
Abstract
Background and Purpose:
Oral citrate supplements have been shown to decrease kidney stone recurrence rates in both laboratory and clinical studies. The taste of the citrate supplements, however, is poor, and long-term compliance is low. Our objective was to determine if Splenda® added to potassium citrate (KCit) improves palatability without changing 24-hour urine parameters.
Patients and Methods:
12 subjects were randomly assigned to receive either KCit alone for 3 days or KCit + Splenda in a double-blind trial. The 24-hour urine collections were performed before and after 3 days of therapy. After 1 week, the two groups switched treatments. After each treatment, a visual analog taste scale was completed to gauge the taste and palatability. The 24-hour urine parameters of kidney stone risk factors were compared between groups. The primary end points were to determine whether Splenda improved palatability of citrate supplementation and whether it altered 24-hour urine parameters.
Results:
Taste was judged to be 2.5±0.9 points better in the Splenda + KCit compared with KCit alone (P=0.02). The 24-hour Cit, K, and pH were significantly higher in the KCit and KCit + Splenda groups compared with baseline, but not significantly different from each other.
Conclusion:
Splenda significantly improves the palatability of KCit therapy and does not alter the beneficial effects of KCit on 24-hour urine Cit, K, or pH. The addition of Splenda altered the average taste score from one that might prohibit compliance to one that would not.
Introduction
Recurrence is common and is found in 50% within 10 years of initial presentation for first- time stone formers, with calcium oxalate making up the majority of stones formed. 3 –5 Many times dietary modification and high fluid intake are not enough, and repeated surgical intervention and acute stone events warrant more aggressive medical preventative treatment. A meta-analysis of randomized medical trials showed a 22.6% risk reduction in recurrence rates with initiation of drug and dietary treatment. 6 One health care cost analysis suggested that medical prevention is of benefit if the expected stone recurrence rates are greater than 0.3 per year. 7
Medical treatment with potassium citrate (KCit) therapy has been shown to significantly decrease recurrence rates in calcium oxalate and uric acid nephrolithiasis. 8 KCit works by increasing urinary Cit (a natural inhibitor) and alkalizing the urine. 9 At a pH <5.5, the undissociated form of uric acid predominates, promoting both uric acid and calcium oxalate stone formation. 10 Calcium oxalate stones form in low pH as a result of heterogeneous nucleation on uric acid crystals.
In a randomized placebo-controlled trial, KCit reduced stone recurrence by more than 90%, whereas the placebo group showed no change in stone recurrence rate. 11 In patients with a history of calcium oxalate stones, compliance with alkalization resulted in a significant decrease in recurrence rates in those with upper tract calculi from 46.2% with no prophylaxis to 7.8% with regular KCit therapy. 12 In a randomized trial in adults recurrence after shockwave lithotripsy at 1 year was 0 with treatment and 28% without. 13 In this study, rates of residual fragments were also significantly better with treatment (4.5% vs 12.5%). Another randomized trial in children showed KCit therapy significantly decreased new stone formation compared with controls (7.6% vs 34.6%, respectively). 14 Last, in a double-blind, placebo-controlled trial K-magnesium Cit was associated with an 85% reduced risk of stone recurrence. 15
Despite its proven efficacy, compliance with KCit therapy is poor. In one study that looked at long-term follow-up of stone formers who were treated with low doses of sodium KCit, only 62% consistently took the medication. 16 The problems with compliance are poorly reported in the literature, but some reasons cited are high cost, bad taste, and inconvenience of bid or tid dosing. 17,18 Poor palatability has been attributed to the unappealing salty taste of most supplements. Despite flavor changes, crystal or liquid forms, and longer acting matrix formulations, long-term patient compliance is low. For these reasons, dietary replacements, such as lemonade, have been sought. Studies have shown mixed results, however, in the effectiveness of Cit-containing beverages to improve urine chemistries. No studies have been performed to show citrated beverages reduce stone formation. 19 –21
One possible way to improve palatability and compliance is to add an artificial sweetener to the powder form. Of the available sweeteners, sucralose (Splenda®) has been shown to be safe in high doses in both laboratory animals and humans. 22 In laboratory animals, the only side effect observed was cecal enlargement secondary to an osmotic effect of active substances. The cecal enlargement was not associated with histologic changes and not toxicologically significant. It was also not observed in dogs, mice, or primates. There has been no evidence of increase in malignancy, teratogenicity, neurotoxicity, or infertility with large supraphysiologic doses in animal models. 22,23 In humans, the majority of sucralose is excreted in the feces unchanged with only 14.5% excreted in the urine. 24
We hypothesized that Splenda taken at physiologic doses would significantly improve the palatability of KCit therapy. We also proposed that Splenda would not alter the efficacy of KCit at increasing pH and Cit in 24hour urine analysis.
Patients and Methods
This was a randomized, double-blind trial. Twenty-one patients were enrolled, and 12 patients completed the study. Criteria for inclusion in the study included age greater than 18 years, no known history of stone formation, and no history of metabolic disease predisposing to stone formation. Patients were asked to volunteer for the study and were not paid for their services. Standard medical history was taken, and patients with any contraindications to KCit supplementation were excluded. These included a history of ventricular fibrillation, hyperkalemia, Addison disease, adrenal hyperplasia, severe renal impairment, or oliguria. Further exclusion criteria included the use of angiotensin-converting enzyme inhibitor and angiotensin receptor blocker medications. There are no known contraindications to Splenda.
Patients were randomized to one of two pathways. Subjects and investigators were blinded to the pathway assignments. Only the research pharmacists had access to the randomization. Both pathways began with a baseline 24-hour urine study without any treatment for reference levels of urinary CIT and pH. All studies were performed by a central reference laboratory (Litholink, Chicago, IL). KCit/citric acid solution (Polycitra-K® oral solution) was the form of K supplementation used in this study. Subjects in the first pathway (group 1) received KCit/citric acid solution (PC/CA) alone (2 tsp=10 mL=20 mEq in 8 oz of water bid) for 3 days. To gauge the taste and palatability, a visual analog taste scale (Fig. 1) was completed. A 24-hour urine collection was performed after 3 days of therapy, and the collection was analyzed in the usual manner for stone risk. Subjects waited 1 week and then completed 3 days of therapy with PC/CA with Splenda (1 standard packet equivalent in the same dose concentration of Cit supplement).

Visual analog taste scale.
Subjects randomized to group 2 were started with 3 days of PC/CA with Splenda and then preceded to PC/CA alone. They completed the same visual analog taste scale and 24-hour urine testing (Fig. 2). Medication and packets were made to look exactly alike by the research pharmacists.

Randomization table.
Subjects were not limited by diet or activity level; however, they were instructed to consume a consistent diet during the study period and to keep their routine level of activity or exercise stable to help lessen variability. Urinary Cit concentration, pH, and standard 24-hour urine metabolic parameters were compared at baseline, with standard Cit supplementation, and with Splenda added to the standard supplement dose. The primary end points of the study were to determine if the sugar substitute improves palatability and taste with Cit supplementation, and to detect any effects of the sugar substitute on urinary Cit and pH.
Statistical analysis
The 24-hour urine parameters were analyzed using the repeated measures analysis of variance with the Tukey test applied for multiple comparisons. The tastes scores were analyzed with a paired t test. Analysis showed that with 20 subjects, there was at least an 85% power to detect a taste score difference of one standard deviation at the P<0.05 level. Institutional Review Board approval was obtained for this study. For security and confidentiality, all data were placed in a single database located in the urology academic/research offices at the Albany Medical Center South Clinical Campus, with access limited to the study investigators.
Results
The demographics for study subjects are shown in Table 1. There were an equal number of male and female subjects with a mean body mass index of 25 (19.2–34.9) and age of 29 (18–43). Because of poor compliance, only 12 of 21 subjects enrolled completed the entire study (Fig. 2). Two subjects in group 1 and three subjects in group 2 returned the medication unused. Of those who started the treatment, 0 of 6 who started on Splenda dropped out as opposed to 4 of 10 in the KCit group (Fisher exact test, P=0.23.)
BMI=body mass index.
The results of the taste and palatability analysis are shown in Figure 3. The average taste score when Splenda was added to KCit therapy was 3.25 (±0.37). This was significantly improved over KCit alone, which had an average score of 5.75 (±0.93). The difference in the taste score was 2.5 (±0.94) (P=0.02).
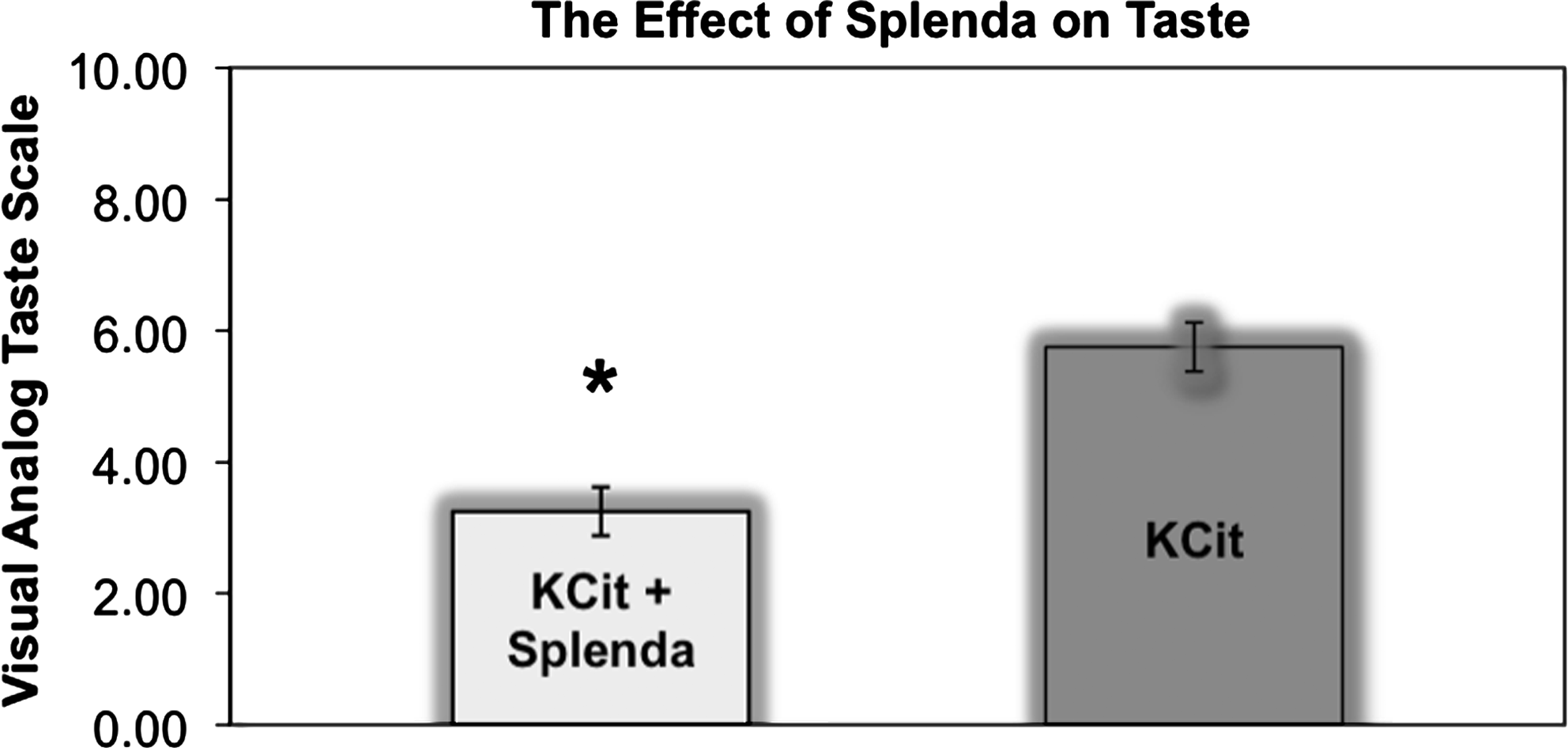
The effect of Splenda on taste. KCit=potassium citrate.
The results of the 24-hour urine collections are shown in Table 2. The 24-hour urinary Cit levels were significantly higher in the treatment groups compared with baseline (P<0.01) but not significantly different between KCit and KCit with Splenda (P=0.79). pH and 24-hour urinary K were also significantly higher in the treatment groups (P<0.02 and P<0.01, respectively) but the effect of KCit was again not altered by the addition of Splenda (P=0.99 and P=0.70, respectively).The 24-hour urinary phosphate levels trended higher with treatment but did not reach statistical significance (P=0.09 and P=0.06 for KCit alone and with Splenda, respectively). The 24-hour urinary ammonium levels also decreased with treatment (P=0.08 and P=0.03 for KCit alone and with Splenda, respectively). All other 24-hour urine parameters were not significantly altered by treatment.
Results expressed as mean value (standard error); urine parameters expressed in mg/d.
Significant change from baseline. P<0.05.
SS=super saturation; CaOx=calcium oxalate; Ca=calcium; CaPh=calcium phosphate; UA=uric acid; Na=sodium; K=potassium; Mg=magnesium; Ph=phosphate; NH4=ammonium; Cl=chlorine; Cr=creatinine; B=baseline; PC=potassium citrate; PC+S=potassium citrate+Splenda.
Discussion
We found that Splenda improved the palatability of KCit. In addition, Splenda did not alter the beneficial effects of KCit on urinary stone risk factors.
Both KCit and CA occur as colorless, translucent crystals or as a white powder. CA has a strongly acidic taste, and KCit has a saline taste. Potassium Citrate ER (Urocit®) is an extended release tablet available in 5, 10, and 15 mEq tablets. It is the more costly at $225.83/mo ($129.46 for generic) for 20 mEq tid dosing. 25 Potassium Citrate and Citric Acid for Oral Solution (Cytra-K® Crystals) is a crystal form and contains 1002 mg CA and 3300 mg KCit (1 packet provides 30 mEq of K and is equivalent to 30 mEq of bicarbonate) in a sugar-free base. It is reconstituted in 4 to 6 oz of water or juice. Cost is $120.60/mo for 1 packet qid. 25 Potassium Citrate and Citric Acid Oral Solution (Polycitra-K® oral solution) comes dissolved in an aqueous medium and was used in this study. Each mL of solution contains 2 mEq of K and bicarbonate. It is the cheapest at a cost of $74.54/mo for 1 mo at 15 mL qid. 25 If you added Splenda, this would add $4.20 to the monthly cost, which is significantly cheaper than other forms.
We found that Splenda improved the taste of KCit in our study. There are no other studies for comparison. We believe that most likely any sweetener would enhance the palatability of KCit. Splenda has been proven to be safe in large quantities and free of any significant side effects. Sucralose is a derivative of sucrose in which three hydroxyl groups are replaced by chloride ions. 23 This makes the molecule extremely stable and unable to be metabolized by the body. It is also stable at high temperatures and is commonly used in cooking. It is readily available and can be easily mixed with KCit powder and then reconstituted at the person's convenience by simply adding water.
By adding a sweetener with very few calories, the patient can avoid the need to take the medication with juice, which is notoriously high in calories. In comparison, the recommended volume of lemonade to achieve the equivalent amount of citrate in a standard dose of KCit would deliver 1700 kcals/week. 7 This would add 26 pounds of body fat over a year. Because it is necessary to take KCit twice or three times daily, adding Splenda makes it much more feasible to tolerate the unpleasant taste several times per day without adding unnecessary calories.
We chose healthy persons with no stone risk factors to avoid any confounding variables that preexisting metabolic abnormalities may have on urine parameters. In the setting of normal renal function, the rise in urinary citrate after a single dose begins by the first hour and lasts for 12 hours. 26 With multiple doses, the rise in Cit excretion reaches its peak by the third day and averts the normally wide circadian fluctuation in urinary Cit, thus maintaining urinary Cit at a higher, more constant level throughout the day. We chose 3 days of therapy so that persons would have a maximal response to therapy and enough doses to adequately judge taste. At maximal dose (60 mEq/d), KCit raises pH by an average of 0.7 units. 26 In this study, subjects received 40 mEq/d, and the pH improved by an average of 0.4 units in both treatment groups, implying that in this very short-term study, there was good compliance with alkalinization.
This study demonstrates that palatability may be one simple and economical way to achieve better compliance with KCit therapy in calcium oxalate and uric acid stone formers. Our results show a significant improvement in palatability with Splenda. It improved the taste score from one that might prohibit you from taking the medication (5.75) to one that would not (3.25) (Fig. 1). Unfortunately, this study was too short to evaluate compliance, but we predict that improvements in taste scores with Splenda would translate into improved compliance rates in stone formers. It is important to note that compliance rates with stone-preventing drugs are poor in general and that the inconvenience of a liquid formulation may negatively effect compliance. There are circumstances, however, in which a liquid form would be advantageous (those who cannot swallow a pill or those with rapid intestinal transit secondary to chronic diarrhea, small bowel resection, or chronic intestinal disease). Based on these results we are planning a randomized trial to evaluate the effect of Splenda on compliance, stone recurrence, and need for surgical intervention.
The main limitation of our study was the small sample size. Of 21 subjects enrolled, only 12 completed all three 24-hour urine collections. The improvement in taste with Splenda was significant, however, despite this limitation. Although our study was initially powered to detect a difference in one standard deviation in taste, the actual difference was much larger (2.5 standard deviations). We believe that this difference is not only statistically significant, but clinically important as well because it would change the taste score from one that would not prohibit the subject from taking the medication to one that might. More subjects dropped out who started with KCit therapy alone. Although this difference is not statistically significant (Fisher exact test, P=0.23), results may have been biased because some may have dropped out because of the taste. Contrary to this idea, none of the subjects who started in the Splenda group first dropped out when crossing over to KCit alone. In any case, if bias were present, it would tend to reduce the difference in taste perception we found, because presumably the subjects who dropped out would rate the taste negatively. Unfortunately, there were no questionnaires reporting the person's reasons for failure to complete the study.
The follow-up is another limitation. Because these subjects were naïve to stone disease and not paid for their participation, they had little motivation to take the medication long term. Compliance in a longer study would have been difficult in this population for these reasons. This being said, we believe that in this study, the compliance was sufficient with regard to the subjects who completed the study. We collected the medication bottles after the study and measured the amount of solution remaining. All of the subjects who completed the study consumed the required amount of medication. The follow-up was sufficient for the 24-hour urine parameters, because 3 days of KCit therapy is all that is needed to achieve maximum effect. Perhaps taste would have been reported differently 1 month later, but we have no reason to think that sensation of taste receptors would change after 1 month of therapy.
Conclusion
The addition of Splenda to KCit is well tolerated and significantly improves palatability. At the same time, it does not alter the beneficial effects of KCit on 24-hour urine parameters.
Footnotes
Disclosure Statement
No competing financial interests exist.