
Abstract
As a result of the widespread application of cross sectional imaging, there has been a significant rise in the incidence of small renal cortical neoplasms. The current standard of care in the management of these lesions is nephron-sparing extirpative surgery. In the last decade, however, image-guided or ablative therapies have garnered significant attention as nephron-sparing alternatives to partial nephrectomy. Although initially laparoscopic ablation was predominately intended for use as active treatment in those patients in whom more invasive therapy was contraindicated, as experience with laparoscopic ablation has become more robust, the indications for the procedure continue to evolve. The current article reviews the indications and contraindications, preoperative preparation, surgical technique, and postoperative follow-up for laparoscopic ablative procedures. Also discussed are techniques and patient selection criteria to avoid complications, as well as the management of complications that do occur.
Introduction
Indication and Contraindications
The dilemma facing urologists regarding the management of the small RCN is because of the uncertainty of an individual tumor's natural history. Historically, the majority of RCNs that were identified were quite large and were symptomatic, and these tumors were removed at the time of initial diagnosis. As such, there was limited knowledge regarding the natural growth or metastatic potential of RCN. Recently, larger active surveillance (AS) series with medium-term follow-up have contributed new information suggesting that most small renal masses (SRMs) have an indolent course, including a slow growth rate and low risk of progression to metastatic disease. In addition, several series have demonstrated that an accelerated RCN growth rate correlates with malignancy. 5 –10
Extripative therapy for small RCN, although remaining the standard of care, continues to be associated with significant morbidity. As such, not all patients are candidates for this form of surgery. Ablative therapies are generally less invasive and are therefore an attractive alternative to some extirpative procedures. Desai and colleagues 11 demonstrated that laparoscopic cryoablation (LCA) has reduced blood loss and complication rates when compared with laparoscopic partial nephrectomy (LPN). Initially, the indications for ablation included elderly patients, patients at high surgical risk, and those who refused extirpation. The availability of intermediate-term and refinement of ablation patient selection and technique data, however, have expanded the indications for ablative therapies as a viable alternative for many patients with small RCN.
Ablative therapies are generally contraindicated in patients with renal masses >4 cm in diameter. Lehman and associates 12 compared results for LCA for small (<3.0 cm) vs large (≥3.0 cm) tumors. The complication rates (0% vs 62%, P = 0.0007) and length of hospitalization (1.65 vs 3.52, P = 0.02) were significantly different for small and large RCN, respectively. In addition, while not statistically significant, the difference in blood loss for small and large tumors was clinically relevant (78 mL vs 398 mL, respectively, P = 0.13). Exophytic tumors had a higher blood loss (103 mL) than either mesophytic (62.5 mL) or endophytic (53 mL) lesions. 12
While overly general in their recommendations, the AUA guidelines separate patients into four categories and therapies into three levels of management strategies. 4 The most strongly suggested management strategy is a “standard,” while a “recommendation” and an “option” have successively decreasing support from the AUA. Patient stratification in these recommendations includes clinical T1a patients of good and poor health (index patients 1 and 2, respectively) and T1b patients of good and poor health (index patients 3 and 4, respectively). For the T1a patient in good health (index patient 1), the AUA suggested that standard of care is PN by an open approach (laparoscopic for simple cases) with radical nephrectomy (RN) an alternate standard. In this population, both thermal ablation and AS are listed as only treatment options. As it pertains to ablation, the panel expressed concerns about higher local recurrence rates, variability in the definition of success in the available literature, and the likelihood of a difficult surgical salvage. For index patient 2, the AUA suggested standard of care remains surgical extirpation by way of PN or RN, but thermal ablation and AS are upgraded to AUA recommendations for this group because of the advantages of the minimally invasive approach.
For index patient 3, RN is the suggested standard of care with PN an alternate standard. In this group, both AS and thermal ablation are listed as “suboptimal” options, receiving the least amount of support by the panel when compared with other patient categories. Surgical extirpation is emphasized in this group because of the high complication and local recurrence rates associated with ablating large tumors, and the high risk of disease progression during AS in an otherwise healthy population. Finally, the AUA maintained that for index patient 4, RN is the standard of care, and PN falls to the level of an AUA recommendation because of the high-risk nature of the surgery in this population. AS is suggested as an alternate recommendation for those patients who may not tolerate or wish to avoid surgery. Thermal ablation persists as an option, but the panel once again cited concerns about high complication and recurrence rates. 4
While recognizing the intent with which the guidelines were constructed, the authors opine somewhat differently than the panel as it pertains to the ablative therapies. First, in healthy patients with small tumors (index patient 1), the complication and re-treatment rates are sufficiently low that thermal ablation can be offered as a primary treatment modality. This is particularly true in light of the feasibility of repeated procedure salvage of failures. In addition, in T1a patients with a comorbidity index of at least 3, AS should be considered a primary treatment with thermal ablation a salvage therapy should it fail. Finally, because of the higher complication rate and poor efficacy of thermal ablation in large lesions, the ablative therapies should not be offered to patients with T1b tumors (index patients 3 and 4), regardless of health status.
Percutaneous thermal ablation has recently gained popularity as an adjunct in the management of the SRM. The primary indication for choosing a percutaneous approach in lieu of a laparoscopic approach is tumor location. Posteriorly located tumors are ideally situated for a CT-guided percutaneous approach, while anterior tumors are more amenable to a transperitoneal approach. The overwhelming majority of published RFA series describe a percutaneous approach while most contemporary cryoablations are performed laparoscopically. As such, RFA will be briefly mentioned, but the focus will be on laparoscopic cryoablation.
Preoperative Workup and Patient Preparation
All patients with a renal mass should undergo a standard evaluation, including a complete history and physical, standard preoperative laboratory studies, electrocardiography, chest radiography, and either an MRI or CT scan of the abdomen and pelvis with and without intravenous contrast. 4 If there are any neurologic findings during physical examination, a head CT or MRI to look for brain metastases should also be considered. An elevated serum alkaline phosphatase level, serum calcium level, or a complaint of bone pain should prompt the surgeon to perform a bone scan to rule out bone metastasis. All medications with anticoagulation or antiplatelet activity are stopped 7 to 10 days before surgery.
High-quality, recent axial abdominal imaging is necessary to characterize the renal mass. The size (maximal diameter in cm), location (upper, lower vs interpolar, exophytic, mesophytic vs endophytic), and quality (cystic vs solid) of the mass should be documented as well as the enhancement (Hounsfield units) after contrast administration. The course of the ureter should be identified and avoided during all ablation procedures. All risks and benefits of the ablation procedure should be discussed with the patient. Similarly, all appropriate consents (including transfusion consent) should be obtained preoperatively.
Instrumentation
The instrumentation discussed will focus on the author's preferences in terms of surgical technique and instrumentation. In the early going, a representative from the company providing the ablation technology can be helpful to coordinate an inservice presentation directed toward all members of the surgical team. During these preparations, the team is introduced to proper use of the ablation equipment and the instruments that will be used (Table 1). It is useful to have a company representative and even an experienced surgeon to act as a proctor, present during the surgeon's initial experience.
Principles of Cryoablation
Optimal ablation results are achieved by understanding the mechanism by which ablation modalities result in cell death. For cryoablation technologies, a combination of processes, including intracellular crystal formation and microcirculatory failure, leads to irreversible cellular injury and subsequent death. Rapid cooling produces an increase in extracellular osmotic force, resulting in intracellular fluid egression and sudden dehydration. Mechanical disruption of the cell membrane along with changes in pH leads to protein denaturization. 13 Microvascular injury leads to circulatory failure with the end result of widespread thrombosis, coagulation necrosis, and apoptosis over the course of hours to days.
Contemporary cryosurgical systems exploit the Joule-Thomson principle to quickly decrease temperatures within the renal tissue. Highly pressurized argon in the liquid state is allowed to expand through a restricted orifice into a gaseous state. The phase change induces rapid cooling and iceball formation. While the core temperatures at the tip of the cryoprobe reach −140°C to −190°C, temperatures increase along a gradient to 0°C at the edge of the visible iceball. 14 This is important because to be consistently tumoricidal, tissue temperatures must fall to −40°C. 15 Temperatures of less than −20°C are reached 3.1 mm from the edge of the iceball. 16 Therefore, the goal is to extend the iceball 1 cm beyond the tumor edge to ensure complete ablation. The cycle is completed with an active thaw phase that uses either helium gas or radiofrequency to heat the cryoprobe.
Surgical Steps
Step 1. Patient positioning
On induction with a general anesthetic, an orogastric or nasogastric tube and Foley catheter are placed. The patient is then placed in a modified lateral decubitus position and bony prominences are carefully padded; an axillary roll is appropriately positioned outside of the axilla. The bed is flexed to allow for adequate kidney exposure, and the patient is secured to the table with wide silk surgical tape and towels across the chest and hips (Fig. 1).

Patient positioning.
Step 2. Pneumoperitoneum and trocar placement
Classically, laparoscopic cryoablation is typically performed transperitoneally for anterior, lateral, and hilar renal masses and retroperitoneally for posterior tumors. Currently, however, posteriorly located tumors are treated percutaneously at our institution.
During the laparoscopic transperitoneal approach, a Veress needle or Hassan access is achieved in the ipsilateral lower quadrant, and pneumoperitoneum established. A nonbladed (dilating) 12-mm trocar is advanced into the distended peritoneal cavity under direct visualization. Before proceeding, the abdomen is surveyed with particular attention to the bowel and vasculature directly below trocar access points to identify occult injuries. A total of three 12-mm trocars are placed in such a manner as to triangulate the kidney mass (Fig. 2). For right-sided tumors, a midline 5-mm trocar is placed just inferior to the xyphoid process. A locking laparoscopic grasper is passed through this trocar to elevate the liver.
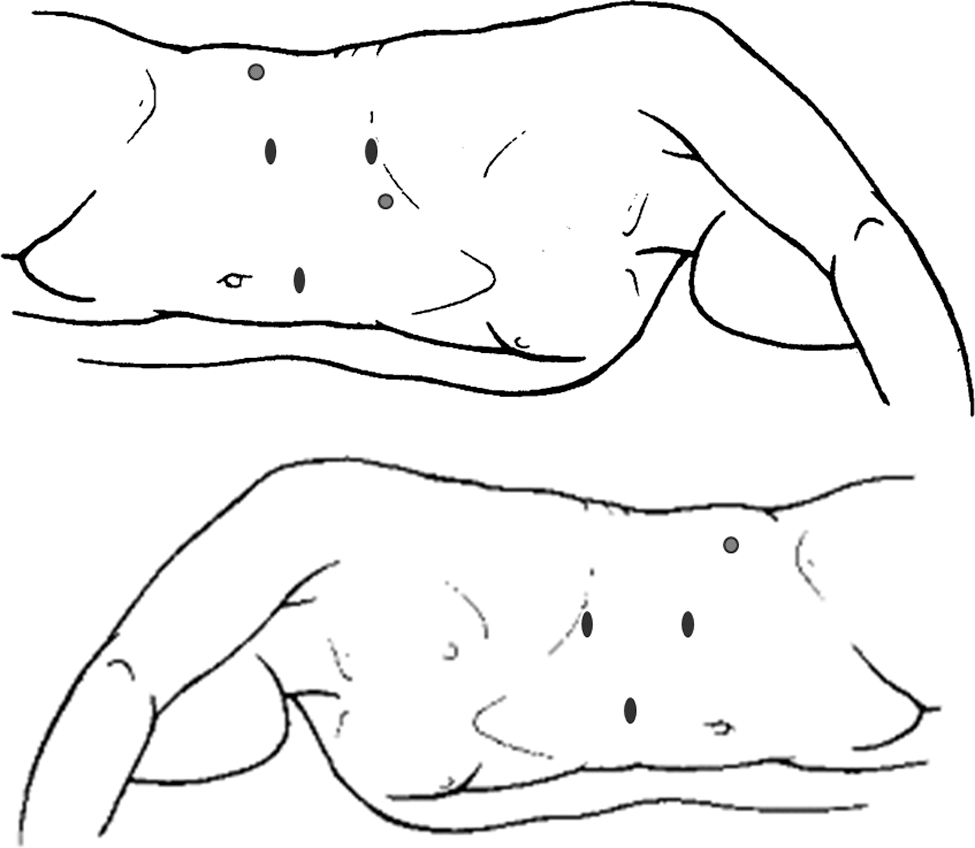
Left- and right-sided transperitoneal trocar sites. Ovals represent 12-mm trocar sites, and circles represent 5-mm retraction sites.
The addition of a 5-mm trocar just anterior to the midaxillary line allows for the placement of a laparoscopic retractor (Jarit® Padron Endoscopic Exposing Retractor (P.E.E.R.), Integra, Plainsboro, NJ), which is secured using a laparoscopic Endoholder (Bookwalter Endoscopic Instrument, Codman, Raynham, MA). While optional, the use of a laparoscopic retractor frees the surgeon's hands facilitating a two-handed approach to the dissection and thus improving the safety of the procedure.
Step 3. Renal mass and hilar exposure
The ascending or descending colon is identified and mobilized along the white line of Toldt before being reflected medially. The kidney's superior attachments (splenorenal ligament on the left and the triangular and anterior coronal on the right) are completely released. On the right, the duodenum is kocherized. Next, the kidney is elevated by creating a posterior plane between the psoas muscle and the Gerota fascia. The ureter and gonadal vein are identified, and the dissection is carried cephalad until the hilum is encountered. In left-sided procedures, the gonadal vein is dissected and tracked cephalad, which leads to the renal vein. For right-sided procedures, the lateral border of the inferior vena cava is followed cephalad to the right renal vein. In the majority of cases, the renal vasculature does not need to be identified and dissected. For challenging cases where there is concern for bleeding or with very hilar tumors, the renal hilum is completely dissected for emergency access. Next, the renal mass is targeted using a combination of preoperative imaging and the intraoperative US. The Gerota fascia is entered, and the perinephric fat is mobilized away from the mass to allow for direct visualization during cryoprobe insertion and iceball formation. In addition, adequate space must be provided for resection and reconstruction of the renal defect if PN is warranted.
Step 4. Renal mass biopsy
We use a small caliber needle (BD™ Spinal Needle, BD Medical, Franklin Lakes, NJ) as a “finder” needle. The finder needle is used to assess multiple cutaneous access sites in an effort to establish the optimal position and direction for biopsy and ablation needle deployment. The optimal needle path is a perpendicular path from the skin surface to the tumor. This is an important step that may take several attempts to determine a perfect needle trajectory. Once an appropriate path is identified, a small skin incision is made adjacent to the finder needle, and several percutaneous core biopsies are taken from the mass under direct visualization using a biopty gun (Bard® MaxCore Disposable Core Biopsy Instrument, 18 G × 25 cm, Bard Peripheral Vascular, Inc/Bard Biopsy Systems, Tempe, AZ). If the mass is cystic, the biopsy should not be performed because of low probability of obtaining an adequate specimen and the theoretical risk of tumor dissemination. In addition, cyst decompression makes precise targeting more challenging.
The surgeon must ensure that perpendicular (not tangential) probe placement is performed. Acute-angle placement of the cryoprobes generates an oblique iceball, which is more difficult to precisely target and which may lead to an incomplete ablation and residual tumor.
Step 5. Probe placement and ablation
Ideal probe placement depends largely on tumor size, shape, location, and whether the tumor is cystic or solid. For solid tumors, the probes are advanced under direct vision just within the confines of the mass. The cryoprobe tips are advanced just beyond the deepest portion of the tumor. Accurate depth is assessed by intraoperative US. For predominantly cystic lesions, we deploy the cryoprobes bordering the outer surface of the tumor so as to avoid cyst puncture and subsequent spillage of tumor cells. The probes should extend beyond the deep margin of the tumor because the tumoricidal zone does not extend appreciably beyond the tip. Intraoperative US evaluation of the expanding iceball demonstrates shadowing from the US reflection, creating a blind spot (Fig. 3). This makes confirmation of the iceball depth unreliable and emphasizes the necessity for correct probe placement from the outset, as well as multiple angles of US ultrasound assessment to confirm complete ablation of the target lesion.
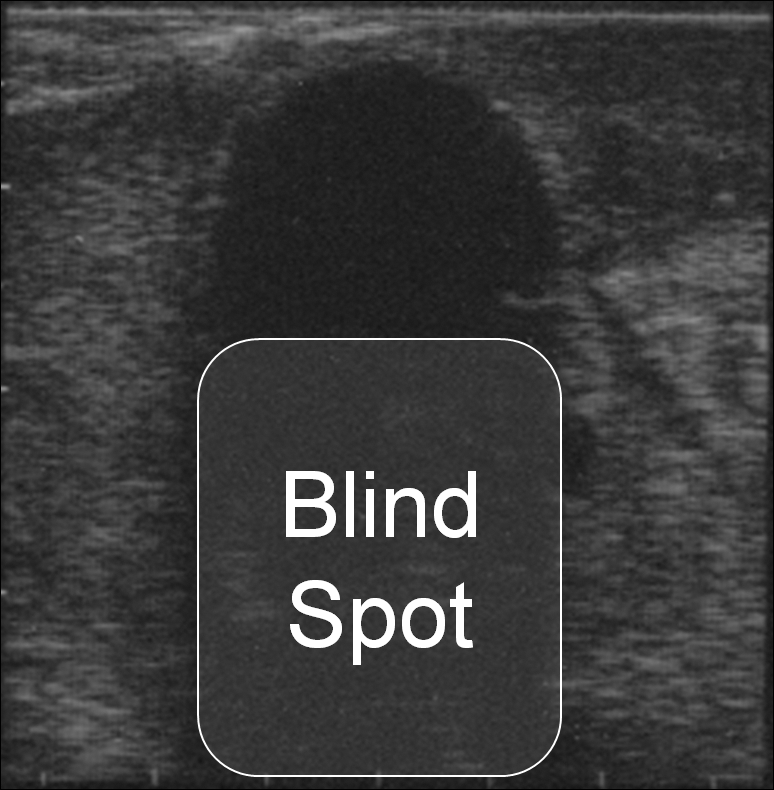
Blind spot created by the expanding iceball.
The first freeze cycle is performed until the iceball extends to 1 cm beyond the mass as determined by intraoperative US. This is followed by either an active or passive thaw phase. A second freeze-thaw cycle is then repeated to ensure adequate lesion ablation. The second iceball usually extends past the initial border of ablation, which gives the surgeon confidence that the tumor has been fully ablated. After a second thaw cycle, the cryoprobes can be removed, but this must be done gently to minimize the risk of tumor cracking and bleeding with traumatic probe extraction. When the probes can be twisted within the ablated parenchyma without resistance, they may be removed. The ablation zone should be monitored for subsequent hemorrhage, and hemostatics such as FloSeal®, and Surgicel® are used combined with gentle pressure to control bleeding.
Management of Intraoperative Complications
Complications from cryoablation are rare with bleeding from iceball fracture being the most common. In the vast majority of cases, intraoperative bleeding is usually easily controlled with hemostatic agents and direct pressure. When bleeding cannot be controlled in this manner, we most typically perform a LPN. Advanced exposure of the hilum is important in cases where the surgeon suspects iceball fracture is likely.
Iceball involvement of the intrarenal collecting system generally does not lead to a urine leak. 17 –20 The ureter and renal pelvis should not be involved in the ablation, however, because it may lead to stricture formation.
Postoperative Complications
Excessive flank discomfort, prolonged ileus, and a decrease in hemoglobin level postoperatively are indications of postoperative hemorrhage. A CT scan of the abdomen and pelvis without contrast will identify a hematoma and thereby be diagnostic. In the event of postoperative hemorrhage, conservative measures usually suffice. Patients remain on bed rest and are monitored with scheduled blood counts. Blood transfusion is rarely necessary.
Focal pain over a specific trocar site, low-grade fever, and leukopenia warrant prompt evaluation with a CT scan of the abdomen and pelvis with oral contrast to rule out bowel injury.
Postoperative Care
The patient is admitted for overnight observation. A blood count and basic metabolic panel should be performed in the recovery room and again on the morning of postoperative day 1. Follow-up includes an office visit 6 weeks after surgery to evaluate the patient's clinical symptoms and surgical incisions. At 3 months postoperatively, a CT or MRI of the abdomen and pelvis with and without a contrast is performed to identify residual disease. If there is no enhancement in the ablation zone, viable tumor likely does not exist, and the patient is considered to be free of disease. 21 Follow-up then consists of annual cross-sectional imaging and physical examination.
In the event of residual disease or recurrence, re-treatment depends largely on final pathology results, renal function, and patient preference. Active surveillance, repeated ablation, or PN may be performed.
Summary of Cryoablation Literature
The body of work on laparoscopic ablation has grown considerably since its inception. The AUA guideline panel reviewed all published series on cryoablation and performed a meta-analysis. 4 The mean patient age was 66.9 years, mean tumor size 2.6 cm, with a mean follow-up of 19.5 months. The rate of major urologic complications (hemorrhage necessitating transfusion, urinary leak, abscess, loss of renal function) was 4.9% while the reintervention rate was 2.6%. At a mean of 26.2 months, the recurrence-free survival (RFS) rate was 87.6%. This calculation of RFS is likely an underestimate, because the panel did exclude a number of series and did not take secondary ablation procedures into consideration.
In a more recent study that examined long-term outcomes after LCA, Aron and coworkers 22 reported on 80 patients with a minimum follow-up of 5 years (range 5–11, median 8 years). Mean tumor size was 2.3 cm with 80% treated with a single 4.8-mm cryoprobe. The perioperative complication rate was low (10%) and included only one retroperitoneal hematoma necessitating transfusion. Among the 55 patients with pathologically confirmed malignancy, there were 11 (14%) recurrences and 6 (7%) cancer-related deaths, resulting in a 5-year overall, disease-specific and disease-free survival of 84%, 92%, and 81%, respectively. Ten-year overall, disease-specific and RFS were 51%, 83%, and 78%, respectively. Interestingly, the only significant risk factor predicting RFS and disease-specific survival on univariate and multivariate analysis was previous radical nephrectomy for renal-cell carcinoma (RCC) (P = 0.019 and 0.008, respectively). 22 Table 2 contains a selected list of recommended publications along with a brief summary for review.
Represents 1 patient with remote recurrence.
Represents 3 patients with recurrence in the tumor bed alone, 2 with new lesions in the treated kidney, 1 with tumor bed recurrence and a distant metastasis, 1 with a new lesion in the treated kidney and distant metastases, and 4 with distant metastases alone.
Represents 2 patients with recurrence in the tumor bed and 3 with remote recurrence.
Cancer specific survival reflects only those patients with >5-year follow-up.
Alternative Ablative Therapies
RFA
RFA is an ablative technique whereby high-frequency electrical current is transferred into the ablation zone. Coagulative necrosis, fibrosis, and vascular thrombosis result as temperatures rapidly rise to more than 60°C. 13 Similar to cryoablation, extending the ablation zone 1 cm beyond the mass is recommended to maximize efficacy. Unlike LCA, real-time ablation is inferred from strategically placed temperature or impedance probes and cannot be immediately visualized with US. 13 This can create inaccuracies because of either charring near the detection probe or a discrepancy between probe readings and actual nearby tissue temperatures. While RFA can be performed open, laparoscopically, or percutaneously, the overwhelming majority of cases are performed percutaneously.
Currently, there are no publications that demonstrate long-term (>10 year) outcomes; however, intermediate-term outcomes are promising. Tracy and colleagues 23 recently published their experience of 243 SRMs with a mean follow-up of 7.5 years. Seven patients had an incomplete primary ablation (97% initial success rate), and there were nine local recurrences, all of which occurred at ≤3 years follow-up. In the subset of patients with pathologically proven RCC, both the 3- and 5-year RFS was 90%, and the 3- and 5-year cancer-specific survival was 99%. The complication rate for RFA is between 2.8% and 17.6%, with the major complications being ureteral obstruction, collecting system injury, and bowel injury. 24
HIFU
HIFU is an extracorporeal ablative technique that is still in its infancy. In HIFU, the tumor is first identified using conventional US. A piezoelectric generator then adjusts the power, duration, and location of the ultrasound waves, which pass through the tissues and are converted to thermal energy within the target zone. Currently, there is no method to monitor the ablation in real time, and the published data on HIFU are very limited. 25 Complications of treatment are mostly local, including skin burns and discomfort at the treatment site. 26,27 Klingler and associates 28 performed laparoscopic HIFU, and although adequate ablation was demonstrated in the majority of patients, 30% of the lesions (3/10 tumors) had evidence of residual disease. Overall, HIFU is still considered investigational and should not be offered to patients outside of clinical trials.
Disclosure Statement
No competing financial interests exist.
Footnotes
Abbreviations Used
*
A coordinating article with video is available in Videourology 25/1 at