
Abstract
Purpose:
To determine the necessity of ureteral stent placement after retroperitoneal laparoscopic ureterolithotomy (RLU) for upper ureteral stones more than 1 cm.
Patients and Methods:
Between May 2006 and May 2009, 104 RLUs were performed as primary management of large upper ureteral stones. The patients were randomly divided into two groups: In group 1 (52 patients), RLU was performed without stent placement afterward, and in group 2 (52 patients), the stent was placed after RLU. The mean stone size was 16.8 cm in group 1 and 18.2 cm in group 2. The stent in group 2 was placed cystoscopically.
Results:
All procedures were performed successfully. The mean operative time was 48 minutes in group 1 vs 65 minutes in group 2. The mean drainage time was 4.1 days in group 1 vs 2.3 days in group 2. All the patients were followed up for a period of 6 months with no recorded cases of residual stone or ureteral stricture.
Conclusion:
RLU for large upper ureteral stones could be considered as a primary line for treatment as regards the economic status in developing countries. Laparoscopic ureterolithotomy (LU) without stent placement for upper ureteral stones is safe, cost effective, has less operative time, and needs no auxiliary procedures when compared with the use of stent placement after LU, which adds costs and discomfort for the patient.
Introduction
Wickham 5 was the first to describe an attempt for removal of a ureteral calculus using the laparoscope in the retroperitoneum. It was not until Gaur 6 demonstrated the concept of retroperitoneal balloon dilation, however, that retroperitoneoscopy was adopted. Many groups have described retroperitoneal laparoscopic ureterolithotomy (RLU): Some of them prefer stent placement in the ureter 7,8 and close the ureterotomy, 9,10 while others suture the ureterotomy without stent placement. 11,12 This debate had encouraged us to evaluate whether ureteral stent placement is considered as an essential step in RLU or not.
Patients and Methods
Between May 2006 and May 2009, 104 patients (86 men and 18 women) in our department underwent RLU for impacted upper ureteral stones (>1 cm at any diameter). In this study, we considered impacted stone as the stone that maintains its place in the upper ureter for more than 1 month. The present study had already been approved by the local medical research ethics committee in our university with informed consent obtained for the patients. Exclusion criteria were patients with uncontrolled coagulation disorders, advanced cardiopulmonary diseases, stone associated with radiologically diagnosed ipsilateral stricture ureter, and patients with obstructed infected kidney.
Preoperatively, background variables, including age, sex, and history, were evaluated. In addition, physical examination and laboratory evaluation, including kidney function tests and urinalysis, were performed. Also, preoperative radiologic evaluation, including intravenous urography (IVU) and ultrasonography, was performed. Patients who presented with renal colic and those with radiolucent stones underwent multislice CT for the evaluation of their stones (Fig. 1). All procedures were performed with the patient under general anesthesia. One dose of a first-generation cephalosporin was administered during anesthesia induction for all patients who were enrolled in our study.
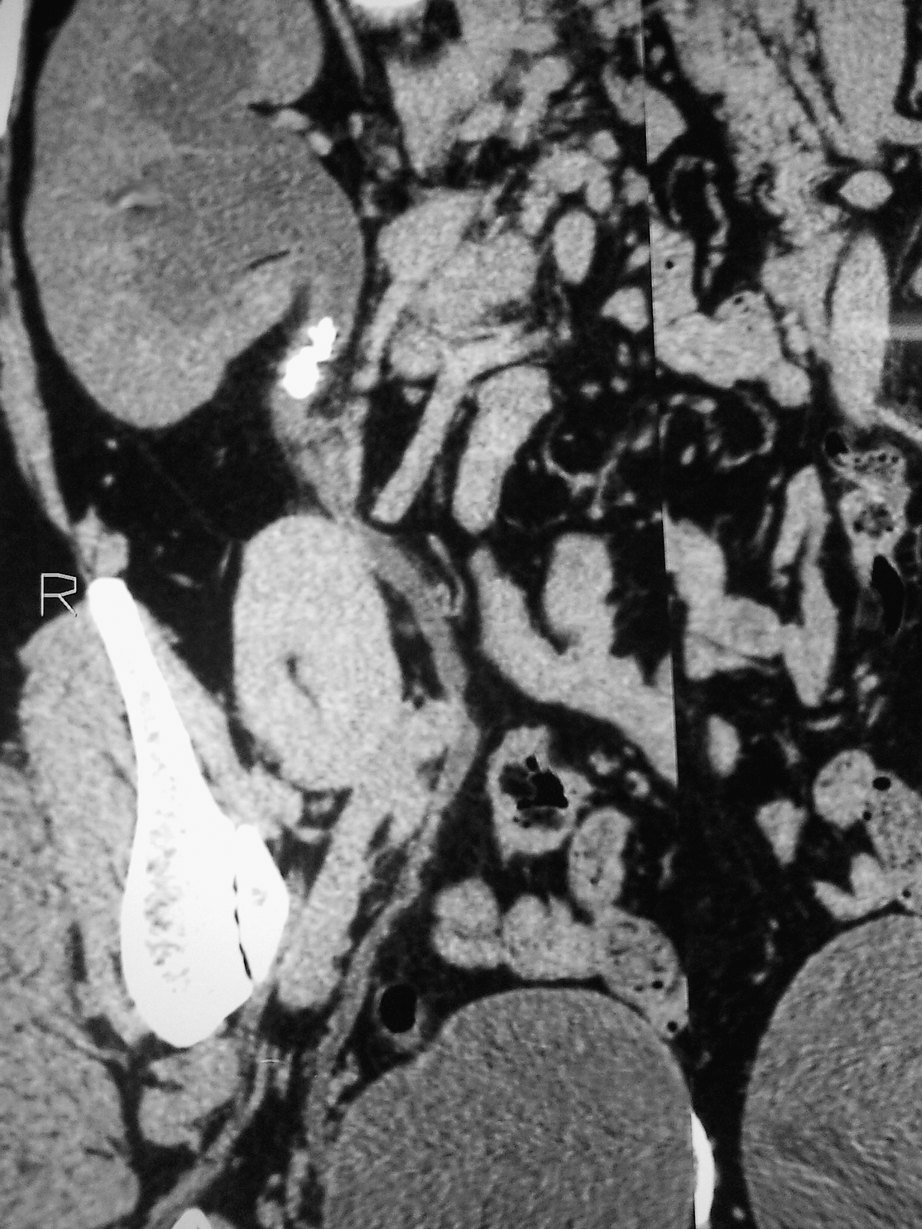
CT urography showing right impacted stone upper ureter.
Operative technique
A small skin incision (1.5–2 cm) was performed through subcutaneous tissue approximately in the posterior axillary line midway between the iliac crest and the last rib (Petit triangle). By using blunt dissection with curved artery forceps, the incision was extended through the muscles to reach the lumbar fascia, which was pierced by the tip of an artery forceps. A well-lubricated index finger (with K-Y jelly to aid finger introduction and dissection) was then introduced through the incision to peal the peritoneum medially from the abdominal wall. We did not use a balloon. Instead, we used finger dissection, which was sufficient in the creation of the retroperitoneal space. 13 Through this incision, a 10-mm port (port 1) was introduced. The second 10-mm trocar (port 2) was inserted 1 inch above the anterior superior iliac spine in the midaxillary line. A third 5-mm trocar (port 3) was inserted 1 inch below the last rib in the midaxillary line (for right-sided laparoscopic ureterolithotomy [LU]).
After trocar fixation, the retroperitoneal space was inflated with CO2. Starting with dissection of the Gerota fascia where the ureter was identified and traced until the stone bulge (Fig. 2), then the ureter was incised directly over the stone longitudinally by L-hook electrode (Karl Storz,® 3 mm) using the lowest cutting power (Fig. 3), and the stone was removed and put into a finger glove (Fig. 4), which was removed at the end of surgery.
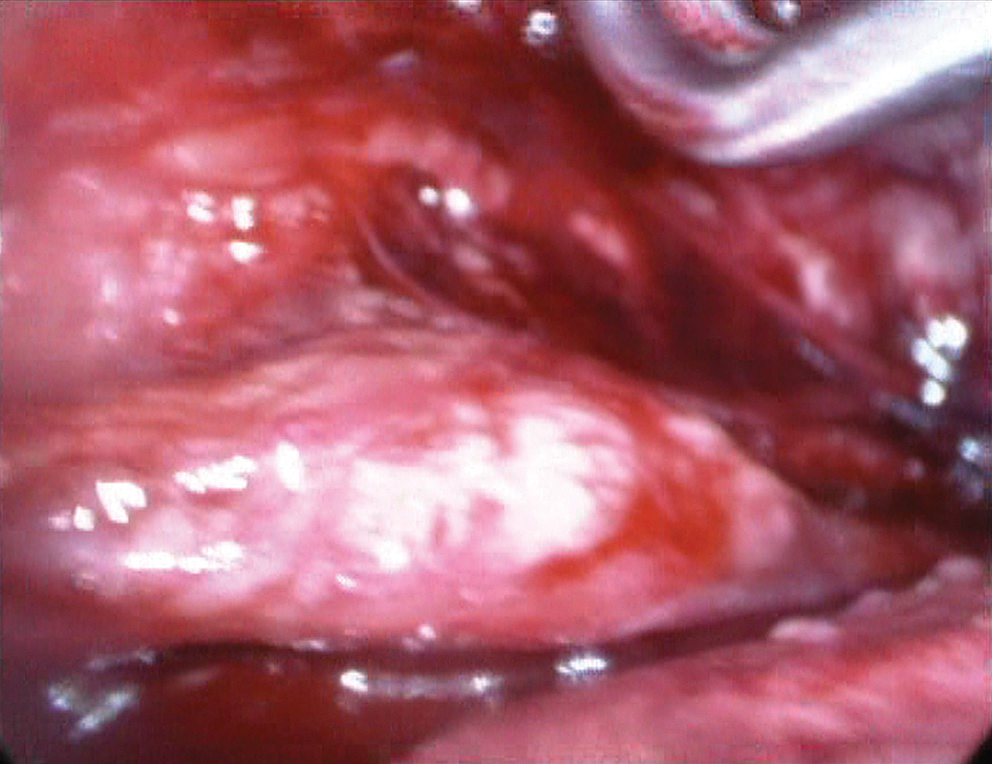
Stone bulge in the ureter.
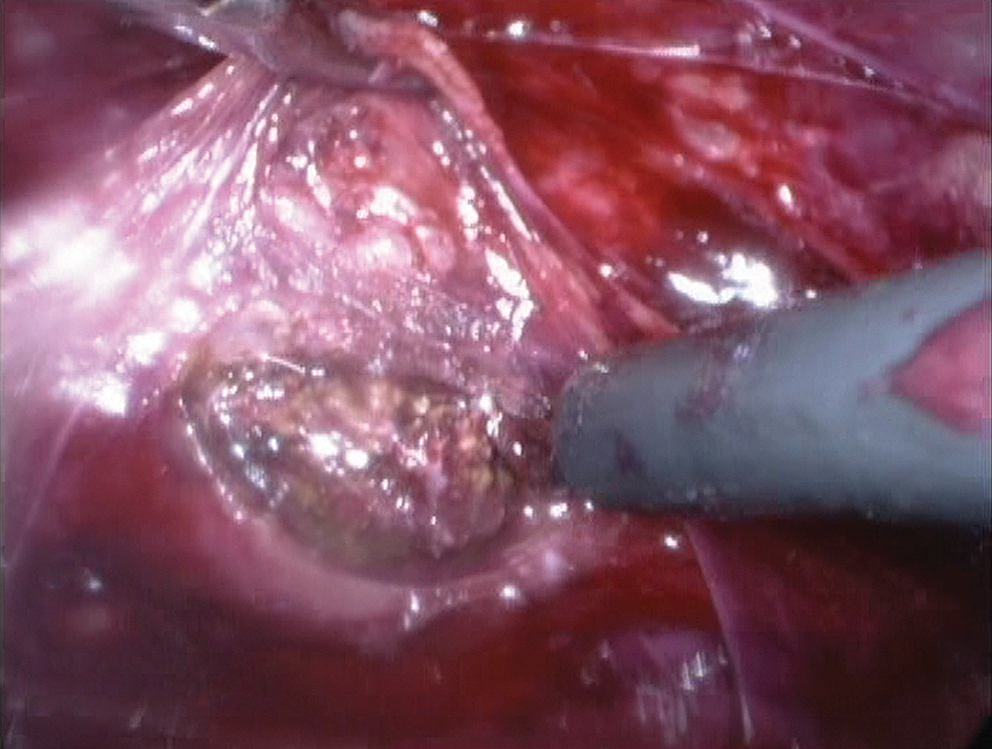
After ureterotomy, the stone was delivered out of the ureter using the hook electrode.
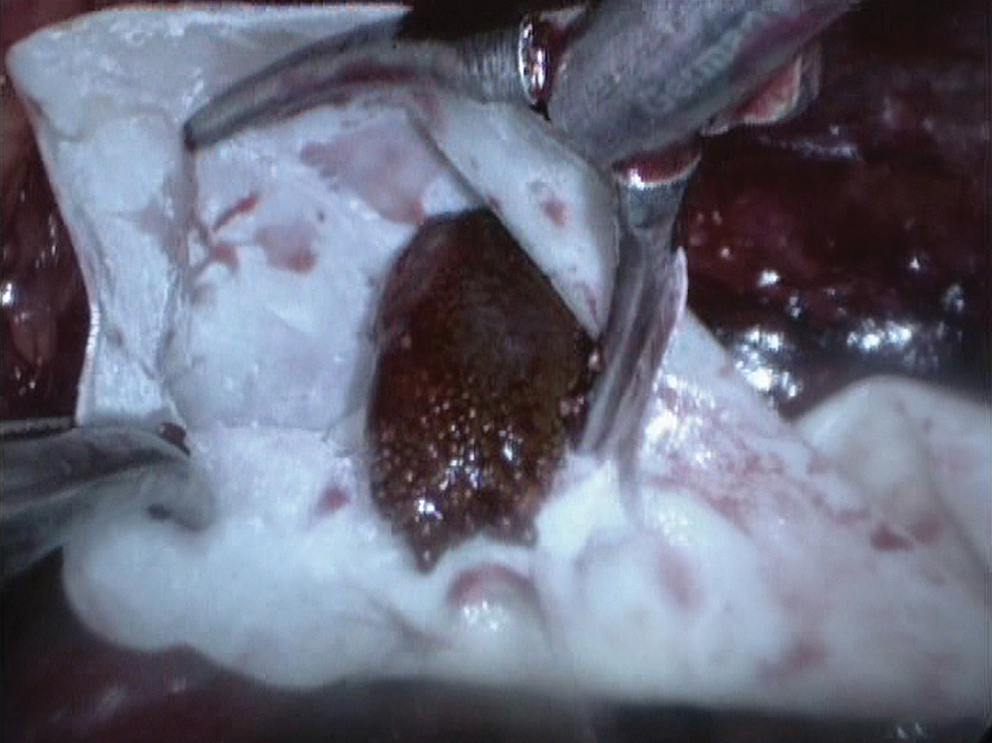
The stone was collected inside a finger glove.
Distal patency of the ureter was tested by antegrade introduction of a 5F ureteral catheter through the ureterotomy. The ureteral catheter was passed through the 5-mm port with its distal end closed by a mosquito to avoid gas leakage during this step, before which the bladder was filled with 150 mL of saline that was injected through the Foley catheter. On manual suprapubic compression, saline drops coming out of the ureteral catheter ensured successful passage of the ureteral catheter to the bladder. After testing the distal patency, the ureteral catheter was removed, and the ureterotomy was closed by approximation of the periureteral sheath using interrupted intracorporeal laparoscopic suture with 4-0 polyglactin suture. A tubal drain (20F plastic catheter) was introduced under direct vision into the second trocar site and was fixed to the skin. For cases in which indwelling stent placement was planned, a 6F 26-cm polyurethane Double-J ureteral stent (Coloplast,® Humlebaek, Denmark) was inserted cystoscopically under fluoroscopy with the patient in the lithotomy position after LU.
Both groups were compared in terms of site and mean size of the stone, operative time, intraoperative complications, mean time of drain removal, analgesic requirements, costs of the procedure, and postoperative complications. The first follow-up visit was 1 week after surgery; patients were evaluated clinically and postoperatIve symptoms were measured using a patient questionnaire that involved upper and lower urinary tract symptoms. In addition, renal ultrasonography was performed for evaluation of hydronephrotic changes. As regards IVU, it was performed if hydronephrosis was diagnosed clinically and sonographically. Monthly visits were scheduled for the patients up to 6 months postoperatively.
Statistical analysis
Statistical analysis was performed using SPSS® version 16 software. To compare the data of our two groups, t test and chi-square tests were used, with P<0.05 considered significant.
Results
The demographic data of both groups were comparable in age, sex, size, and location of the stones (Table 1). For body mass index (BMI), the American Society of Clinical Nutrition established clinical guidelines to define patients with a BMI of <25 as normal, from 25 to <30 as overweight, and ≥30 as obese. In our groups, BMIs were also comparable (25.2±0.4 for group 1 vs 26.8±02 for group 2, P=0.725).
The operation was performed by the same surgeon (AH), and the success rate was 100%, with no conversion to open surgery. The mean (range) stone size was 16.8 mm (11–21.5 mm) in group 1 vs 18.2 mm (12.3–19.7 mm) in group 2, and the difference was statistically insignificant (P=0.239). The mean (range) operative time was 48 minutes (45–72 min) in group 1 vs 65 minutes (55–95 min) in group 2, with a statistically significant difference (P=0.027). Peritoneal tears were encountered in five patients who were treated by placing a veress needle through the anterior abdominal wall into the peritoneal cavity to avoid the development of pneumoperitoneum and affecting the working retroperitoneal space. For those patients, no conversion to open surgery was needed, and there were no postoperative complications because of those tears. In group 2 patients, the Double-J stent was inserted cystoscopically under fluoroscopic guidance, and we were not faced with any difficulties during the stent insertion.
There was no statistical difference in blood loss between both groups (P=0.238), although there was a statistical difference in analgesic requirements (P=0.038) where a larger dose of intramuscular morphine in group 2 was needed. For the external drainage tube, we considered it for removal when the drainage amount was <20 mL. In our study, we found a longer time for external drainage in group 1 than in group 2 (the mean [range] drain removal time was 4.1 days [3–10 d] for group 1 vs 2.3 days [2–6 d] for group 2), although the difference was not statistically significant (P=0.0634). The drainage time was prolonged in five patients from group 1 more than 8 days, but we preferred conservation, because all of them became dry before the 11th postoperative day (Table 2). All patients were discharged from the hospital on the second postoperative day.
M = mean; SD=standard deviation.
On the follow-up visits, the patients of both groups were evaluated using a patient questionnaire. Flank pain was encountered in both groups (15.3% in group 1 vs 54% in group 2, respectively) with a statistically significant difference (P<0.05). Dysuria, urgency, and frequency were dominant with the patients from group 2 (86.5%, 80.7%, and 88.4%, respectively), while hematuria and flank pain were encountered in 77% and 54%, respectively (Table 3). Oral analgesics (diclofenac sodium 50 mg) were prescribed for the symptomatic patients, and reevaluation on a weekly base was performed until the time of stent removal. The stent was removed after 2 weeks in all patients of group 2. In the follow-up period (6 months), ureteral stricture at the site of ureterotomy or stone recurrence did not develop in any of our patients in both groups. As regards the cost of LU in our department, it was about 1500 EP ($253) in the group without a stent, while in group 2 with stent insertion, the total cost was about 2400 EP ($405).
Discussion
The innovation of modern minimally invasive methods for the management of ureteral stones has resulted in the decline of the use of open surgical approach. The 1997 American Urological Association (AUA) guideline stated that: “Open surgery should not be the first-line treatment for ureteral stone.” 14 On the other hand, open surgery is reserved for certain conditions, such as very large, impacted stones and/or multiple ureteral stones.
After Wickham 5 performed the first extraperitoneal ureterolithotomy in 1979, LU became a less invasive alternative to open surgery in this setting. In a review of the literature, most of the reports agreed with Gaur and colleagues 11 that the main indication for LU is as a salvage procedure for failed ureteroscopy and SWL. Nevertheless, all these studies reported the use of laparoscopy as a primary procedure; even Gaur and coworkers 11 used it in 24 patients in the series.
We thought, according to our results and other reports, that LU should be considered as first-line management of proximal ureteral stones >1 cm, especially if we consider that the stone-free rate (SFR) with the use of SWL and ureteroscopy was 68% and 79%, respectively, accordIng to the 2007 AUA guideline. 14 In addition to the socioeconomic factor in our community as a developing country in which LU is less expensive than SWL and ureteroscopy (in our country, LU costs about 1500 EP [$253] while SWL and ureteroscopy cost about 2700 EP [$455] and 3500 EP [$590], respectively).
In addition to the cost, most patients also want their stone removed within a single procedure so they can return quickly to their regular activities. 15 In our study, all LUs were performed as a primary procedure for managing proximal ureteral stones >1 cm with a 100% SFR. This is consistent with many series 6,15,16 that reported 100% SFR. Other studIes 11,17,18 reported SFR ranging from 75% to 95%, which was mostly attributed to initial experience, difficulty in locating the stone, vascular injury, and post-SWL retroperitoneal fibrosis.
As regards the use of PCNL for the removal of upper ureter stone, some groups concluded that PCNL is usually reserved for complex ureteral stones and stones associated with distal ureteral stricture as well as various forms of urinary diversion. 2,19 In contrast to its SFR that range between 85% and 100%, LU is less expensive and more nephron sparing than PCNL. 20,21
Using the retroperitoneal approach in LU adds many advantages to the procedure, such as avoiding intra-abdominal organ injury, keeping the urine leakage away from the peritoneal cavity, and decreasing the incidence of postoperative ileus. On the other hand, limited working space and sometimes difficulty in identifying the ureter are the main dIsadvantages of this approach. In 1992, Gaur 6 described his innovation in the retroperitoneal approach using a hydraulic balloon dilation system; since then, many authors have adopted this approach.
In our series, we created the retroperitoneal space by using finger dissection, 13 which was sufficient in creating the retroperitoneal space. In our series, the identification of the ureter was performed by the use of the gonadal vein as an anatomic landmark that is located medial to the ureter in its upper part while the stone was identifed by its bulge in the ureter and by the use of fluoroscopy in cases when the exact location of the stone was doubtful.
Nouira and associates 22 have recommended the use of cold knife for ureterotomy to prevent ureteral stricture, while many authors 1,16,17 believe that the use of the electrical hook with cuttIng mode is easier and safe. In all our cases, ureterotomy was performed by 3-mm hook diathermy, which has a very thin L-shaped hook; the lowest cutting power was used. With the use of this thin diathermy instrument, we were trying to minimize the tissue damage during ureterotomy. For the 6-months of follow-up postoperatively, stricture at the site of ureterotomy did not develop in any of our 104 patients. In addition, we used the hook electrode as a tool to lever the stone out of the ureter without the need of the spatula.
After stone extraction, testing the distal patency is crucial to rule out distal ureteral stricture. In our series, we passed a 5F ureteral catheter through the ureterotomy, and the ureteral catheter was passed through the 5-mm port with its distal end closed by a mosquito to avoid gas leakage during this procedure. Kijvikai 17 used a feedIng tube, which we believe is soft and difficult to manipulate; on the other hand, the ureteral catheter is more rigid and always available in the operating theater.
In both groups, the ureterotomy was closed by approximating the periureteral fascia using interrupted 4-0 polyglactin sutures, but it was not watertight to avoid ischemia or stenosis at the site of the ureterotomy. Postoperative ureteral strictures did not develop in any of our patients.
As regards stent placement after LU, some groups preferred to place the stent in the ureter 7,8 and then close the ureterotomy 9,10 ; other authors 23,24 left it open. Gaur 6 has left the ureter neither with a stent nor sutured in 48 patients in his series; on the other hand, some authors 11,12 did not use a stent and preferred to suture the ureterotomy to reduce urinary leakage. In cases with prolonged stone impaction and chronically inflamed ureter, Gaur and colleagues 11 have concluded that ureteral stent placement without ureterotomy suturing is indicated.
In our series, we closed the ureterotomy in all patients; moreover, in patients of group 2 after LU, we inserted a Double-J stent cystoscopically under fluoroscopic guidance during which we did not face any difficulties. In both our groups, the drainage time was statistically insignificant (P=0.0634).
Gaur and coworkers 25 had described a simple technique for laparoscopic insertion of a stent after LU with the use of a specially closed-ended stent, and they stated that there is a risk of ureteral perforation because the ends of the stent were floppy; also, there is little strain on the ureter during the introduction of the stent with the possibility of submucosal or subserosal dissection during initial stent insertion. With the effort to facilitate laparoscopic stent insertion, Khan and Khan 26 also described another technique with the use of an open-ended stent with a guidewire 1 cm longer than the stent that seems easy to perform and saves extra time and costs to the operation; in our opinion, however, it carries risk of ureteral perforation and is difficult to perform with small ureterotomies.
As regards operative time and analgesic requirement, there was a statistical difference; the stentless group had less operative time and analgesic requirement (Table 2). The longer operative time could be explained by the time needed for the stent to be inserted cystoscopically; most of this extra time was consumed in repositioning of the patient. Not only was extra time added to LU for group 2 but also there was extra cost for the stent insertion, which is about 900 EP ($152) with the additional cost for its removal later.
On postoperative follow-up, patients of group 2 had experienced bothering symptoms (Table 3) that were attributed to the indwelling stent and used larger amounts of analgesia; these symptoms were also observed by many authors 27 –29 with the use of a stent after ureteroscopy.
The most probable shortcoming of our study was that the patients had been followed up for 6 months, which could be considered a short-term follow-up, especially for evaluation of the possible incidence of ureteral stricture at the site of ureterotomy; nevertheless, the aim of this study was mainly for the evaluation of the need for a ureteral stent after LU. So, it is to be recommended that future study of LU with longer-term follow-up is needed to determine the efficacy and long-term safety of our technique.
Conclusion
RLU for large upper ureteral stone could be considered as a primary line for treatment as regards the economic status in developing countries. LU without stent placement for large upper ureteral stones is safe, cost effective, has less operative time, and needs no auxiliary procedures when compared with the use of stent after LU, which adds costs and discomfort for the patient.
Footnotes
Disclosure Statement
No competing financial interests exist.