
Abstract
Background and Purpose:
The Single Port Instrument Delivery Extended Reach (SPIDER) surgical system was developed for true continuous instrument triangulation during laparoendoscopic single site (LESS) surgery. We present our initial preclinical experience with the SPIDER surgical system during renal surgery.
Material and Methods:
Bilateral laparoscopic nephrectomies were performed in a live adult porcine animal model using the SPIDER device. A standard surgical approach was used via direct video guidance.
Results:
The procedure was successfully performed without surgical error or complication. The SPIDER system proved easy to use with only a minimal learning curve. Intracorporeal surgical knots were tied without difficulty using this single site system.
Conclusions:
Our initial experience with the SPIDER surgical system during renal surgery is promising. SPIDER allows for true single port instrument triangulation offering a superior operative experience to currently available LESS surgical systems.
Introduction
To address these shortcomings, TransEnterix Inc. (Durham, NC) has developed the Single Port Instrument Delivery Extended Reach (SPIDER) surgical system for true single port instrument triangulation allowing for improved operative views. This novel device was recently reported with favorable results in a series of porcine cholecystectomies. 3 We describe our initial preclinical experience with the SPIDER surgical system during a bilateral laparoscopic nephrectomy in an adult pig.
Material and Methods
SPIDER surgical system design
The flexible SPIDER surgical system was developed to allow for continuous instrument triangulation within the abdominal cavity via a single site approach. The SPIDER system is a sterile and disposable device that has the potential for use in a variety of transabdominal laparoscopic procedures.
The SPIDER system is composed of three major components: A multichannel port (main cannula), flexible extended reach instrument delivery tubes (IDTs), and a retractable sheath (Fig. 1a–d). The main cannula has four usable instrument channels: Two lateral, one superior, and one inferior (Fig. 1b). The two lateral channels contain the IDTs (Fig. 1d) for the passage of specialized flexible instruments (True Left FLEX and True Right FLEX). These flexible instruments include a wavy grasper, fenestrated grasper, Maryland dissector, 5-mm Hem-o-lok clip applier (Teleflex Medical, Research Triangle Park, NC), shears, monopolar hook, and suction-irrigator. The IDTs allow for full three-dimensional motion of instruments with complete 360 degrees of rotation at the distal end. The superior and inferior channels are static and have diameters of 12 and 5 mm, respectively. These ports allow for the passage of an endoscope as well as traditional laparoscopic instruments. A SPIDER rigid grasper is available for use with these ports (Fig. 1d).
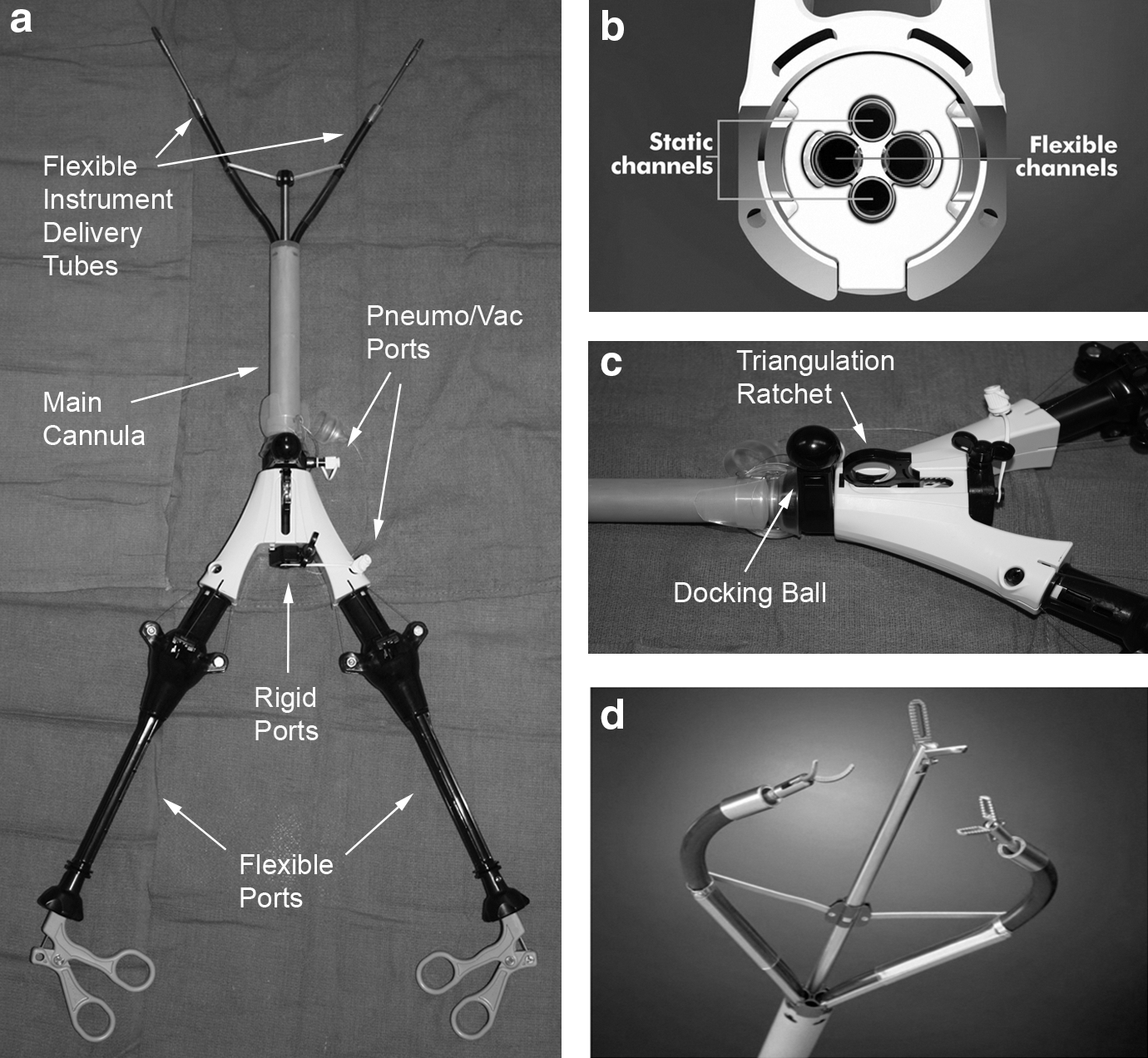
The main cannula has a surrounding retractable sheath with a disposable pointed cap. The sheath extends to cover the distal end including the IDTs (Fig. 2a) and serves to protect internal organs from damage on insertion and removal of the device. In total, the diameter of the SPIDER system is 18 mm and may be introduced via a single cut-down incision.

After insertion, the angle of the IDTs can be adjusted using the device's triangulation ratchet (Fig. 1c). Pneumoperitoneum is achieved by way of three pneumo/vac ports and is maintained by one-way valves. These ports may be used for both insufflation and smoke evacuation. The device is secured by a docking ball (Fig. 1c) that attaches to a stabilizing support arm and a bed clamp (Fig. 2b). The docking system allows for secure rotational movement of the device and is easily loosened via a “wing-nut” mechanism that allows rapid optimal repositioning.
Animal testing
The SPIDER system was tested in a preclinical porcine nephrectomy model for ergonomic ease of use and accuracy. Previous approval was obtained from the University of Miami animal use committee. A single 2-cm midline incision was made. After insertion, the SPIDER sheath was retracted, disposing the cap and exposing the IDTs. Flexible instruments were inserted through the IDT ports, and an endoscopic camera was inserted through one of the static ports. Visualization was achieved with a 5-mm diameter × 50-cm length bariatric endoscope (Karl Storz, Tuttlingen, Germany). The SPIDER device was secured with the docking system (Fig. 2b). Vascular control was planned with both hemostatic clips and suture ligation so as to determine the ease of use in performing complex laparoscopic maneuvers that typically require triangulation and are extremely challenging during LESS.
Results
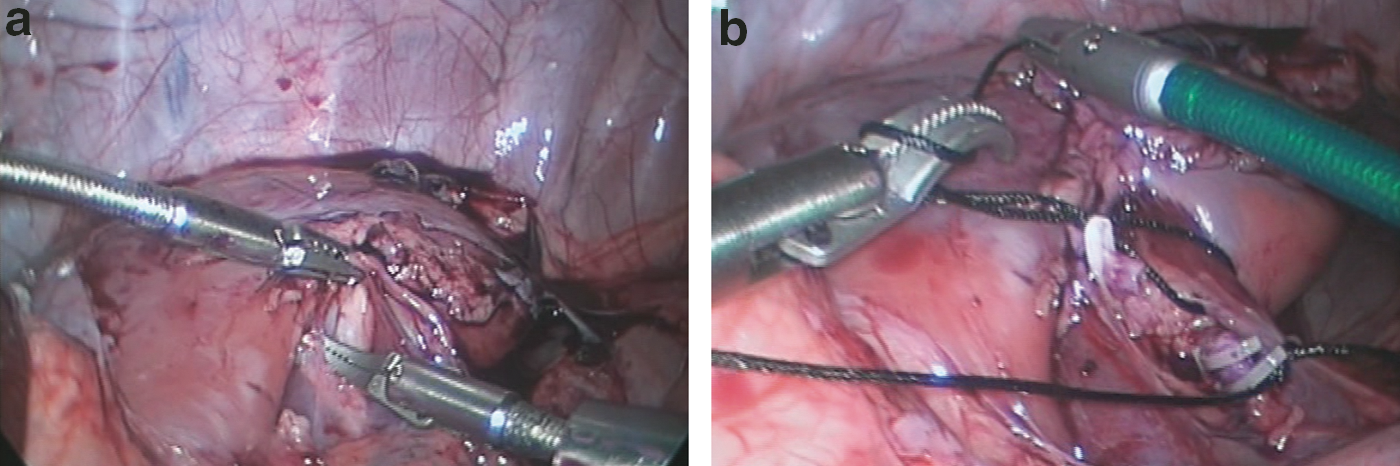
Bilateral nephrectomies were successfully performed by an experienced laparoscopist in a female Yorkshire pig (50 kg). A standard laparoscopic approach occluding the renal artery, then vein was used (Fig. 3a). A wide working envelope adequate for renal surgery was successfully accessed.
Visualization was achieved with a 5-mm diameter x 50-cm length endoscope. Both 0 and 30 degree lenses were used. Throughout the procedure, the scope remained securely in place within the 5-mm static port. The view was successfully maintained by the surgeon without the aid of an assistant.
The custom-designed flexible instruments were used without difficulty. At several points in the case, a third rigid instrument was used via the static port to aid in tissue retraction. Suction and irrigation were performed with the SPIDER flexible suction-irrigator. Intracorporeal laparoscopic surgical knots using 2-0 silk ligatures were tied around the hilar vessels with ease. Medium-large (5 mm) Hem-o-lok clips were also used for hemostasis (Fig. 3b). These clips were placed using the SPIDER flexible clip applier. At no point in the procedure did we experience instrument crossing or collision. The case was successfully performed without surgical error or complication. In total, the SPIDER system was found to be easy to use with only a minimal learning curve.
Discussion
The first laparoscopic nephrectomy was performed by Clayman and associates in 1991. 4 Since that time, urologists have strived to improve this minimally invasive procedure. One approach that has received recent attention is LESS surgery. 1,2 In comparative studies, LESS has been found to be associated with decreased postoperative pain as well as recovery time. 5 –7 Moreover, LESS leads to improved comesis because of the need for only a small single incision, typically made at the umbilicus.
At present, there exists no ideal platform for LESS surgery. Currently available technologies include multichannel port systems (TriportTM and QuadportTM) from Olympus KeyMed (Southend-on-Sea, Essex, UK) as well as the GelPointTM system from Applied Medical (Rancho Santa Margarita, CA). These technologies are limited by loss of triangulation and instrument crossing/crowding, leading to a frustrating and at times difficult surgical experience. In an attempt to minimize these shortcomings, robotic-LESS (R-LESS) has been developed. Using currently available robotic technology, R-LESS has been reported with favorable results in a series of human radical prostatectomies. 8 The authors, however, do report some degree of instrument clashing even with removal of the fourth robotic arm.
To further improve existing robotic technology, the VeSPA R-LESS platform was recently introduced. 9 This system further minimizes instrument interference by using specially designed curved robotic cannulas and semirigid instruments. This platform is similar in concept to that of the SPIDER system. To date, this platform has only been reported in a preclinical model and is not currently available for routine clinical use. While offering improvements above “traditional” LESS, R-LESS is limited by significant cost and issues of availability.
The novel SPIDER surgical system was specifically engineered to overcome the limitations of currently available LESS systems. SPIDER uses flexible instruments that allow a full range of three-dimensional movement and 360 degrees of rotation. This design fixes the camera at the center of the instruments and allows the surgeon to simultaneously control the view as well as instrumentation, thus maintaining constant triangulation within the peritoneal cavity. Using this system, the surgeon need never to operate cross-handed, which may lead to improved safety.
To date, the SPIDER surgical system has only been described in one other preclinical study. 3 Pryor and coworkers 3 detailed their experience with the device in porcine laparoscopic cholecystectomies. The authors reported favorable results consistent with our own experience. At 1 week, all animals survived the procedure. Unique to this work, the authors performed a histologic evaluation of port sites acutely and 7 days postoperatively. An increase in inflammation and tissue trauma was observed at the standard four laparoscopic port sites compared with the single insertion site of the SPIDER system. Moreover, the authors observed an increase in peritoneal and fascial injury associated with standard ports. Combined, these data support the use of the SPIDER surgical system and provide a possible explanation for the reduction in postoperative pain and scarring that is associated with LESS surgery.
In our experience, the SPIDER system proved easy to use with only a minimal learning curve. Throughout the surgical procedure, the view was maintained, allowing for excellent surgical accuracy and instrument triangulation. In addition, the specialized flexible instruments were easy to learn and allowed adequate tissue retraction and dissection. The SPIDER flexible instruments were successfully used in conjunction with ridged instruments passed through the static port. Moreover, using these specialized instruments, the surgeon was able to tie standard surgical knots with ease, similar to that of articulating laparoscopic instruments. At no point in the case did we experience instrument crossing or clashing. In our experience, currently available LESS technologies (ie, Triport, Quadport, and GelPoint) do not adequately address these issues, making them difficult to learn and impractical for routine use. This is perhaps the largest improvement of the SPIDER system.
While the results of our experience are promising, there exist limitations to the presented work. Foremost, our experience is limited to two renal units from a single animal study. Larger series are needed for a more complete evaluation of the SPIDER surgical system. Moreover, this work was limited to a porcine model. The true usefulness of this novel LESS system will be learned with translation to human surgery. The SPIDER system is already approved by the Food and Drug Administration for use in humans. Future work aims to test the SPIDER surgical system in human renal surgery.
Conclusion
This report is a proof of concept that the SPIDER surgical system can be successfully used for renal surgery. The system's novel flexible design allowed for improved instrument triangulation over currently available LESS systems.
Footnotes
Acknowledgments
The authors wish to acknowledge Susan Mazzola and Raymond Gonzalez for their work at the Center of Excellence for Laparoscopic and Minimally Invasive Surgery at the University of Miami Miller School of Medicine.
Disclosure Statement
Raymond J. Leveillee: Angiodynamics, Inc., scientific study; Covidien, Inc., scientific study/consultant; Cook Medical, lecturer; Intuitive Surgical, proctor; Applied Medical, lecturer.
Vincent G. Bird: Applied Medical, lecturer.
Nelson Salas: Angiodynamics, Inc., scientific study.
No competing financial interests exist for the other authors.