave the visual field, and the cautery should never be activated unless it is completely visualized. Blind cautery is exceedingly risky. Access complications are not unique to robotics or pyeloplasty and are discussed elsewhere.
If inadvertent bowel injury occurs, local cleaning, examination, and placement of an imbricating figure-of-eight stitch is generally appropriate. If there is any question as to bowel viability, a general surgical consultation is appropriate.
Vascular injuries are uncommon, because the procedure is not generally near the renal vasculature, but if bleeding develops, either lifting or compression is the best to control it and permit identification of the site. If cautery cannot stop the bleeding, a superficial suture ligature usually controls this. It should not be excessively deep to avoid injury to other structures.
Management of Postoperative Complications
Postoperative complications are unusual in robot-assisted pyeloplasty in children but are either acute or delayed. Acute issues include ileus or evidence of bowel injury. Ileus may be simply from manipulation and will resolve spontaneously in 1 to 3 days. One should always consider an occult bowel injury. This is classically manifest by ileus, port site pain, low-grade fever, and a depressed white blood cell count. If there is strong suspicion, a contrast CT is indicated, but free air in the abdomen can be expected for several days postoperatively. If a bowel injury is documented, laparoscopic or open exploration is appropriate, depending on the clinical scenario.
Urine leak is another early complication that may manifest as ileus with urinary ascites. Nearly always this may be predicted by the child not voiding after the catheter is removed and is the result of urine leak from the stent at the anastomosis. Replacement of the Foley catheter for 3 to 5 days will nearly always resolve the problem.
Late complications include persisting hydronephrosis because of stenosis of the anastomosis. It is not always clear why this would happen, and it is often that no explanation may be identified, but urine leak is not uncommonly associated. The diagnosis is not always simple, and it is often worthwhile placing a Double-J stent for 6 weeks if drainage is not satisfactory. This can stent open the repair enough to permit long-term drainage. In the worst case, reoperative pyeloplasty is necessary, and these are now being done robotically.
Results to Date
There are limited data as to pediatric robot-assisted pyeloplasty, and there are no formal prospective trials. At best one can say that the method is safe and effective with equivalence to open and laparoscopic pyeloplasty. It is certainly more readily learned than conventional laparoscopic pyeloplasty, which has few practitioners since it was described 15 years ago. 5 One report comparing with conventional laparoscopic pyeloplasty reported no advantage for robot-assisted surgery, but the learning curve must be considered. 6 A recent meta-analysis compared robot-assisted and conventional laparoscopic pyeloplasty and found them to be equivalent. This was in adults and children. 7 There are few practitioners using conventional methods to perform laparoscopic pyeloplasty in children, and the robotic approach has been used in children from 3 months to teen years. It is unclear at which age a clear advantage over open surgery is achieved, but the author does not believe that age discrimination is justified and any patient can be a candidate for robotic repair. Parental preference appears to favor robot-assisted pyeloplasty in one report, although the value of the small difference noted is undefined. 8 Table 1 shows the major reports of robot-assisted pyeloplasty in children.
RP = retroperitoneal; TP = transperitoneal; rob = robot-assisted; lap = laparoscopic.
Reoperative robot-assisted pyeloplasty is now beginning to be explored, and early reports are favorable. 9 This is a challenging procedure by any method, and the visualization and dexterity provided by the daVinci system are a valuable adjunct.
Conclusion
Robot-assisted pyeloplasty has emerged slowly as offering the advantages of conventional laparoscopy in terms of perioperative morbidity, but with a more rapid and efficient learning curve, with the potential for superior results based on the enhanced manipulation and visualization. While it is unclear how significant the advantages may be for infants, there is no simple cutoff age, and this common procedure has facilitated development of more complex renal and ureteral procedures for children using this new technology.
Footnotes
Acknowledgements
The contributions of Drs. Alan Retik as Chief of the Department of Urology and James Mandell, as CEO of Children's Hospital Boston in recognizing the potential and supporting robot-assisted surgery in children contributed significantly to the application of this new technology for children.
Disclosure Statement
No competing financial interests exist.