
Abstract
Purpose:
Our objective was to design an intranet-based database to streamline stone patient management and data collection.
Materials and Methods:
The system developers used a rapid development approach that removed the need for laborious and unnecessary documentation, instead focusing on producing a rapid prototype that could then be altered iteratively. By using open source development software and website best practice, the development cost was kept very low in comparison with traditional clinical applications. Information about each patient episode can be entered via a user-friendly interface.
Results:
The bespoke electronic stone database removes the need for handwritten notes, dictation, and typing. From the database, files may be automatically generated for clinic letters, operation notes. and letters to family doctors. These may be printed or e-mailed from the database. Data may be easily exported for audits, coding, and research.
Conclusions:
Data collection remains central to medical practice, to improve patient safety, to analyze medical and surgical outcomes, and to evaluate emerging treatments. Establishing prospective data collection is crucial to this process. In the current era, we have the opportunity to embrace available technology to facilitate this process. The database template could be modified for use in other clinics. The database that we have designed helps to provide a modern and efficient clinical stone service.
Introduction
Clinical audit is an essential requirement of clinical governance for healthcare professionals, and good data collection is a vital component of this process. Local, national, and international professional bodies are increasingly keen to evaluate new surgical techniques and audit established procedures. Clinical research relies on comprehensive data collection of defined parameters, and translational basic science research needs accurate demographic, procedure, and outcome data to link with biologic sample analysis. When clinical data are not collected in a template-based system, subsequent data mining for audit and research is laborious and often incomplete. By evaluating complete, prospectively collected datasets, decisions on best practice can be made, and patients may be stratified by phenotype to identify cohorts for targeted research projects.
Most international healthcare systems have a methods of accountability, and a physician-led system is the most accurate way to record volumes of activity and their outcomes. Collecting this prospective data will become increasingly important to meet the demands of health economics. Some centers have moved to electronic patient records to reduce administrative paperwork, and a few centers are now paper free. These systems, however, are expensive, often generic, and not yet widely adopted.
A bespoke electronic stone clinic offers the possibility both to reduce administration and provide a prospectively collected, organized dataset on stone patients for research and audit purposes. We describe how we have developed a stone database for our center that could readily be extended to other stone centers and into other areas of urologic or medical practice.
Materials and Methods
After a series of workshops and sessions between system developers and clinical users, wireframes were constructed to blueprint how the stone database would function, its processes, and appearance. A key consideration was the creation of a clinically intuitive, user-friendly "front end" for the clinician to minimize the inconvenience of moving to an electronic system. The system developers used a rapid development approach that removed the need for laborious and unnecessary documentation, instead focusing on producing a rapid prototype that could then be altered iteratively. The system was constructed with a combination of open-source content management system (Joomla) and structured query language.
Results
Security
Most electronic patient data in the United Kingdom is stored on the N3 network. 5 N3 is the National Health Service national broadband network linking hospitals, medical centers, and general practitioners in England and Scotland. Our database is password protected and hosted locally on an N3 virtual server. Password protected systems hosted on local intranets should offer similar levels of acceptable security (Fig. 1). Care must be taken when data are trafficked electronically to ensure identifiable and sensitive information is not accessible to a third party. Encryption of data must meet national guidelines.
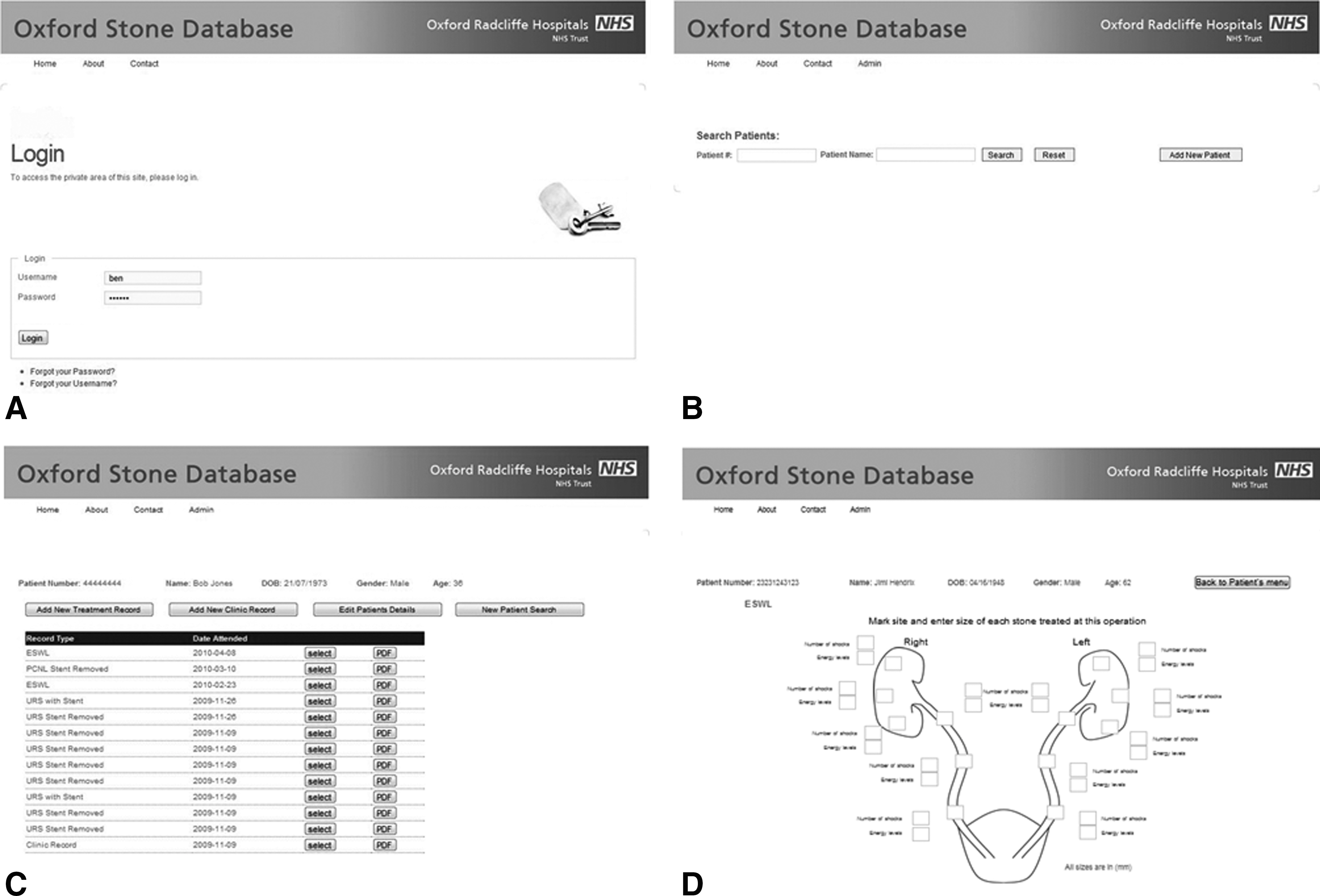
Screen shots from the database.
Accessibility
Some databases are hosted only on one computer; this creates problems of accessibility, restricting access to one person at a time and in one location. Our web-based system is available on any computer connected to the hospital intranet. Therefore, patient stone episodes can be created, reviewed, e-mailed, or printed from the clinic, ward, or operating room (Fig. 1).
Efficiency
The stone database offers the ability to remove the need for handwritten notes, dictation, and typing for stone procedures and outpatient clinic attendances. From the database, report files may be automatically generated for clinic letters, operation notes, and letters to family doctors (Fig. 2). These may be printed or e-mailed as needed. This generates several clear efficiency savings: The patient's stone history is immediately accessible in the clinic; no writing or dictation or typing is necessary; the patient can receive a consultation summary on departure; and reports can be communicated electronically.

Example of database outputs.
Data integration
Once the central stone database is created, it can be linked with other electronic resources locally, including patient demographics and clinical laboratory results (Fig. 3). This means that some data fields are populated automatically to improve efficiency and accuracy of data collection. Systems could potentially be connected to other systems, including radiology data, outpatient clinic appointment diaries, and operating lists. Other data could be incorporated from electronic patient surveys of factors such as diet and lifestyle.

Cartoon to highlight the interactions of the stone database. Data entered in the stone clinic can be augmented from data in other hospital databases (eg, laboratory results, patient demographics) before producing formatted letters, operation notes, and procedure summaries. Data may also be linked to independent data such as a biobank of clinical samples.
Clinic template
The stone database forms a template that can be modified for use in other clinic settings. Such systems would be particularly useful when patients are followed up multiple times biochemically, radiologically, or with an intervention such as a biopsy or endoscopy. Management of other urologic conditions (prostate cancer, bladder cancer, and renal cancer) readily meet these criteria.
Data mining
The large volumes of data that quickly accumulate can be mined to examine subgroups by phenotype or intervention. This provides a powerful tool for clinical research and also allows stratification of patients for translational basic science research.
Discussion
Electronic methods of data storage and communication (e-mail, electronic calendars, etc.) are ubiquitous and have been adopted by most doctors in their personal lives. Medical practice, however, generally lags behind other sectors in adopting this technology. An electronic clinical database can improve the efficiency of clinical practice, be cost effective, and provide the benefits of a custom-made solution to gather, store, and output data.
To improve patient safety, treatment, and evaluation of new technologies, representative datasets containing large numbers of patients are essential. Unfortunately, data collection for audit and research is usually an additional burden to clinical practice, yet much of the required data is collected more than once in different settings. An electronic clinical database removes the duplication of work by linking with existing systems to increase administrative efficiency and collate the data simultaneously. To encourage compliance with data collection, the system must be logical and user-friendly. This necessitates input from clinicians who are familiar with the relevant field of medicine.
Once the framework for a database is created, it forms a template for creating similar systems for other areas of urologic and medical practice. Bespoke systems designed in collaboration with clinicians promote relevant data collection via a user-friendly and intuitive interface. The system we have designed reflects practice in our institution. While it should be possible to modify the current system to meet the demands of other institutions, this has not yet been tested.
From the basic framework, there are multiple means of enhancing the system. For example, links to local/national/international guidelines, consent forms, patient information leaflets, nomograms, and risk tables could be readily incorporated.
Conclusions
Data collection remains central to medical practice, to improve patient safety, to analyze medical and surgical outcomes, and to evaluate emerging treatments. Establishing prospective data collection is crucial to this process. In the current era, we have the opportunity to embrace available technology to facilitate this process. For these systems to work, it necessitates input from clinicians to help design systems to collect appropriate information. The database template could be modified for use in other clinics. The database that we have designed helps to provide a modern and efficient clinical stone service.
Footnotes
Acknowledgments
IconZest and Levita were the information technology companies involved in developing this system. This project was funded by charitable donations from the Oxford Urology Foundation.
Disclosure Statement
No competing financial interests exist.