
Abstract
Background and Purpose:
Urinary incontinence is a significant cause of morbidity after robot-assisted radical prostatectomy (RARP). Several techniques have been developed to improve continence rates. In this study, we compared the continence rates of patients who underwent RARP with total reconstruction and without reconstruction.
Patients and Methods:
Between March 2005 and September 2009, 245 patients underwent RARP at our institution. The initial 120 patients (control group) underwent standard RARP without reconstruction and the last 125 patients (reconstruction group) underwent a total reconstruction technique, which included an anterior and posterior reconstruction. Patients were followed for 1, 4, 12, 24, 36, and 52 weeks after the operation. Continence was defined with strict criteria—no usage of pads and no leakage of urine.
Results:
In the reconstruction group, the continence rates at, 1, 4, 12, 24, 36, and 52 weeks postoperatively were 71%, 72%, 80%, 84%, 86%, and 91%, respectively; in the control group, the continence rates were 23%, 49%, 76%, 80%, 85%, and 88%, respectively.
Conclusion:
The overall continence rates were similar in both groups at 52 weeks of follow-up. Patients in the total reconstruction group, however, had higher early continence rates compared with patients in the control group. The total reconstruction procedure is an efficient way to achieve an early return to continence.
Introduction
The continence rates of RARP typically reach satisfactory levels at 1 year after the procedure, and early continence rates are very low in most of the published series. 2,3
Patients' demands are to not only be completely continent but to also have an earlier return of continence. For this reason, several technical modifications have been developed to improve early continence rates. Some of these methods are: Achieving maximum length of urethra after surgery; preservation of puboprostatic ligaments and bladder neck; suspension operations; anterior reconstruction; and posterior reconstruction techniques. 4
In this study, we evaluated the continence rates of patients who underwent RARP with anterior and posterior reconstruction and compared them with patients without reconstruction.
Patients and Methods
Between March 2005 and September 2009, 245 patients underwent RARP at our institution. The initial 120 patients (control group) underwent standard RARP without reconstruction and the last 125 patients (reconstruction group) underwent a total reconstruction technique, which included an anterior and posterior reconstruction. The same surgical team performed all operations. Patients were followed for 1, 4, 12, 24, 36, and 52 weeks after the procedure. Continence was defined with strict criteria—no use of pads accepted as continent.
Patients with diabetes and neurologic diseases, previous pelvic operations, or simply those with symptoms of urinary incontinence before radical retropublic prostatectomy (RRP) were excluded from the study. Two patients in the first group (one diabetes and one neurologic disease) and three patients in the second group (one neurologic disease, one diabetes, and one patient with urge incontinence before the operation) were excluded from the study.
Surgical technique
Our technique has been described previously. 3 All cases were performed with a six-port technique via the transperitoneal route. The anterior abdominal wall was dropped down and the retropubic space was entered; then the endopelvic fascia was opened on both sides and levator ani muscles were pushed away from the prostate. The dorsal vein complex (DVC) was ligated using a 2/0 polyglactin suture with sliding knot technique. The anterior reconstruction and posterior reconstruction techniques are performed as follows;
Anterior reconstruction
After ligating the DVC, the same suture was passed through the periosteum of the symphisis pubis. The suture was ligated to symphysis pubis with sliding knot technique, and only mild tension was applied to the suture. In our technique, we performed only a single layer of suspension in all of our operations. After anterior reconstruction, the bladder neck was divided, seminal vesicles were dissected, and nerve sparing was performed when indicated.
Posterior reconstruction
Posterior reconstruction was performed by a single 2/0 polyglactin suture on a UR-6 needle. The suture was placed between the urethral stump and the bladder neck. First the suture was placed posterior and proximal to the urethral stump and then passed through the posterior musculofascial plate; finally, the suture was placed posterior to the bladder neck. To easily tighten the suture, a sliding knot was used, and perineal pressure was applied when needed. Because the rationale for this maneuver is to recreate the previous continuity of the Denonvillier fascia and the posterior rhabdosphincter, a single suture was enough. After completing posterior reconstruction, urethrovesical anastomosis was performed using two 20-cm 2/0 Biosyn™ sutures—one dyed and the other undyed—with Van Velthoven technique. First, the posterior side of the anastomosis was created, and then both sides of the anastomosis were completed—one side in clockwise and one side in counterclockwise direction. Sutures were tied at the 12 o'clock position. A Jackson Pratt drain was placed around the anastomosis.
Cystography was performed on the seventh postoperative day. If no significant leak was detected, the urethral catheter was removed and a trial of void was conducted. We defined continence as 0 pads or 1 dry pad for reassurance. Any involuntary urine loss or pad use was defined as incontinent. Patients were followed and interviewed by the same physician at 1, 4, 12, 24, 36, and 52 weeks postoperatively.
Statistical analysis
Descriptive results such as median, interquartile range, and percentage were reported for all studied variables. A nonparametric method, Wilcoxon T-test, was used at the 5% level of significance to compare median values of age, prostate-specific antigen (PSA), free PSA (fPSA), prostate volume, Gleason score, operative time, blood loss, body mass index, final pathology result Gleason score, hospitalization time, and catheter removal among the with and without anterior/posterior reconstruction groups. To test the homogeneity for surgical margin stages, pathologic stages, and nerve sparing, we also performed the chi-square test for two groups. The Fisher exact test and chi-square test at the 5% significance level were used to compare the continence rates of control and reconstruction groups. Finally, univariate and multivariate models for early return to continence were developed that used logistic and multiple logistic regression analysis using backward regression procedure. All statistical analysis tests were performed with the Statistical Analysis Software 9.2 (SAS Institute, Cary, NC).
Results
The patient demographics, operative parameters, and pathologic data are given in Tables 1 and 2. The parameters that may affect urinary continence, such as age, body mass index (BMI), nerve sparing, catheterization time, prostate volume, and pathologic data were comparable in both groups of patients. Operative time, blood loss, and hospital stay, however, were significantly shorter in the second group (P<0.05) (Table 1).
Denotes the two groups are statistically different at 5% level of significance.
AP=anterior/posterior; IQR=interquartile range; PSA=prostate-specific antigen; fPSA=free prostate-specific antigen; Bx=biopsy; EBL=estimated blood loss; BMI=body mass index.
Denotes the two groups are statistically different at 5% level of significance.
AP=anterior/posterior; IQR=interquartile range.
In the first group, 77% of patients underwent a bilateral nerve-sparing procedure, 18% underwent a unilateral nerve-sparing procedure, and 4% a non–nerve-sparing procedure. In the second group, 71% of patients underwent a bilateral nerve-sparing procedure, 16% underwent a unilateral nerve-sparing procedure, and 12% underwent a non–nerve-sparing procedure. There was no statistically significant difference between both groups, and the nerve-sparing procedure was performed in equal numbers in both groups (Table 1). The two groups had no significant differences regarding the pathologic stage, positive surgical margin rate (PSM), and final pathology result Gleason score. The overall PSM rates were 8.3% and 8% in the first and second groups, respectively (Table 2).
The continence rates of the whole study group are given in Table 3. Continence rates of the initial 120 patients (control group) and the last 125 patients (reconstruction group) were 23%, 49%, 76%, 80%, 85%, 88% and 71%, 72%, 80%, 84%, 86%, and 91% at 1, 4, 12, 24, 36, and 52 weeks of follow-up, respectively.
Denotes the two groups are statistically different.
AP=anterior/posterior.
Table 4 gives the univariate analysis and multivariate backward logistic regression analysis results for the outcome variable APR (without/with) to see other factors such as age, PSA, fPSA, prostate volume, Gleason score, operative time, blood loss, BMI, final pathology result Gleason score, hospitalization time, and catheter removal and pathologic data that might affect the early return of continence. In multivariate analysis, operative time and hospitalization time are selected in the final model. The adjusted odds ratios of APR (without) vs APR (with) for operative time and hospitalization time are 1.009 and 2.069, respectively; ie, the odds are significantly higher for the first group.
P value: Univariate analysis and amultivariate analysis using backward elimination method.
OR=odds ratio; BMI=body mass index; PSA=prostate-specific antigen; fPSA=free prostate-specific antigen; PV=prostate volume; GS=Gleason score; OP=operative; EBL=estimated blood loss; FPG=final pathology Gleason; hosp=hospitalization; CR=catheter removal; NS=nerve sparing; PS=pathologic stage; SM=surgical margin.
Discussion
One of the most important complications of radical prostatectomy (RP) is urinary incontinence with an incidence ranging from 1% to 67% in contemporary series. 5,6 The long- term continence rates are quite good; however, early continence rates are still low in most of the published series. 7 –12 Prolonged incontinence deteriorates the patients life quality and creates a dissatisfaction in a majority of patients after RP. For these reasons, multiple techniques were developed in RARP to achieve continence earlier.
In 2006, Rocco and associates 13 first published results of reconstruction of the posterior aspect of the rhabdosphincter in open RP. In this study, they modified Walsh's technique by reconstructing the musculofascial plate and restoring the connections of the residual Dennonvilliers fascia to the posterior wall of the rhabdosphincter. The authors reported 72%, 78.8%, and 86.3% continence rates in the posterior reconstruction group at 3, 30, and 90 days whereas the numbers were 14%, 30%, and 46% in the historical control group.
The feasibility of their technique in open, laparoscopic, and robot-assisted operations has been reported by several studies. 14,15 The applicability of this technique has been shown in laparoscopic radical prostatectomy (LRP) operations by Rocco and colleagues. 15 In a study, the authors evaluated the posterior reconstruction technique in 31 LRP operations and compared them with 31 patients who underwent standard LRP operation. At catheter removal, 74.2% of patients were continent in the reconstruction group whereas only 25% of patients were continent in the nonreconstruction group.
Moreover, the effectiveness of the posterior reconstruction technique has been shown in robotic operations. In 2008, Coughlin and coworkers 16 described a posterior reconstruction technique in RARP. In their technique, posterior reconstruction was performed in two layers by using a continuous suture of two 3/0 poliglecaprone sutures of different colors that were tied together. They reported 58% (defined by the use of no pad) or 72% (0 or 1 pad per day) continence rate at 1 week. In another study, Nguyen and associates 17 evaluated posterior musculofascial reconstruction in a mixed group of patients undergoing laparoscopic and RARP. They compared 32 consecutive patients having robot-assisted or laparoscopic RP with reconstruction to 30 historical controls without reconstruction. At 3 days and 6 weeks after catheter removal, continence rates were better in the reconstruction group. Moreover, they measured the mean length of membranous urethra before and after the operation and they reported that posterior reconstruction reestablished the length of membranous urethra by a mean of 2 mm. Finally, they concluded that posterior reconstruction technique leads to an increased membranous urethral length and significantly higher early continence rates.
Different suspension techniques have been developed to improve continence results in RP. In 2001, Sugimura and colleagues 6 described an anterior urethral stitch technique in open RP. In this study, a 2/0 polyglactin suture was placed in the levator ani musculature between the cut edges of the lateral pelvic fascia and then the suture was firmly tied parallel to the urethra. The authors postulated that the anterior urethral suture might result in rising and narrowing of the urethra, thus possibly supporting the sphincter. As a result, they reported a shorter time for continence recovery (median 8.5 days) in the suspension group when compared with the historical control group (median 72 days).
In another study, Noguchi and coworkers 18 evaluated the urodynamic findings after RP in 33 patients in whom suspension was performed and compared them with 12 nonsuspension patients. Postoperatively, the continence rates and abdominal leak point pressures were significantly higher in the suspension group.
In 2009, Patel and colleagues 3 reported the anterior reconstruction technique in RARP. In this study, they applied the suspension stitch in 237 patients and compared them with 94 patients without suspension stitch. The continence rates were higher in the suspension group at 1, 3, 6, and 12 months; however, the difference between the two groups was only statistically significant at 3 months postoperatively.
Anterior reconstruction technique can be performed separately or in a combined style with posterior construction (total reconstruction). In 2008, Tewari and associates 10 reported their experience of total reconstruction technique in RARP patients. In this study, 182 patients underwent an extensive total reconstruction, 304 patients underwent anterior reconstruction, and 214 patients underwent standard anastomosis and served as the control group. At 1, 6, 12, 24, and 52 weeks of follow-up, the continence rates were significantly higher in the total reconstruction and anterior reconstruction groups than the control group.
In another study, Koliakos and coworkers 19 reported their results in a prospective study. Twenty-three patients were randomized to total reconstruction group and 24 patients randomized to standard anastomosis. At catheter removal and 7 weeks, 39% and 65% of the patients were continent in the total reconstruction group whereas only 12.5% and 33% of the patients were continent in the control group.
In our study, we compared the continence rates of patients who were undergoing RARP with posterior and anterior reconstruction to a group without reconstruction. In contrast to previous studies with anterior and/or posterior repairs that necessitate extensive reconstruction and multiple sutures, we used a simplified technique using a single stitch, which is easier to perform and saves time. Unlike the Rocco or Tewari techniques, an extensive repair was not performed. According to the original technique, posterior reconstruction is applied with running sutures in a multilayer fashion. On this point, our study differs from the previous studies with performing the posterior repair with a single suture and in one layer fashion (Figs. 1 and 2).
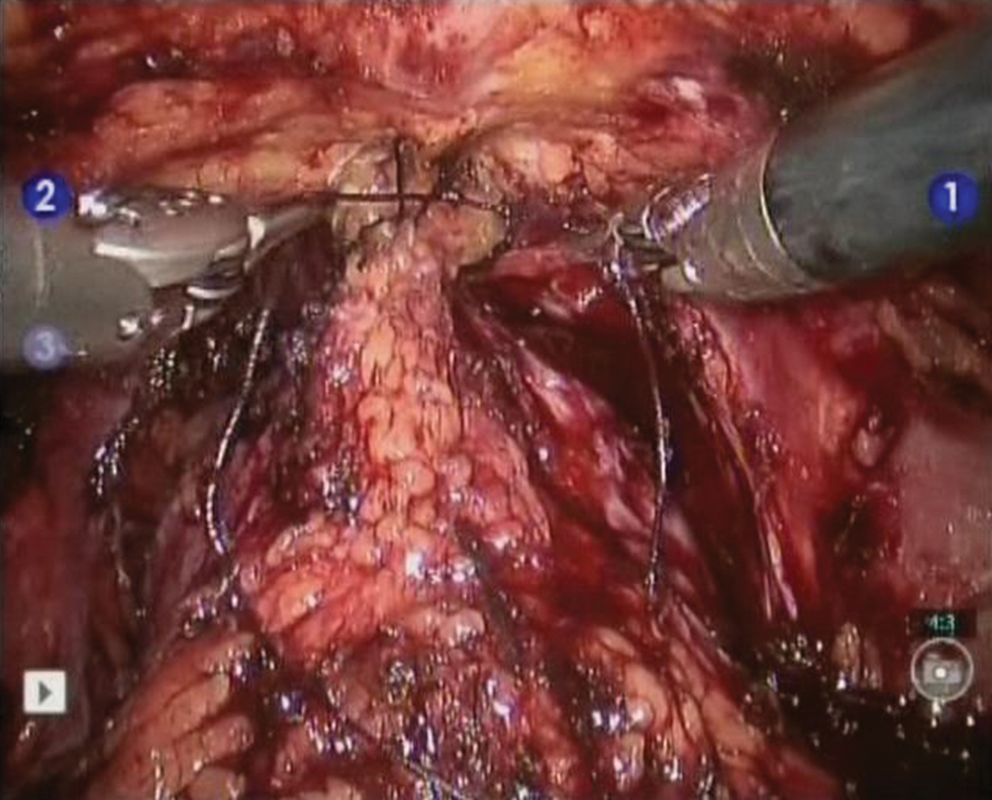
Anterior reconstruction.
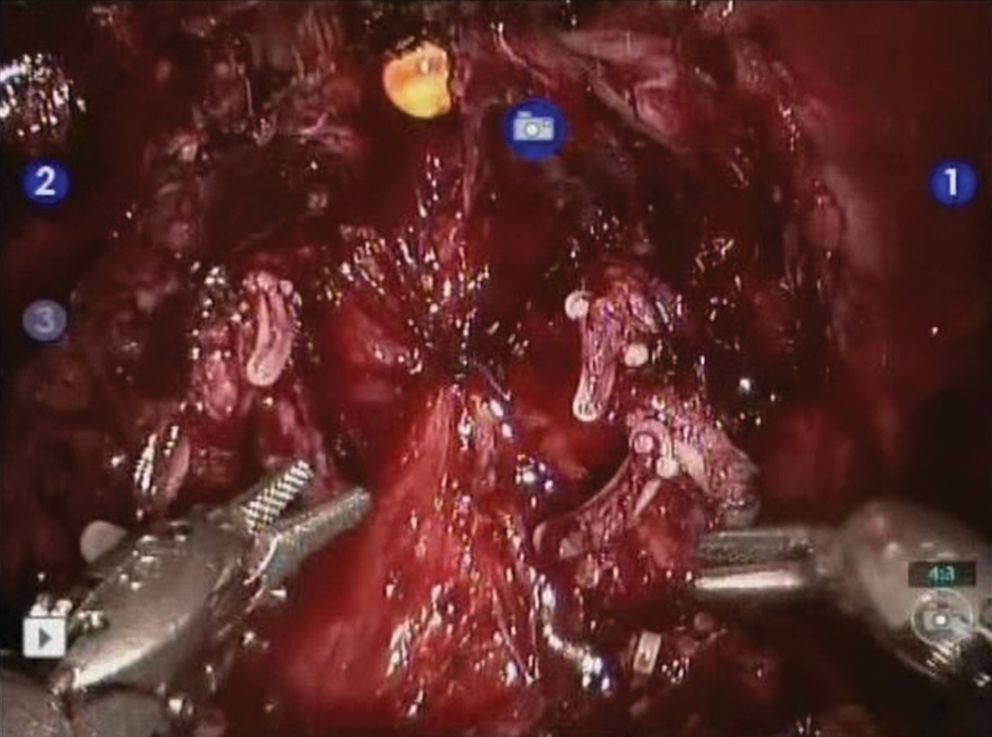
Posterior reconstruction.
Sammon and colleagues 20 recently published their long-term results that compare single- vs double-layer anastomosis during RARP in 116 consecutive patients. At 2 years of follow-up, 96% and 100% of patients were continent (0–1 pad daily) in single- and double-layer anastomosis groups, respectively. On the other hand, pad-free rates (defined by the use of no pad) were 80% and 82%, respectively. As a result, the authors found no significant difference in continence rates between single- vs double-layer anastomosis.
Our technique also does not necessitate multiple interrupted or continuous sutures to reestablish the posterior urethra. This eliminates the multiple knots, which makes it easier and uncomplicated and therefore quicker and easily applicable by less experienced surgeons when compared with previously described techniques.
In this study, we also examined the factors that might affect the urinary incontinence status of our patients. Patients with diabetes and neurologic diseases, previous pelvic operations, or simply those with symptoms of urinary incontinence before RRP were excluded from the study. In addition to the use of reconstruction techniques, final urinary continence depends on several other factors, such as patient age, BMI, bladder function, prostate size, pathologic stage, and neurovascular bundle preservation. There was no statistical difference between the groups with regard to patient age, BMI, PSA level, prostate volume, Gleason score, catheterization time, and nerve-sparing status (Table 2).
Operative time, blood loss, and hospital stay were significantly shorter in the reconstruction group. We believe that this difference is a result of the learning curve. As expected, the operative times will decrease as the number of cases increases.
Our study showed that patients receiving anterior and posterior reconstruction achieved continence earlier than those patients who did not receive any reconstruction. The differences between the two groups were quite significant until the 12th week (Table 3). The long-term results, however, were similar with no statistical difference; 88% and 91% of the patients were continent in groups 1 and 2, respectively, at 1-year follow-up (Fig. 3).
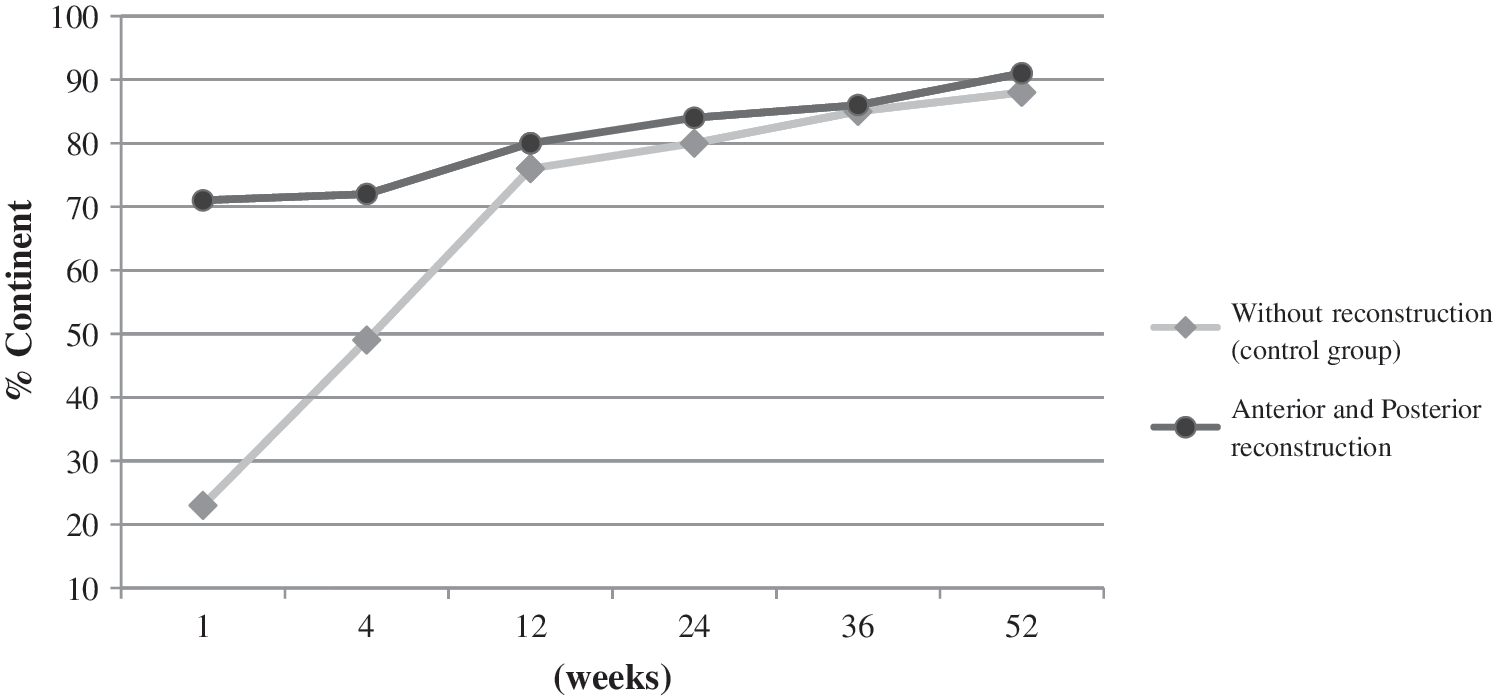
Continence rates at 1-year follow-up.
Conclusion
The overall continence rates were similar in both groups at 52 weeks of follow-up. Patients in the total reconstruction group, however, had higher early continence rates than patients in the control group. The total reconstruction procedure is an effective and safe technique for the early return of urinary continence after RARP. Early return of continence might increase patient satisfaction after RARP operations.
Footnotes
Disclosure Statement
No competing financial interests exist.