
Abstract
Background and Purpose:
Access for percutaneous nephrolithotomy (PCNL) is critical to successful removal of stone burden and is often performed by a specialist other than a urologist. In many regions, however, there is limited availability of such personnel. We reviewed the complication rates that were related to PCNL access when performed at a teaching hospital to establish that access for PCNL may be safely taught to and performed by urology residents. Chief urology residents across the nation were also anonymously surveyed to better understand the current trends and dynamics regarding PCNL access in teaching institutions.
Patients and Methods:
A retrospective chart review was performed of all PCNLs performed at our institution from 1995 to 2009 for any complications that were related to surgery. Patients with access gained at outside institutions or not attempted at the time of surgery by residents were excluded. The complication rate was compared with those of the American College of Radiology. An eight-question survey was also sent by e-mail to all current urology chief residents regarding their experience with PCNL access during residency.
Results:
A total of 290 patients underwent PCNL with 338 separate access sites gained at the time of surgery under the supervision of nine teaching staff. Access was gained in all cases at the time of surgery. Major complications included: Transfusion in 20 (5.9%) patients, sepsis in 2 (0.6%) patients, pseudoaneurysm necessitating intervention in 2 (0.6%) patients, hydrothorax in 2 (0.6%) patients, pneuomothorax in 1 (0.3%) patient, ureteropelvic junction disruption in 1 (0.3%) patient, and one death (0.3%) after surgery. Minor complications included: Urinary tract infection in five (1.5%) patients, and collecting system injuries in 6 (1.8%) patients necessitating placement of a ureteral stent. Our survey of residents demonstrated that 53% did not routinely gain access for PCNL at their institution. The 94% who did not get instruction on PCNL access, however, thought it would be a valuable addition to their training.
Conclusion:
Our results show that access for PCNL surgery can be safely and successfully obtained by genitourinary residents under the supervision of trained staff at the time of surgery. We think that access for PCNL is a valuable tool that should be in the armamentarium of all urologic surgeons on leaving an accredited urology training program.
Introduction
Despite the numerous practical applications and indications for percutaneous renal access, many urologists do not obtain their own access. Often, reliance is placed on the local interventional radiologist (IR) when considering access for PCNL or other antegrade renal procedures. This is performed as a joint procedure in the operating room between IR and urology or as a staged procedure, with access gained before PCNL. 3
We report our experience with urology residents obtaining access for PCNL under the supervision of nine staff physicians. Albeit, the majority were obtained under the supervision of a single staff physician. Moreover, we compare success and complication rates to those put forth by the American College of Radiology (ACR). 4,5
We also surveyed graduating chief residents at all accredited United States urology programs regarding their experience with PCNL access as well as their plans to obtain percutaneous access post-training.
Patients and Methods
A retrospective chart review was performed of all patients undergoing PCNL at our institution from 1995 to 2009. Patients were excluded if access was gained elsewhere, before the time of surgery, or if access was not attempted by the resident at the time of surgery. The 290 PCNLs resulting in 338 separate access obtainments were equally distributed throughout the study time frame. All patients underwent preoperative evaluation with history and physical examination, complete blood cell count, basic metabolic panel, and determination of serum calcium and uric acid. Each radiologic evaluation was patient specific and included plain film radiography, intravenous urography, ultrasonography, as well as CT scan. In addition, all patients submitted a 24-hour urine collection to aid in identification and treatment of metabolic risk factors for stone formation.
All patients underwent induction of general anesthesia and were placed in the dorsal lithotomy position. Under fluoroscopic guidance, a 5F Pollack catheter was directed into the collecting system to be punctured, preferably in the upper pole. At this point, the patients were taken out of the dorsal lithotomy position and transferred to the prone position. Using the triangulation technique and C-arm fluoroscopy, the desired calix was located with the aid of radioopaque contrast injected through the previously placed 5F catheter. The desired calix was then punctured using an 18-gauge needle with stylet (Fig. 1). The desired calix was accessed within two skin punctures. Only 5% of the time was access unsatisfactorily gained, necessitating a secondary access.

Intraoperative photo illustrating obtainment of percutaneous access.
Access was gained using a combination of J guidewires as well as straight and angle-tipped hydrophilic glidewires where appropriate. When possible, access was secured with two wires directed down the ureter and into the bladder. A 30F working sheath was then routinely placed after dilation of the tract with a NephroMax™ balloon. Appropriate stone removal surgery was then performed, and at the end of the case, a 20F reentry Malecophy nephrostomy tube was placed if indicated. Nephrostogram confirmed placement, and a sterile dressing was applied after securing the nephrostomy tube.
Postoperative chest radiography was performed on all patients to rule out pneumothorax or hydrothorax. Postoperative CT scans were not obtained on a routine basis. The need for postoperative imaging was highly individualized based on the preoperative stone burden and success of stone clearance during PCNL. Notably, we did not consistently record fluoroscopic time, and therefore it has not been included as a variable. This may be an important component to include prospectively in our database.
Success rates related to access and complications in our series were compared with those set forth by the ACR for performance of PCNL, as shown in Table 1.
Regarding the survey, an eight-item questionnaire was sent by e-mail to all chief residents at accredited United States urology training programs. The questions covered residents' experience with obtaining access for PCNL during training as well as plans for access after graduation. All responses were anonymous.
Results
Charts were identified by Current Procedural Terminology code search for PCNL both under and over 2-cm stone burden. Charts were evaluated for 290 patients with 338 separate access sites performed under the supervision of nine different staff. Access was gained by residents operating in the role of primary surgeon at the time of surgery in all cases reviewed. This means faculty was acting purely as a second assistant in the operating room. If the resident had difficulty obtaining access, the faculty would intervene.
Major complications included bleeding necessitating transfusion, sepsis, pseudoaneurysm, hydrothorax, pneumothorax, ureteropelvic junction (UPJ) disruption, and death. Minor complications included urinary tract infection and collecting system injury that necessitated prolonged stent placement. We noted a total of 40 complications: 29 major and 11 minor. Hemorrhage necessitating transfusion was the most common at 5.9%. A postoperative hemoglobin level of 7.5 was used as transfusion criteria. Sepsis, UPJ disruption, pneumothorax, and hydrothorax were all treated by the urology team successfully. Broad-spectrum antibiotics and supportive care were instituted for treatment of postoperative urosepsis. The single patient with a UPJ disruption underwent a successful reconstructive procedure at a later point. All patients with pneumothorax or hydrothorax were treated with chest tubes placed by the primary service. Two patients with arteriovenous fistula were treated with angioembolization, and one death was noted from postoperative pulmonary embolus. Minor complications were also treated by the primary team. Compared with complications put forth by the ACR (Table 2), our complications compared very favorably (Table 3).
PCNL=percutaneous nephrolithotomy.
UPJ=ureteropelvic junction; UTI=urinary tract infection.
Our survey of urology chief residents showed that while only 47% of respondents noted that access was routinely gained at their institution by urologists, 94% felt that learning access would be a valuable tool. In addition, 90% of participants plan to perform PCNL on graduation, but only 43% planned to gain their own access at that time.
Discussion
Percutaneous renal access has a multitude of applications, including but not limited to management of infectious processes, relief of obstruction, treatment of malignancy, and stone surgery. In addition, PCNL has become a mainstay for the treatment of patients with large stone burdens. Ureteroscopic stone extraction has remained the mainstay for smaller <1 cm) stones, especially those that are distal or not visible on radiography of the kidneys, ureters, and bladder. Nonetheless, recent articles have begun to compare ureteroscopic stone extraction for the management of large stone burden or staghorn calculi. 6,7 Shockwave lithotripsy also revolutionized treatment of patients with stone disease by providing a noninvasive therapeutic modality for calculi, but PCNL is still the treatment of choice for renal calculi over 2 cm or staghorn calculi. 8
In our study, we examined more than 300 PCNLs in which access was obtained by postgraduate year (PGY) 4 and PGY 5 urology residents under the supervision of nine attending surgeons at our teaching institution. Although nine different attending surgeons are included in the data set, a single surgeon supervised 314 of the 338 access cases reviewed. Success was described as access secured within the collecting system at the beginning of every PCNL procedure. The PGY 4 or PGY 5 residents, under close staff supervision, were able to access all renal units in our study at the time of PCNL. Complications overall were minimal and well within the range of those noted in other series. Notably, on two or three occasions, the procedure was terminated before complete stone removal because of poor visibility attributed to bleeding or return of grossly infected urine. Complications such as hemorrhage or UPJ disruption were more likely from the stone surgery itself rather than obtainment of access.
Because our complication rates remained low and comparable with ACR data, there are several advantages to obtaining access to the kidney at the time of surgery. For example, if the preoperatively selected site of access appears suboptimal at the time of puncture, this can easily be modified according to surgeon preference. In addition, if the access is suboptimal once gained, or if there are persistent areas of stone unreachable from a single access site, it is a small matter for the trained urologist to select another calix or do multiple punctures to increase the rate of stone clearance (Fig. 2).
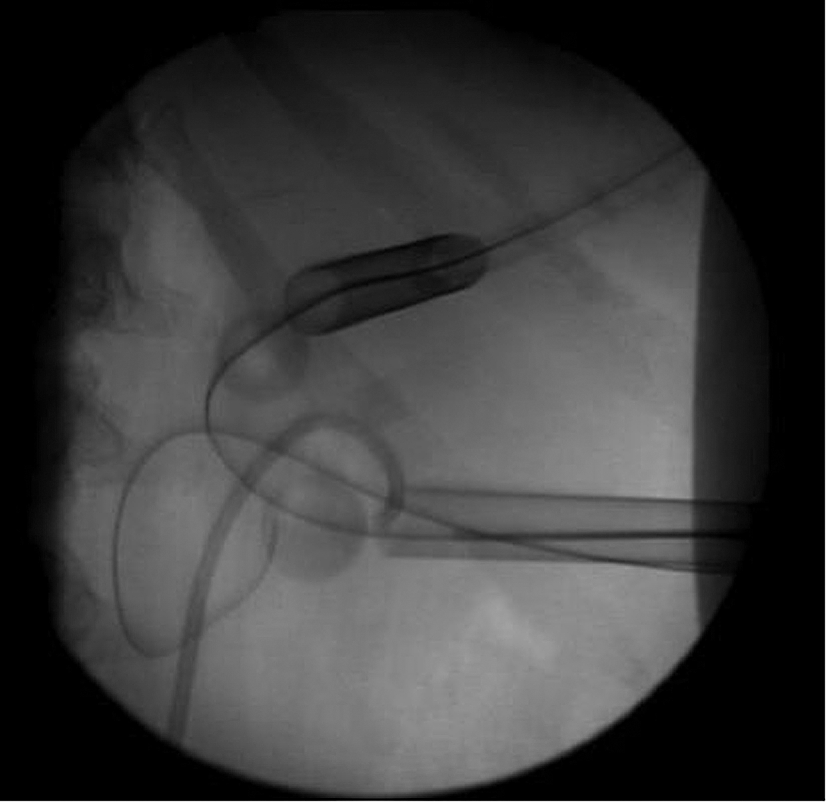
Intraoperative flouroscopy.
Finally, it is also worth noting that at our institution, we are referred many patients with difficult anatomy, severe stone disease, solitary kidneys, spinal deformities as well as those who are morbidly obese (Fig. 3). We have found it a rare circumstance in which access is unable to be obtained from below necessitating emergent percutaneous nephrostomy tube placement for urgent decompression. That being said, in our institution, we have the unique experience of performing percutaneous nephrostomy tube placement in these situations as well because the IRs defer to urology in these instances. Certainly, it is fair to conclude that the residents at our institution may have an accelerated learning curve because of this unique experience.

Sample of challenging patient with morbid obesity.
The safety and efficacy of percutaneous renal access is fairly well established, and the high success rate as well as relatively low rate of complications has allowed this procedure to gain widespread popularity. El-Assmy and colleagues 9 reviewed more than 2000 percutaneous renal access cases for the purpose of PCNL comparing nearly equal groups with access gained by either urology or radiology. They found similar complication rates except for significant bleeding in the urology group. Rana and coworkers 10 reported a 97% success rate when placing percutaneous nephrostomy tubes in 765 procedures. This was performed by three staff physicians who were trained by IRs. Watterson and associates 11 compared complications and stone-free rates when access was gained by a group of five IRs or by a single urologist and found favorable outcomes when access was gained by the urologist. In regard to this, when the patient does have a complication from gaining access, a urology service is more likely to admit and provide care to the patient. Often, IR does not admit patients to their service and inevitably, urology services assume the role of the providing physician.
De la Rosette and colleagues, 12 who performed a critical review regarding training in PCNL, discussed the steep learning curve that is involved in becoming proficient, stating that a resident must perform about 24 PCNLs before becoming adept. 12 The University of Iowa sent out a survey to all practicing members of the North Central Section of the American Urological Association concerning practice patterns with regard to large renal stones. They showed that only 11% of practicing urologists routinely gained their own access for PCNL. 3 Another study from the University of Minnesota surveyed residents who had graduated from that program and were in practice. All residents had been instructed in PCNL access, but only 27% of these surgeons continued to gain access. 13 Although the response rate to our resident survey was somewhat low at 30%, it was still fairly telling that 94% of graduating chief residents thought that access for PCNL would be a valuable skill to learn during training. Certainly, it would be appropriate to poll our own graduates to see if they continue to obtain their own access for PCNL in their respective practices.
With a well-documented shortage of health care providers looming and a burgeoning elderly population around the corner, it is unrealistic to assume that every urologist in the country will have access to an IR. Moreover, in many underserved rural areas, there is not an IR available, necessitating transfer of the patient to an already strained tertiary center.
A notable criticism of our study is its retrospective design. A control group in which access was performed by an IR would also be helpful, but would be difficult to fairly compare because all access for PCNL at our institution has been obtained by the urology service for the past 20 years. Another possible area of concern is that multiple staff taught residents different techniques for access and would subject the data to variability in regard to complication rates. The vast majority of cases, however, were staffed by a single physician (314 of the 338 cases reviewed) using the same technique from study start to finish. Moreover, our excellent success rate and low complications only strengthen the premise that this is a skill that can be successfully taught to residents with good reproducibility in a teaching institution under close supervision. Finally, as previously noted, complications such as hemorrhage necessitating transfusion were likely because of the stone removal portion of the case rather than gaining access.
In light of today's rapidly advancing technology and varied treatment alternatives, it is important for the urologist to remain at the forefront of all aspects of patient care. Reliance on other services to provide aspects of urologic care is a slippery slope that becomes dangerous as more and more treatment options progress to less invasive therapies. With the advent of percutaneous renal ablative therapies, it becomes all the more imperative to be independent in our treatment decisions and options because radiologists are usually involved if not in charge of these procedures.
Conclusion
PCNL can be safely and successfully obtained by urology residents under the supervision of trained staff at the time of surgery, with minimal complications and excellent success rates. A teaching institution provides the ideal setting in which to instruct the urology resident in this valuable skill. To maximize patient care and success in the operating room, access for PCNL should be taught to all residents before graduation.
Footnotes
Disclosure Statement
No competing financial interests exist.