
Abstract
Background and Purpose:
Photoselective vaporization of the prostate (PVP) has emerged as an effective debulking procedure for prostatic urinary obstruction. Surgical technique for the most efficient vaporization has, however, received little scientific investigation. We used an ex-vivo bovine prostate model to investigate how variation in the angle of laser fiber rotational movement (“sweeping”) affects prostate tissue vaporization efficiency.
Materials and Methods:
Experiments were conducted using the GreenLight™ HPS 120W laser system. A single surgeon performed a clinical PVP video analysis, forming the basis of our study design. Sixty bovine prostate specimens were vaporized using an ex-vivo chamber equipped with computer-assisted axial movements. Specimens were vaporized at a fixed sweeping speed (0.5 sweeps/sec) and variable sweeping angles (0, 15, 30, 60, 90, and 120 degrees). The volume of tissue vaporized was calculated from cross sections and compared by a two-sample t test.
Results:
Clinical PVP video analysis of a single experienced surgeon showed a mean angle of 47.7 degrees with 25% of vaporization between 0 and 30 degrees. Ex-vivo analysis showed larger sweeping angles generated wider but more superficial vaporization defects, leading to smaller vaporized volumes. Specifically, vaporization volumes with angles of 0, 15, or 30 degrees were significantly greater than those with rotational angles of 45, 60, and 90 degrees (1.5-3.0 X; P<0.05). The depth of tissue coagulation significantly increased with greater rotational angles.
Conclusions:
Optimal PVP occurred at narrower angles of laser fiber sweeping in our ex-vivo model. Our findings highlight that PVP laser fiber movement can be tested in a scientific manner, identifying parameters to maximize vaporization efficiency.
Introduction
Among laser modalities, PVP offers the theoretical advantage of using a characteristic 532-nm wavelength laser that is selectively absorbed by hemoglobin within prostatic tissue. 8,9 This wavelength is achieved by specific crystals (either potassium-titanyl-phosphate [KTP] or lithium triborate [LBO]), which halve the 1064-mm wavelength of pulsed neodymium:yttrium-aluminum-garnet laser light to create the desired 532-nm wavelength. The result is selective vaporization of prostatic tissue with effective hemostasis and relatively little tissue coagulation (1.5±0.3 mm margin), as demonstrated in preclinical models. 10 Clinically, PVP has been shown to have an improved side-effect profile, time of catheterization, hospital stay, and improvement in urinary flow rate. 7,11 –15 PVP is also efficacious in high-risk patients, such as those with large prostates or receiving anticoagulant medication, 16 –23 and has long-term durability. 24 Accordingly, PVP has been shown to have a significant cost advantage over traditional TURP. 25
A primary limitation of PVP, however, has been less efficient tissue removal relative to traditional TURP. The next generation of PVP laser systems has aimed to improve vaporization efficiency, including the GreenLight™ High Powered System (HPS) that uses a LBO crystal to achieve a power of up to 120W compared with the 60W or 80W power of KTP-crystal predecessors. This change, coupled with a smaller beam divergence for higher power density, has allowed more effective prostate vaporization in cadaveric bovine and living canine animal models without an increase in coagulative tissue effects or long-term fibrosis. 26 Clinically, initial studies support the new HPS technology as safe and effective. 27,28
Currently, there are few specific surgical recommendations for achieving optimal tissue vaporization efficiency. 2,29 Common to virtually all described laser approaches is the rotational side-to-side movement of a laser fiber along the prostatic tissue often referred to as “sweeping,” distinct from the axial movement during traditional TURP. Despite its virtually universal acceptance, the laser fiber sweeping technique has received little scientific investigation or validation. We recently reported that the speed of laser fiber sweeping could affect tissue vaporization efficiency during PVP with the Greenlight HPS 120W laser. 30 Specifically, using a novel ex-vivo bovine model, we showed that slower sweeping speeds (≤1.0 sweep/sec) removed up to twice as much tissue as faster speeds (1.5–2.0 sweeps/sec), with significant, albeit minimal reductions in coagulation margins. These results suggested that vaporization efficiency might be compromised with faster laser fiber sweeping speeds, countering basic principles of traditional TURP in which faster axial movement toward the surgeon removes tissue more efficiently. While the clinical translation of these findings is uncertain, the study underscored that PVP technique can be tested in a scientific manner for identification of optimal parameters for tissue vaporization.
Another important parameter of laser fiber sweeping is the angle of rotational movement. Gomez and associates 29 in 2007 published recommendations for a suggested 60-degree arc of rotation as the ideal sweeping motion. With greater rotation, the authors propose that an increased distance from fiber to tissue occurs, causing coagulation, not vaporization. To our knowledge, however, scientific validation of this standard has not been attempted. 29 Here, we follow up our previous study on sweeping speed with a novel investigation testing the hypothesis that variation in the angle of sweeping alters PVP vaporization efficiency. To do so, we again use the Greenlight HPS 120W system and a similar ex vivo bovine prostate model. 30 Our aim again is to elucidate principles for PVP technique that may aid urologists in maximizing tissue vaporization efficiency.
Materials and Methods
Clinical PVP and video analysis
To identify rotational angles used in clinical PVP, video analysis was performed on a 34-minute clinical PVP session conducted by a urologist who was experienced with the technique. Ten minutes of clinical footage were randomly selected for analysis. All video analysis was performed using a frame grabber program by GOP media, which digitized each analog video to acquire frame-by-frame images at a rate of 100 ms. The fiber tip showed a blue arrow on the surface, which was indicative of the opposite side of laser firing. During the procedure, the arrow moved circumferentially because of the angular motion of a fiber tip, and the angle between two frames was calculated using mathematical modeling (Fig. 1).
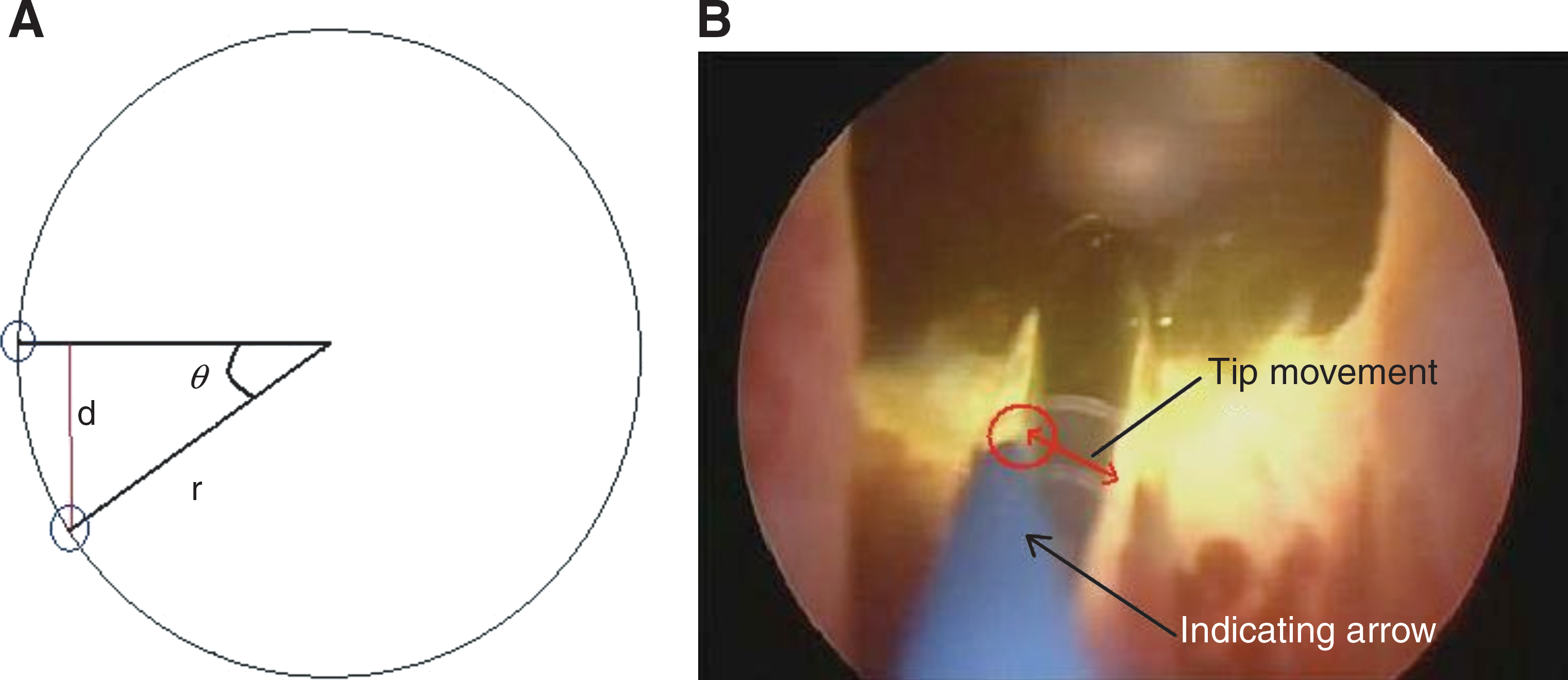
Representation of laser fiber sweeping angles.
Bovine prostate tissues
PVP experiments were performed using cadaveric bovine prostate tissue. The use of the cadaveric bovine prostate model for this purpose is previously described. 31,32 Freshly frozen bovine lower urinary tracts (bladder, prostate, urethra) were obtained from a local slaughterhouse and stored for up to 4 hours in 4°C saline before experimental PVP. Prostate tissue was dissected out of the urinary tract, and sections of 2.5×2.5 cm were excised for use in the ex vivo chamber, as described below.
Laser system and PVP experimental design
The GreenLight HPS laser system equipped with a 70-degree side-firing, 600-μm laser fiber was used for all experiments. Tissue vaporization was performed at this system's customary power of 120W by a urologic surgeon who was experienced with clinical PVP. Ex-vivo PVP was performed on a total of 60 2.5-cm×2.5-cm cut prostatic specimens using a custom-made two-dimensional laser scanning system, as previously described and detailed in Figure 2. 30,31 Specimens were fixed in position with epithelial side up in a metal tissue holder with a screw-tight top plate containing a 1.5-cm×1.5-cm aperture, which flattened the tissue surface while exposing a window for vaporization. The tissue holder was submerged under continuous-flow 20°C saline to remove tissue debris and cool the fiber. Computer-assisted motors enabled relative movement of the laser fiber tip along the tissue surface (x-axis) at a fixed speed of 1 mm/s for a 15-mm stretch while maintaining a fixed 1-mm working distance (z-axis).

Prostate tissue vaporization apparatus.
Experimental PVP was performed using side-to-side sweeping angles (y-axis) of 0, 15, 30, 60, 90, and 120 degrees by visual monitoring of a protractor attached to the laser fiber. A constant sweeping speed was maintained by manual synchronization with an audible metronome at 0.5 sweeps/sec based on our previous finding of optimal PVP vaporization at this speed in this ex-vivo bovine model. 32
Measurement of vaporization efficiency and coagulation
Vaporization efficiency was assessed by measurement of tissue cavity volume created during PVP by histologic cross-sectioning, as previously described. 30 Briefly, vaporized tissues were cut into ten 1-mm histologic cross sections. The area of each cross-sectional cavity was quantified using the Image-J software program (National Institutes of Health, Bethesda, MD) and multiplied by 1 mm to give the vaporized volume for the cross section. Vaporized volume for the whole specimen was calculated as the sum of the 10 cross-section volumes. Coagulative margins were similarly determined using cross sections of tissues by measuring the depth of necrotic rim at five specific points (3, 5, 6, 7, and 9 o'clock) along the vaporized cavity of each specimen. 31 Our previous study showed that this coagulation margin measured from gross cross sections correlates with microscopic histology. 31
Results
Clinical video analysis of PVP performed by a single experienced urologic surgeon demonstrated a mean sweeping angle of 47.7 degrees±19.6 degrees and a range from 0 to 120 degrees. As depicted in Figure 3, the vast majority of analyzed operative time was spent using sweeping angles in the range of 20 to 80 degrees. Angles less than and greater than this range were used only 7% and 3% of the time, respectively. The most common angles were 20 to 30 degrees and 60 to 70 degrees, together representing one third of the analyzed operative time. Sweeping angles >30 degrees were used during 75% of the analyzed case (Fig. 3).
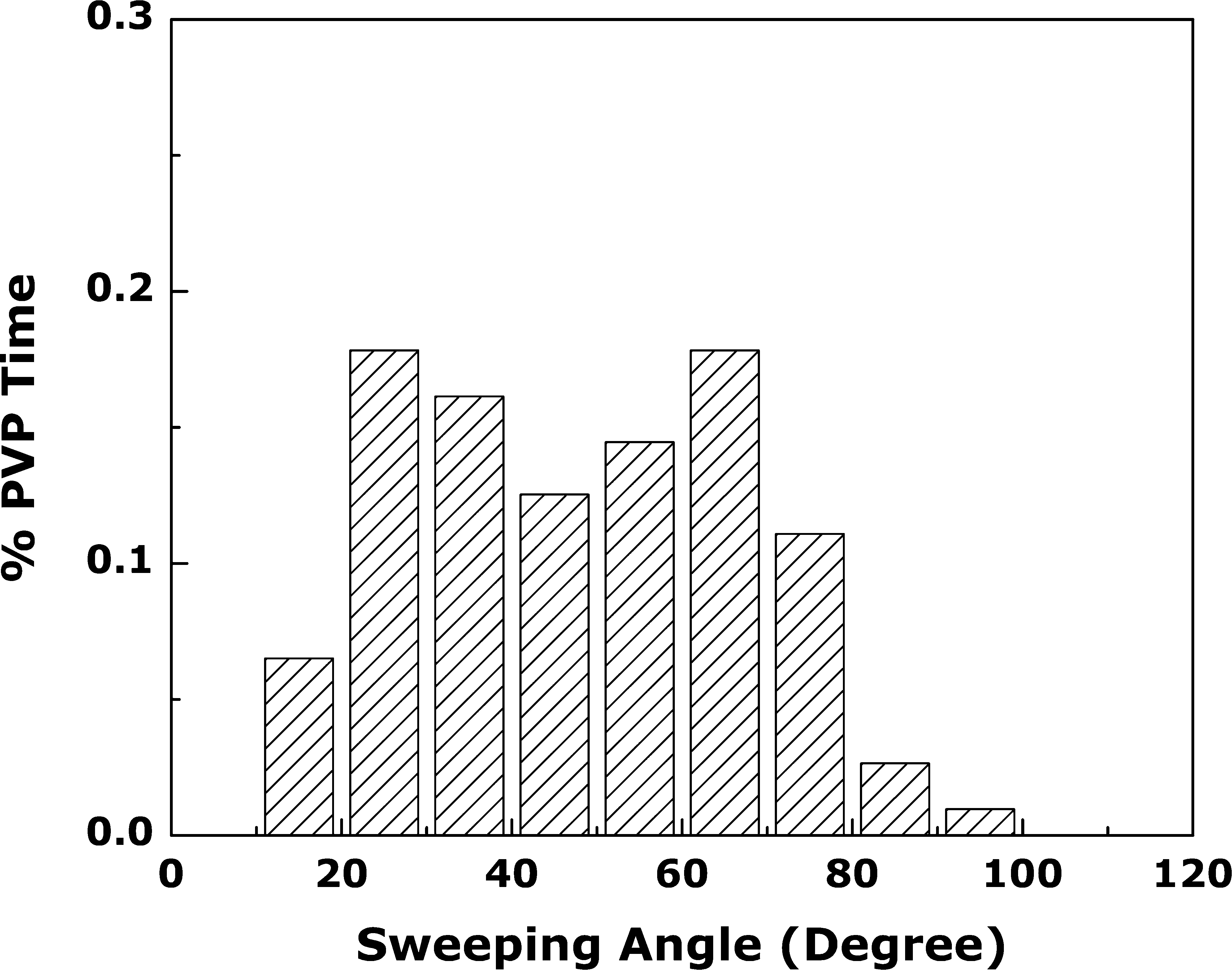
Clinical photovaporization video analysis. Percent of photoselective vaporization of the prostate (PVP) time spent at each sweeping angle from 10 random minutes of clinical PVP. Note that sweeping speed=o.5 sweep/sec.
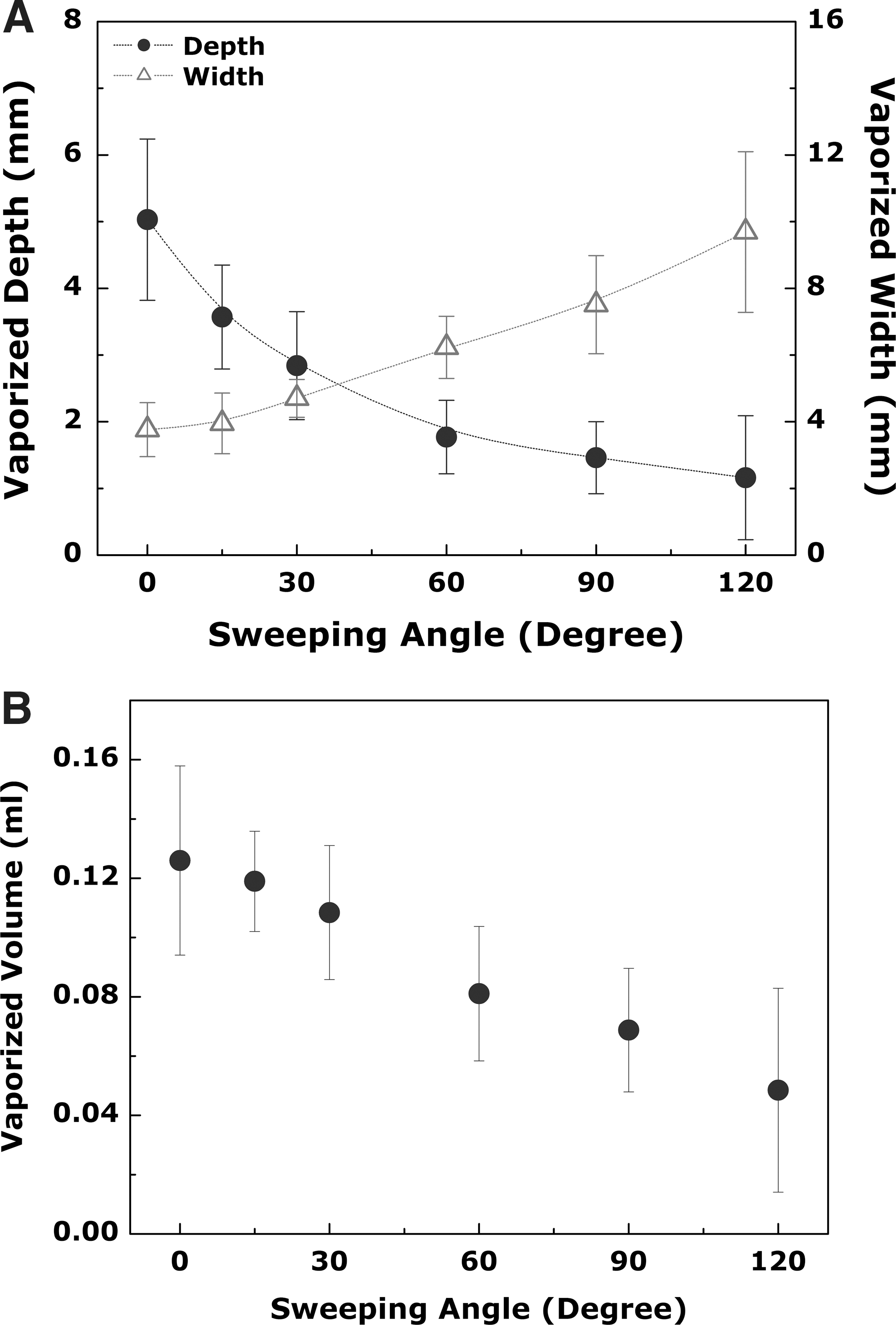
For experimental analysis in the bovine prostate model, we selected six different sweeping angles for analysis, ranging from 0 to 120 degrees. Using a computer-assisted motorized system for PVP on bovine prostatic tissue sections (Fig. 2), we found that wider sweeping angles, while generating increased vaporization widths, resulted in significantly more shallow vaporization depth, as depicted in Figure 4A. This translated to decreased vaporized volumes with increasing sweeping angles above 30 degrees (Fig. 4B). Specifically, sweeping angles of 0, 15, or 30 degrees that generated vaporization volumes were approximately 30% to 60%, 60% to 90%, and 130 to 170% larger than those volumes achieved with 60, 90, and 120 degrees, respectively (P<0.05 in all cases; Table 1, Fig. 5). Volumes generated by sweeping angles of 0, 15, or 30 degrees were not, however, significantly different from each other (Table 1, Fig. 5). These findings suggest that smaller angles of vaporization of up to 30 degrees provide the greatest vaporization volumes at a fixed sweeping speed of 0.5 sweeps/sec in this bovine prostate model.

Vaporized tissue defects and cross sections for various sweeping angles.
Vaporization volumes achieved with rotational angles of 0, 15 or 30 degree were not significantly different from each other, but were significantly greater than those achieved with rotational angles of 45, 60 and 90 degree (∼ 1.5-3.0X; P<0.05) For angle 0 degree vs 15 degree (P=0.35), vs 30 degree (P=0.1) vs 60 degree (P<0.005) and vs 90 degree (P<0.005). For angle 15 degree vs 30 degree (P=0.25), vs 60 degree (P<0.005), vs 90 degree (P<0.005). For angle 30 degree vs 60 (P=0.015), vs 90 degree (P<0.005). For angles greater than or equal to 60 degree, vaporized volumes were significantly reduced.
Volume (cc)=Mean±1SD.
Two-sample t-test with unequal variance.
Given the reported tissue coagulation margin at 1.5±0.3 mm, we then measured the coagulation depth at varying sweeping speeds at 120W. 10 At 0, 15, and 30 degrees, depths of coagulation were similar at 1.10 mm±0.13, 0.97 mm±0.14, and 1.08 mm±0.12, respectively (Table 2). As depicted in Figure 6, however, with sweeping angles above 30 degrees, coagulation depth increased in linear fashion. Specifically, there was a 16%, 26%, and 18% increase in coagulation depth with 60 degrees vs 0, 15, and 30 degrees, respectively. If the sweeping arc was increased to 120 degrees, there was an overwhelming 70% increase in coagulation depth when compared with 30 degrees.
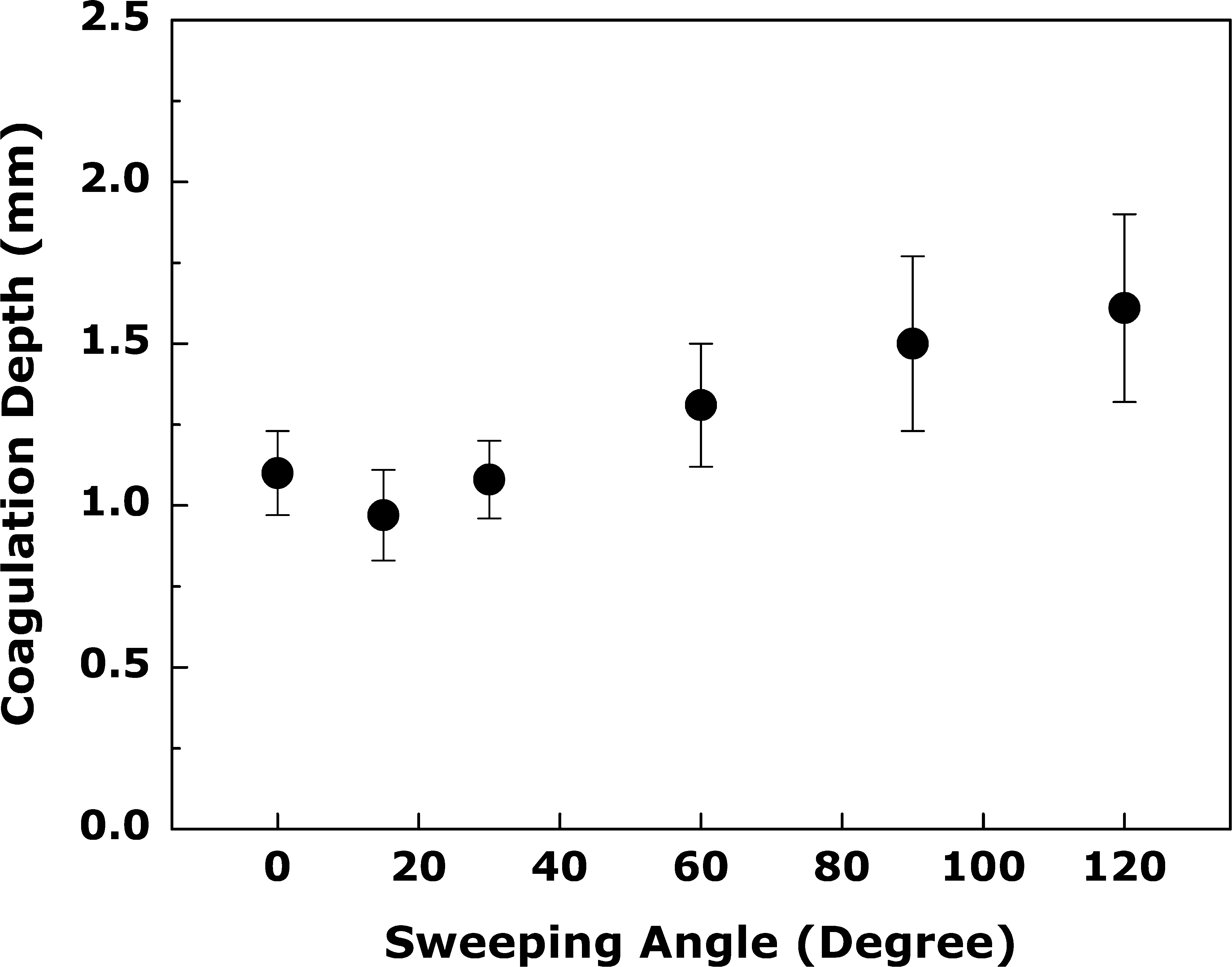
Coagulation depth as function of sweeping angle±1 standard deviation. P values all <0.05.
P-values all <0.05.
Coagulation depth (CD; mm)=Mean±1SD.
Two-sample t-test with unequal variance.
Discussion
PVP has become a surgical alternative compared with traditional TURP for the treatment of patients with LUTS that is secondary to BPH. Scientific validation of PVP technique and its impact on clinical outcome(s) is currently lacking. 28 Despite this, laser fiber sweeping motion is a virtually universal practice among urologists who perform PVP. We previously reported that slower speeds of sweeping during PVP in a bovine model lead to more efficient vaporization without increase in a coagulation effect. Here we studied whether changes in the angle of a laser fiber sweeping can similarly affect vaporization efficiency. While anecdotally based advice from current literature exists, 28 scientifically validated recommendations regarding the angle of PVP are not previously reported.
To test the effect of varying angles on vaporization efficiency, we used the 120W GreenLight HPS system with an ex-vivo cadaveric bovine prostate animal model. We selected rotational angles of 0 to 120 degrees for investigation based on clinical observations of a single experienced PVP surgeon and based on what we expect to encompass a broad range of angles used by other urologists. In our ex-vivo model, we observed wider tissue vaporization with larger sweeping angles, as expected, but at the cost of a more superficial vaporization depth and significantly lower vaporization volumes. Specifically, volumes achieved with rotational angles of up to 30 degrees were not significantly different from each other, but were significantly greater by 30% to 60% vs volumes achieved with a 60-degree angle, and up to 170% greater than volumes achieved with even larger angles. This study thus identifies sweeping angles of 30 degrees or less as most efficient in the cadaveric bovine prostate model.
These findings somewhat contrast previous recommendations suggesting that a wider sweeping arc—ie, 60 degrees—is a more efficient means of vaporization. 28 Accordingly, our experienced surgeon performing clinical PVP spent only 25% of the time using angles ≤30 degrees, and the vast majority of time was spent at larger angles, which in on our ex-vivo model proved to be less efficient. Nevertheless, it is remains to be determined whether the ≤30-degree angle identified in our bovine model will prove most efficient in the clinical setting as well. We anticipate, however, that the general concept of more efficient vaporization at lower angles will stand. Of note, given the similar vaporization efficiency of 0, 15, and 30 degrees, a 30-degree angle may be preferable clinically because of the wider surface area of exposed underlying tissue allowing better visualization (eg, of blood vessels/active bleeding), in contrast to the narrower groove created with 0 or 15 degrees.
The mechanism behind increasing PVP efficiency with smaller sweeping angles is unclear, but it is possible that the more narrow angles provide for more concentrated delivery of laser energy. In contrast, at larger angles, the dispersal of energy and thus lower “effective” wattage (ie, 30W) may predominate, diminishing the efficiency of PVP and increasing coagulation. Previous studies by Kang and coworkers 31,32 used histologic analysis of bovine prostate tissue after PVP on hematoxylin and eosin stain and confirmed a clear correlation with gross coagulative rims; however, such studies did not measure the impact of changes in sweeping angle as in Figure 5. To confirm this theory, we examined the gross coagulation depth of tissue at varying sweeping angles (Table 2) and discovered a linear relationship between increasing laser fiber rotational angle and depth of coagulation at larger angles (≥30 degrees) (Fig. 6). Interestingly, a 60-degree arc, as recommended by Gomez and colleagues, 29 resulted in nearly 20% more coagulation than smaller angles in our model.
The ex-vivo bovine prostate model has inherent limitations that may limit its impact to clinical translation. Our unique ex-vivo model uses cadaveric bovine prostates that lack active blood perfusion, thereby impacting the absorption of PVP via the hemoglobin chromophore, and thus diminishing vaporization efficiency. Despite this, correlate PVP studies in a canine model demonstrate effective vaporization of cadaveric prostate tissue; however, it was estimated 50% decreased efficiency. 33 Nonetheless, the bovine model may provide a particularly valuable resource because of its structural similarities.
Overall, evidence for optimal PVP efficiency is lacking, with only anecdotal advice suggested. This study has established more specific standards for laser fiber movement and achieving optimal tissue vaporization. During clinical PVP, however, several visual cues signify efficient vaporization to the urologist, such as the creation of tissue cavities or the vigorous formation of vaporization bubbles, which can also be heard or tacitly appreciated. Our conclusions regarding the potential value of lower rotational angles are not meant to replace the ability of the urologist to monitor and respond to these cues in real time, but simply to complement them.
Conclusion
There have been few attempts to scientifically validate PVP surgical techniques. This study follows up our previous study, which provided the first experimental investigation of the laser fiber sweeping technique commonly used by urologists. 31 We conclude that in an ex vivo bovine prostate model, larger sweeping angles are less efficient, generating wider but significantly more shallow vaporization defects, and with increased coagulation. Smaller sweeping angles of up to 30 degrees on the other hand may provide the most efficient vaporization, with minimal coagulation effect. While our ex-vivo bovine prostate model may have inherent limitations, we suspect the mechanistic principle(s) behind our findings will translate to clinical PVP. In the meantime, this study highlights that PVP technique can be tested in a standardized, scientific fashion, to best identify parameters for achieving optimal tissue vaporization efficiency.
Footnotes
Acknowledgment
This study was supported by American Medical Systems, Inc, Minnetonka, MN.
Disclosure Statement
No competing financial interests exist.