
Abstract
Purpose:
To directly compare perioperative, oncologic, and functional outcomes of laparoscopic renal cryoablation and open partial nephrectomy using a matched pair analysis.
Patients and Methods:
A total of 41 patients who underwent laparoscopic cryoablation for an incidental, solid clinical T1aN0M0 renal tumor were matched with 82 patients who received partial nephrectomy in cold ischemia, using optimal matching based on propensity scores, which were created on the basis of preoperative aspects and dimensions used for an anatomic classification of renal tumors (PADUA) score, preoperative glomerular filtration rate, age-adjusted Charlson comorbidity index, and sex. Median follow-up was 33.6 months.
Results:
No differences in the overall incidence of complications (cryoablation, 20%; partial nephrectomy, 17%; P=0.739) and grade of complications (P=0.424) were observed. After cryoablation, local recurrence developed in four patients with renal-cell carcinoma (n=35) after a median duration of 14 months (range 6–18 mos), but none after partial nephrectomy. The 3-year recurrence-free survival probabilities after laparoscopic renal cryoablation vs open partial nephrectomy were 83% vs 100%, respectively (P=0.015). The average decrease of estimated glomerular filtration rate during follow-up was 7.8±3.1 mL/min/1.73 m2 after laparoscopic cryoablation and 9.8±2.3 mL/min/1.73 m2 after open partial nephrectomy, which was not statistically significant (P=0.602).
Conclusions:
Perioperative complications and renal functional outcomes of laparoscopic cryoablation and open partial nephrectomy are similar; however, laparoscopic cryoablation confers a substantially higher local recurrence risk of about 17% after 3 years. Therefore, laparoscopic renal cryoablation should be reserved for high-risk patients with decreased life expectancy. Careful patient counseling is advocated. Study limitations include the small sample size, the lack of randomization, and the short follow-up.
Introduction
Partial nephrectomy, considered the standard treatment for patients with these small renal tumors, provides excellent oncologic and functional outcomes. 5 The overall perioperative complication rate, however, is about 20%. 6,7 In the last years, laparoscopic cryoablation has become an alternative approach, which may be recommended to patients with significant comorbidity. 8 Perioperative complications appear to be lower, 9,10 and long-term follow-up studies indicate favorable oncologic outcomes, 11 although the rate of local recurrences may be higher than expected. 12 Because low-grade (G1–2) RCCs appear to be the best candidates for cryoablation, tumor characteristics, including grade, should be determined from a renal tumor biopsy. 13
To date, however, there have been only two studies that directly compared outcomes of laparoscopic cryoablation and partial nephrectomy. Both studies accrued relatively few patients, did not report functional outcomes, had relatively short follow-up duration, and did not consider the anatomic characteristics of compared tumors. 9,10 Thus, the aims of this study were to directly compare perioperative, oncologic, and functional outcomes of both procedures on a larger cohort using a matched pair analysis.
Patients and Methods
Study design
After obtaining Institutional Review Board approval for this nonrandomized retrospective study, we queried our institutional renal tumor database and identified 294 patients who underwent laparoscopic renal cryoablation (n=41) and open partial nephrectomy (n=253) in cold ischemia for an incidental, solitary, solid, clinical T1aN0M0 renal mass between 2004 and 2010. The patient selection criteria for cryoablation and open partial nephrectomy were not established with a standardized protocol. Rather, patients discussed the options with the treating urologist. The decision to proceed with cryoablation was a consensus between the treating urologist and the patient. The decision was mainly based on anatomic tumor factors, age, and comorbidity.
Clinical, demographic, and pathologic data were collected for each patient. Comorbidity conditions at the time of surgery were assessed from preoperative clinical records, and age-adjusted Charlson comorbidity index (ACCI) was calculated. 14 Preoperative chest radiography and a CT or MRI scan of the abdomen were performed at the department of radiology, Medical University of Vienna. For the purpose of this study, preoperative as well as follow-up imaging studies were reviewed by one dedicated uroradiologist (GHP). Tumors were classified according to the preoperative aspects and dimensions used for an anatomic classification of renal tumors (PADUA). 6 The parameters of the PADUA classification include: (1) Polar location: Superior/inferior (1 point) or middle (2 points); (2) tumor deepening into the parenchyma: ≥50% exophytic (1 point), ≤50% exophytic (2 points), or endophytic (3 points); (3) rim location: Lateral (1 point) or medial (2 points); (4) renal sinus involvement: Involved (2 points) or not involved (1 point); (5) involvement of the urinary collecting system: Not involved (1 point), dislocated/infiltrated (2 points); and (6) tumor size: ≤4 (1 point), 4.1–7 (2 points), or >7 cm (3 points).
Laparoscopic renal cryoablation
For laparoscopic renal cryoablation, the access was dependent on tumor position. Patients were placed in a 45-degree modified flank position for transperitoneal access (Veress needle) of anterior tumors (n=21) and in a 90-degree full flank position for retroperitoneal access (Hasson technique) of posterior tumors (n=20). Three ports were placed for the entire operation. After exposure of the tumor, a needle frozen-section biopsy was performed, even if a pretherapeutic biopsy had been performed earlier. Diagnosis of RCC was not necessary to proceed with the ablation. Ultrathin cryoprobes (median 6, range 3–6) were placed under ultrasonographic guidance (Galil Medical, Yokneam, Israel). A median of 2 (range 2–4) freeze-thaw cryoablation cycles were performed. The ice ball was monitored via ultrasonography. After removal of the cryoprobes, hemostasis was achieved using biopolar coagulation and a biologic hemostatic agent (Floseal, Baxter, Deerfield, IL). A percutaneous drain was inserted and removed after 24 to 48 hours.
Follow-up consisted of office visits, physical examination, measurement of serum creatinine and subsequent estimated glomerular filtration rate (eGFR), and radiologic surveillance with an abdominal CT or MRI scan quarterly in year 1, every 6 months in year 2, and annually thereafter. In addition, radiography of the chest was performed annually.
Matched pair analysis
The goal of this study was to perform matched pair analysis; each patient who was treated with laparoscopic renal cryoablation was matched with two patients from the cohort of 253 patients who were treated with open partial nephrectomy in cold ischemia (median ischemia time 20 min, range 11–40 min). Even if laparoscopic partial nephrectomy is performed regularly in our center, 7 our standard approach for partial nephrectomy is the open procedure. Thus, matched pairs were generated with patients who underwent open partial nephrectomy.
At our institution, retroperitoneal open partial nephrectomy is performed through a flank incision. The kidney is completely mobilized within the Gerota fascia, and perirenal fat over the tumor is maintained. Hilar clamping is performed with Satinsky clamps. Renal hypothermia is achieved through surface cooling with ice slush. After excision of the tumor with a margin of healthy parenchyma, transected blood vessels are secured with sutures. The renal parenchyma is sutured over Surgicel® bolsters. The hilum is then unclamped.
Patients were matched for ACCI, PADUA score, preoperative eGFR, and sex, using optimal matching, which finds the matched samples with the smallest average absolute distance across all matched pairs based on propensity score. Propensity score distribution of the matched groups is depicted in Figure 1. Surveillance after partial nephrectomy was performed according to a consistent protocol. 15

Distribution of propensity scores of matched patients who underwent cryoablation and partial nephrectomy, demonstrating good matching results.
Outcome measures and statistical analysis
The following outcomes were assessed: Perioperative complications, survival, and renal function. Perioperative complications were graded using the modified Clavien classification. 16 The oncologic end point of this study was recurrence-free survival, which was calculated from the date of operation to the date of local recurrence. Local recurrence was defined according to Working Group on Image-guided Tumor Ablation criteria. 17 Functional outcomes were based on eGFR, which was calculated according to the Modification of Diet in Renal Disease formula. The percent change in the eGFR from baseline, defined as (absolute change/baseline)×100, was assessed in every patient. Chronic kidney disease (CKD) was defined as an eGFR <60 mL/min/1.73 m2.
Group differences in continuous and categorical data were compared using two-tailed Student t tests and chi-square tests, respectively. Intrapersonal changes in eGFR were assessed using paired t tests. Recurrence-free survival probabilities were estimated with the Kaplan-Meier method. A log-rank test was performed to compare recurrence-free survival after cryoablation and partial nephrectomy. All analyses were performed with the statistical package R-2.10.1 (
Results
Patient and tumor characteristics are shown in Table 1. Groups were well balanced with regards to age, sex, ACCI, PADUA score, preoperative eGFR, tumor size, subtype, and Fuhrman grade. Patients undergoing laparoscopic cryoablation tended to be older, but this difference did not reach statistical significance. Median ischemia time during open partial nephrectomy was 22 min (mean 24 min, standard deviation 20 min).
ACCI=age-adjusted Charlson comorbidity index; PADUA=preoperative aspects and dimensions used for an anatomic classification of renal tumors; RCC=renal-cell carcinoma; eGFR=estimated glomerular filtration rate.
Perioperative complications
Complications after laparoscopic renal cryoablation were observed in eight (20%) patients. The complications consisted of a urinary leak ultimately necessitating nephrectomy after unsuccessful treatment with an internal ureteral splint (n=1), acute renal failure necessitating chronic dialysis in a patient with preexisting chronic renal insufficiency (preoperative GFR 20 mL/min/1.73 m2) (n=1), a large perihepatic hematoma that was managed conservatively (n=1), prolonged gross hematuria resolving spontaneously after 1 week (n=1), prolonged hypoxemia (n=1), ileus (n=1), and impaired wound healing (n=2). According to the modified Clavien classification, there were three grade 1 (7%), three grade 2 (7%), and two grade 4 (5%) complications.
Compared with open partial nephrectomy, the overall incidence of complications was similar (20% vs 17%, P=0.739). Further, no difference in the grade of complications was observed (P=0.424) (Table 2). Complications after open partial nephrectomy were: Impaired wound healing (n=3), urinary leak (n=3), pneumonia (n=1), bleeding necessitating transfusion (n=2), life-threatening bleeding necessitating open revision (n=1), pseudoaneurysm necessitating radiologic intervention (n=1) pneumothorax necessitating a chest tube (n=1), and other medical complications (n=2).
The overall incidence (P=0.739) and grade of complication were similar (P=0.424).
Recurrence-free survival
After a median follow-up of 33.6 months (range 3–52 mos), no patient had metastases or died because of RCC after cryoablation. Local recurrence developed in four (11%) patients with RCC (n=35) after a median duration of 14 months (range 6–18 mos). Previous imaging did not show local evidence of disease or persistent enhancement in any case, thereby excluding technical failure. In all patients, salvage laparoscopic nephrectomy was performed and revealed vital clear-cell RCC. Currently, all these patients are alive without evidence of disease. During follow-up, asymptomatic renal arteriovenous fistulas developed in two patients.
In contrast, there were no local or systemic recurrences after open partial nephrectomy. The 3-year recurrence-free survival rates after laparoscopic renal cryoablation vs open partial nephrectomy were 83% (standard error [SE], 8%) vs 100%, respectively. This difference was statistically significant (P=0.015, Fig. 2).
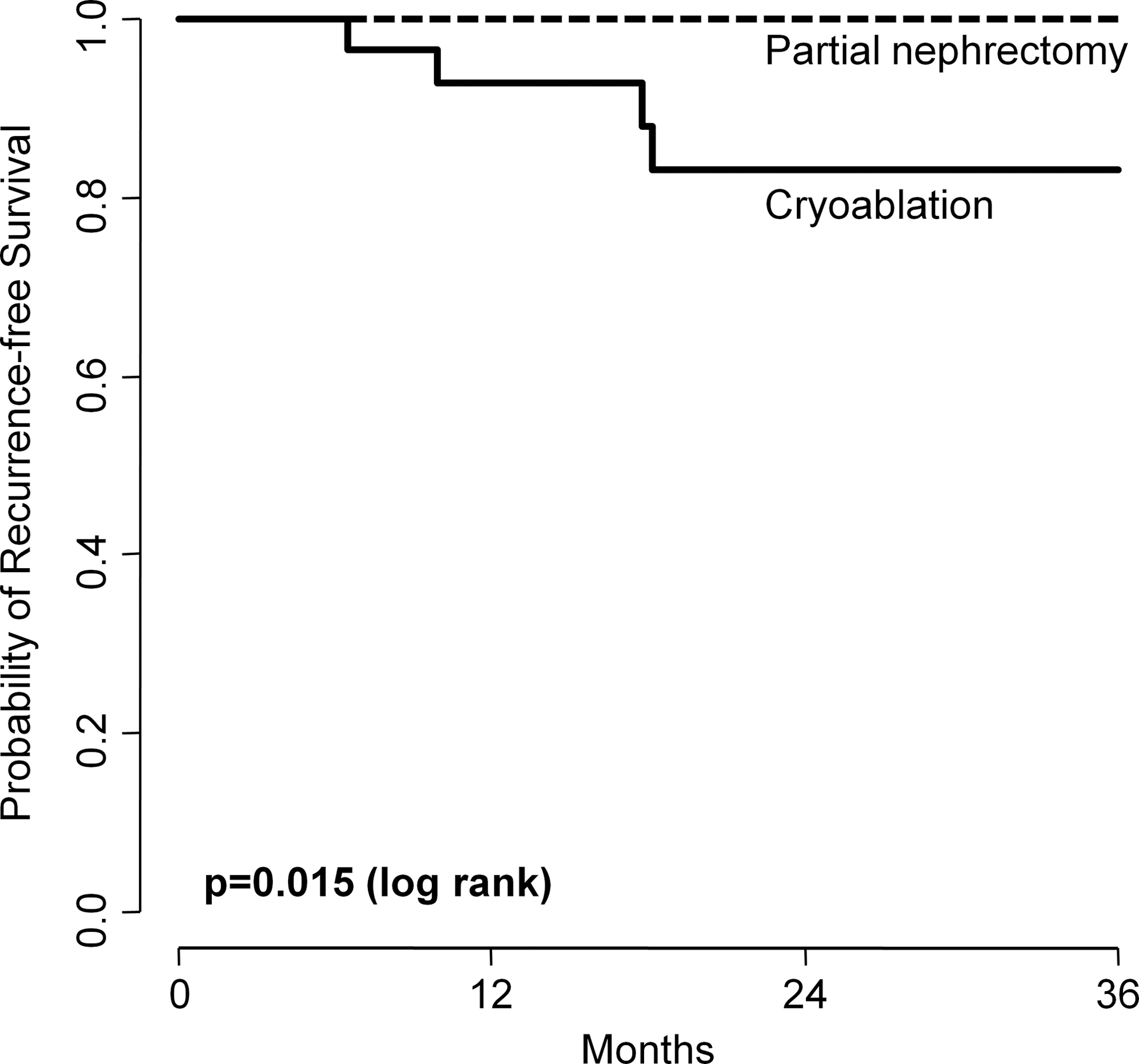
Kaplan-Meier recurrence-free survival estimates after renal cryoablation or open partial nephrectomy for renal-cell carcinoma. The incidence of local recurrence was significantly increased after laparoscopic renal cryoablation (P=0.015). The recurrence-free survival probabilities after 3 years for laparoscopic cryoablation and open partial nephrectomy were 83% and 100%, respectively.
Renal function
Before cryoablation, CKD was present in 23 (56%) patients. Postoperative CKD developed in four patients who had normal preoperative renal function (4/18=22%). The mean (±SE) eGFR decrease after 3 months was 5.3±2.4 mL/min/1.73 m2 (P=0.049), followed by insignificant changes in eGFR at 6 months (P=0.428). Between 6 and 12 months, eGFR increased a mean of 3.9±2.3 mL/min/1.73 m2 (P=0.107), and remained stable at year 2 and 3 (P=0.738). Similarly, after open partial nephrectomy, the eGFR decreased an average of 6.4±1.5 mL/min/1.73 m2 after 3 months (P<0.001), and remained stable thereafter (P=0.285, P=0.449, P=0.118, and P=0.825). CKD developed in two patients who had normal preoperative GFR. The average decrease of eGFR after laparoscopic cryoablation and open partial nephrectomy was 7.8±3.1 mL/min/1.73 m2 and 9.8±2.3 mL/min/1.73 m2, respectively. This difference did not reach statistical significance (P=0.602). Figure 3 shows individual changes of eGFR in both groups.
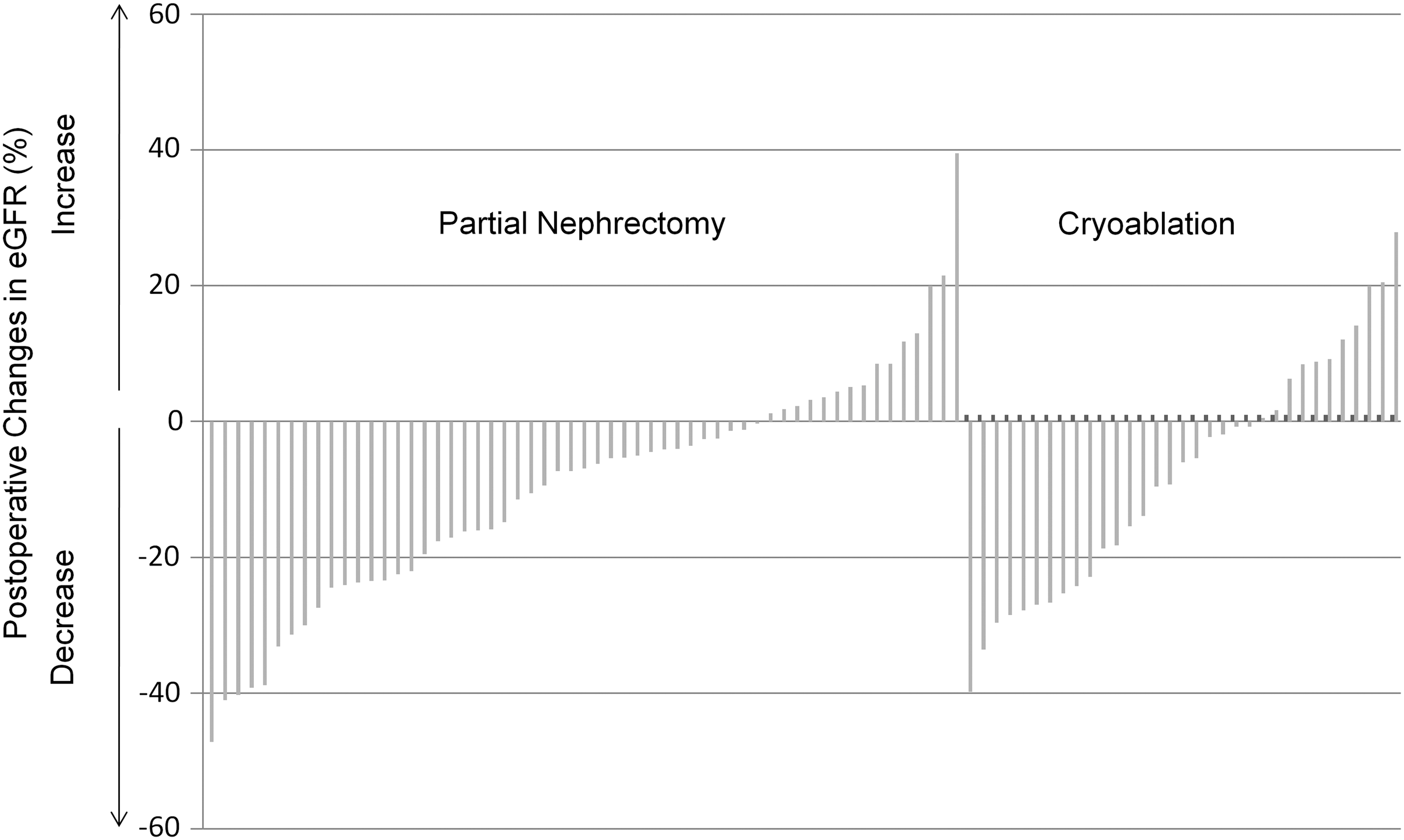
Waterfall plots showing individual changes in estimated glomerular filtration rate (eGFR) after partial nephrectomy and cryoablation. The majority of patients showed a decrease in eGFR. The average decrease in GFR after laparoscopic cryoablation and open partial nephrectomy was 7.8±3.1 mL/min/1.73 m2 and 9.8±2.3 mL/min/1.73 m2, respectively (P=0.602). A minority of patients showed long-term improvement of renal function after intervention.
Discussion
We performed a matched pair analysis of perioperative, oncologic, and functional outcomes of laparoscopic renal cryoablation and open partial nephrectomy. We found similar perioperative complication rates and renal functional outcomes; however, laparoscopic cryoablation conferred a substantially higher risk of local recurrence.
We compared the incidence and grade of perioperative complications. Today, assessment and grading of complications are performed according to the modified Clavien classification, 16 which is validated for partial nephrectomy 6,7 and laparoscopic cryoablation. 18 In our cohort, there were only two (5%) major complications, but the overall incidence of perioperative complications was 20% and thus appears relatively high. 9 This may in part be explained by the fact that other authors did not assess complications according to the Clavien classification, and that minor deviations from the normal postoperative course may not have been recorded. The rate of major complications, including urinary leak, however, is in agreement with the literature. 9,18 –20 We found two asymptomatic patients with a renal arteriovenous fistula during follow-up. This is a rare complication after cryoablation, although the incidence may be higher after long-term follow-up. Our standard radiologic follow-up procedure is a four-phase renal CT scan, in which fistulas may mimic tumor recurrence. Therefore, an additional MRI was performed.
Oncologic outcomes after laparoscopic renal cryoablation have been well documented. 19,21 –23 Recently Aron and associates 11 presented single-surgeon data on 80 patients who had at least a 5-year follow-up. Of these patients, there were 55 (69%) who had biopsy-proven RCC. In this cohort, the 5-year disease-free survival rate was 81%, mirroring the data from the current study. In case of local-regional recurrence, we performed nephrectomy in all cases, because two tumors invaded into the renal vein and two had extensive perinephric scarring. This is in accordance with results from recent studies. 24,25 In a large series, Nguyen and colleagues 25 evaluated 42 local recurrences after ablative therapy. Twenty-six underwent repeated ablation; in 10 cases, partial nephrectomy was attempted but was only possible in 2. Based on these data, one has to conclude that repeated ablation or radical nephrectomy may be the only surgical options after recurrence.
In our cohort, the rate of local recurrence was significantly higher after laparoscopic cryoablation compared with open partial nephrectomy. That is supported by a meta-analysis of 6471 lesions, where cryoablation was associated with a 7.45-fold increased risk of local recurrence compared with partial nephrectomy. 12 Two further studies directly compared laparoscopic cryoablation with partial nephrectomy. Ko and coworkers 9 analyzed 20 RCC patients undergoing laparoscopic cryoablation and 20 partial nephrectomies. Blood loss and transfusion rates were lower in patients undergoing laparoscopic cryoablation. In contrast to the current study, no recurrences occurred in both groups after a mean follow-up of 27 and 29 months, respectively. This study, however, accrued few patients, did not evaluate renal function, and showed relatively high blood transfusion rates of 40% after partial nephrectomy, which do not match data from contemporary cohorts. 6,7 In a similar study from O'Malley and colleagues, 10 15 patients who underwent laparoscopic cryoablation were matched with 15 laparoscopic partial nephrectomies. As expected, blood loss was higher in laparoscopic partial nephrectomy, but there were no other relevant early postoperative differences. Mean postoperative follow-up was less than 1 year, so that no reliable oncologic outcomes could be presented. 10
Our study shows that both laparoscopic cryoablation and partial nephrectomy in cold ischemia offer similar outcomes with regard to renal function. The eGFR ultimately decreased about 5 to 10 mL/min/1.73 m2 after both procedures, although that may not be clinically relevant in the majority of the patients. For our matched pair analysis, we chose patients who underwent partial nephrectomy in cold ischemia, which represents the standard approach at our institution and provides excellent long-term renal function. 26 It is now well established that postoperative renal function and occurrence of CKD is directly related to ischemia time, and that CKD strongly contributes to nontumor-related mortality after renal surgery. 27 Recently, a 62-patient study on renal functional outcomes after percutaneous and laparoscopic renal cryoablation has been presented. 28 Here, renal function was generally well preserved, and de novo CKD occurred in only five cases. Our study revealed comparable results. In solitary kidneys, however, cryoablation appears to be advantageous in maintaining renal function, although disease-free survival is dramatically worse. 29
One should critically question the argument that renal cryoablation represents an alternative approach for patients with significant comorbidity. 8 For both partial nephrectomy and laparoscopic cryoablation, general anesthesia is necessary. If the patient may finally need salvage surgery for local recurrence, comorbidity is no longer an argument. Despite shorter hospital stay and lower blood loss, oncologic outcomes after cryoablation are worse, 12 and complication rates and renal functional outcomes are not better. Thus, one should carefully counsel the patient and critically discuss the available approaches. According to the American Urological Association guideline, that should include partial nephrectomy and radical nephrectomy as standard options, but may include cryoablation and active surveillance. 8
There are several characteristics of the current study that merit mention. All preoperative and postoperative imaging studies were performed at one department according to a consistent protocol and reviewed by one expert uroradiologist. Thus, exact preoperative classification according to PADUA score, 6 subsequent optimal matching with partial nephrectomy patients, and exact determination of tumor status in follow-up imaging studies was possible. Unlike some authors, 11 we did not perform a 6-month follow-up biopsy, because data indicate proper correlation of radiologic and histologic findings after cryoablation. 30 In addition, all patients with suspected local recurrence underwent salvage surgery, and thus local recurrences were all confirmed by histology. Finally, using matched pairs, direct comparison of patients with identical comorbidity, tumor characteristics, and renal function was possible. The nature of our study remains retrospective, however, which limits the strength of the conclusions. Prospective randomized trials on this topic would be extremely important. Additional limitations of this study include the small sample size, the lack of randomization, case selection bias, and the relatively short follow-up.
Conclusions
Perioperative complications and renal functional outcomes of laparoscopic cryoablation and open partial nephrectomy are similar; however, laparoscopic cryoablation confers a substantially higher local recurrence risk of about 17% after 3 years. Therefore, laparoscopic renal cryoablation should be reserved for high-risk patients with decreased life expectancy. Careful patient counseling is advocated.
Footnotes
Disclosure Statement
No competing financial interests exist.