
Abstract
Introduction:
Probe-based confocal laser endomicroscopy (pCLE) is an emerging technology for dynamic, in vivo imaging of the urinary tract with micron-scale resolution. We conducted a comparative analysis of pCLE with a 2.6-mm probe and a 1.4-mm probe that is compatible with flexible endoscopes.
Materials and Methods:
Sixty-seven patients scheduled for bladder tumor resection were recruited. pCLE imaging was performed using 2.6- and 1.4-mm probes. Image quality with the different probes was examined and further compared with standard histopathology.
Results:
Images with the 2.6-mm probe have better resolution of cell morphology. The 1.4-mm probe has a wider field of view and better view of microarchitecture. While image quality with the 2.6-mm probe is superior, the 1.4-mm probe is compatible with flexible cystoscopy and maneuverability is maintained, enabling imaging of areas of the bladder that were previously challenging to access with the larger probe.
Conclusions:
The optical specifications of the 2.6-mm probe are more suitable for distinguishing urinary tract histopathology. Further design optimization to improve resolution and additional validation of the diagnostic accuracy of the smaller probe are needed to help extend application of pCLE for optical biopsy of the upper and lower urinary tract.
Introduction
Recently, we reported the first ex vivo and in vivo feasibility studies of pCLE in the urinary tract with a 2.6-mm imaging probe. 10,11 Using fluorescein as a contrast agent, we developed a pCLE imaging protocol and investigated its potential application for bladder cancer diagnosis. As the fifth most common cancer, bladder cancer has a high recurrence rate and requires lifelong surveillance. 12,13 White-light cystoscopy, the standard modality for the diagnosis, treatment, and surveillance of bladder cancer, has numerous well-recognized shortcomings, including operator dependency and challenges in differentiation of nonpapillary lesions, such as carcinoma in situ (CIS) from inflammation. 14,15
In this study, we examine the clinical feasibility of a recently available 1.4-mm probe 8 and performed a comparative analysis with the 2.6-mm probe. The smaller probe is compatible with flexible cystoscopes and could expand the potential applications of pCLE in the urinary tract.
Materials and Methods
With local institutional review board approval, patients scheduled to undergo cystoscopy under anesthesia or transurethral resection of bladder tumors were recruited from November 2009 to June 2010. White-light cystoscopy was first performed, followed by administration of fluorescein contrast and pCLE through a 26F resectoscope and/or a 15F flexible cystoscope (Karl Storz, Culver City, CA). As previously described, 400 mL 0.1% intravesical or 0.5 mL 10% intravenous fluorescein sodium (Alcon Laboratories, Inc., Fort Worth, TX) was administered for tissue contrast. 11 A single surgeon (J.C.L.) performed image acquisition and transurethral resection of bladder tumor. The confocal images were compared with standard histopathologic hematoxylin and eosin staining interpreted by a board-certified pathologist (K.C.J.).
The Cellvizio® system (Mauna Kea Technologies, Paris, France) was used for pCLE image acquisition and processing as previously described. 11 A 2.6-mm (GastroFlex UHD®) and/or 1.4-mm (AlveoFlex®) confocal probe was used for imaging. The 2.6-mm probe has the following optical specifications: resolution 1 μm, field of view (FOV) 240 μm, depth of focus (DOF) 60 μm, and optical slice thickness 10 μm; for the 1.4-mm probe: resolution 3.5 μm, FOV 600 μm, DOF 0 μm, and optical slice thickness 50 μm. Cystoscopy and pCLE video sequences were recorded in real time and further reviewed off-line. The probes were sterilized after each use, with Sterrad® (ASP, Irvine, CA) or Steris® (Mentor, OH).
Results
Overall, 67 subjects were recruited for the study. Forty-nine patients were imaged with the 2.6-mm probe, 11 with the 1.4-mm probe, and 7 with both probes. The mean age of the patients was 71 years (range 28–90). The mean imaging duration was 15.5 minutes per patient. There were 22 patients with low-grade urothelial carcinoma, 22 with high grade, 8 with CIS, and 17 with benign lesions. No significant adverse events were noted with either intravenous or intravesical fluorescein administration.
Figure 1 shows the compatibility of the 1.4- and 2.6-mm pCLE probes with standard urological endoscopes. The 1.4-mm probe fits within the working channels of standard flexible cystoscopes (15F), rigid cystoscopes (22F), and resectopes (26–28F), whereas the 2.6-mm probe fits within standard resectoscopes. With the 1.4-mm probe in the working channel, maneuverability of the flexible cystoscope was retained and all parts of the bladder were accessible, including the anterior and lateral walls that were previously challenging to image using the rigid scope in combination with the 2.6-mm probe. 8 As expected, visibility was reduced with the 1.4-mm probe in the flexible scope as a result of diminished flow of irrigation fluid.
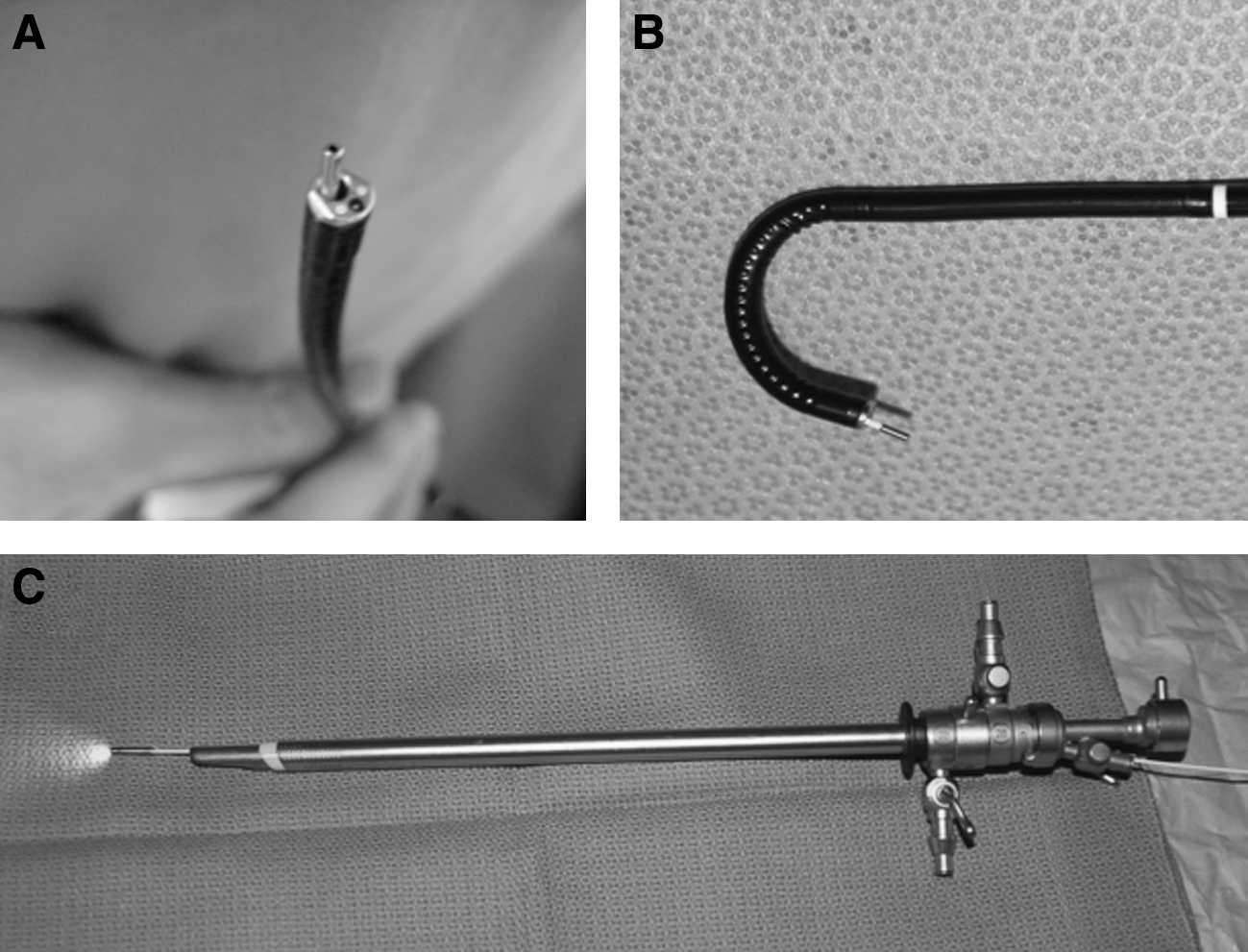
Compatibility of the confocal laser microscopy probes with standard urological endoscopes.
In addition to size, the two probes differ in optical specifications, including resolution, DOF, and FOV, which affect the quality and interpretability of images obtained from the bladder. With the 1.4-mm probe in contact with normal urothelium, the umbrella cells, intermediate cells, and lamina propria were observed with similar characteristics as previously observed with the 2.6-mm probe. 11 Notably, the image quality from the 2.6-mm probe was generally better, which is related to the greater number of fiberoptic fibers encased in the probe (approximately 30,000 compared with 10,000 for the 1.4-mm probe). With the 1.4-mm probe, the individual cells appeared smaller due to the larger FOV (Fig. 2) and comparatively; this made the assessment of the cellular morphology more challenging.
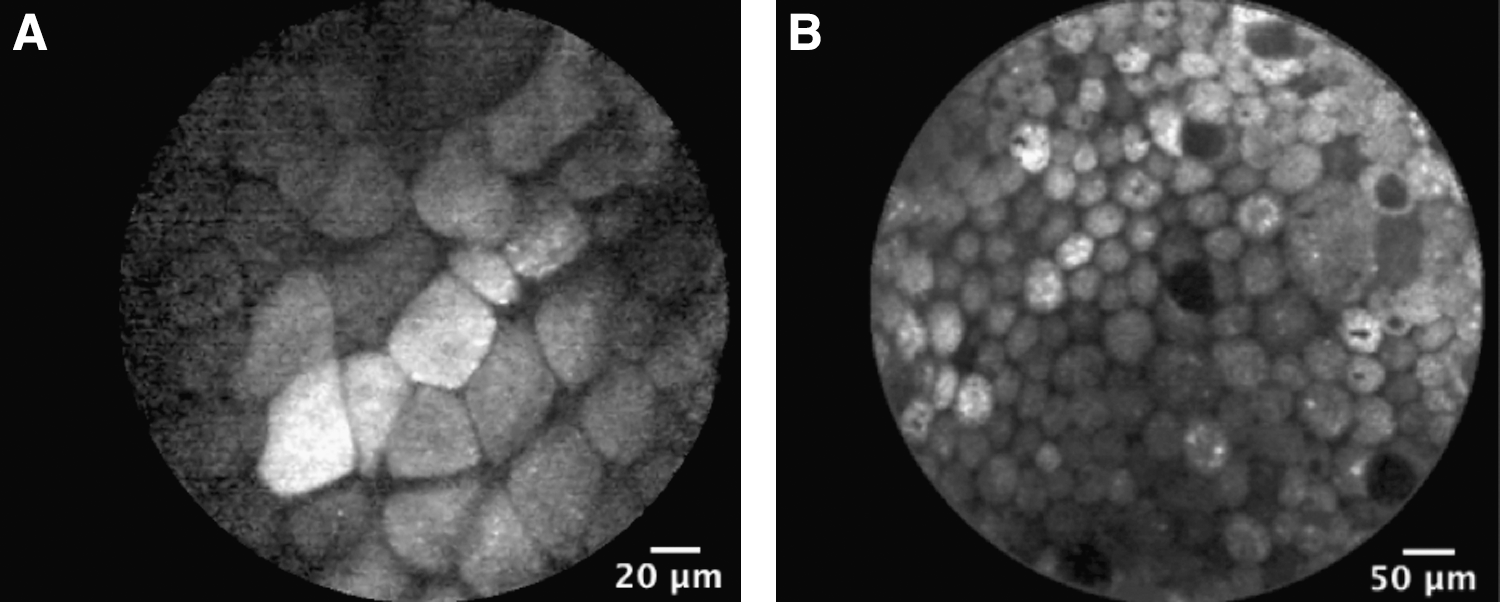
In vivo confocal images of umbrella cell layer of the normal urothelium using the
For bladder tumors, the pCLE images of low-grade tumors were characterized by densely packed cells and the presence of fibrovascular stalks, whereas high-grade tumors displayed a much greater degree of pleomorphism and poor cellular cohesiveness. As seen in Figure 3, the 1.4-mm probe provided a broader view of tumor microarchitecture, whereas the 2.6 mm was superior in detailing the cellular morphology, which is particularly important in differentiating high- and low-grade tumors. A defining characteristic of papillary bladder cancer is the presence of fibrovascular stalks related to neoangiogenesis and the presence of flowing erythrocytes, both of which were more easily observed with the 2.6-mm probe. Figure 4 shows a representative example of a low-grade tumor that was imaged with both the 2.6- and the 1.4-mm probe.
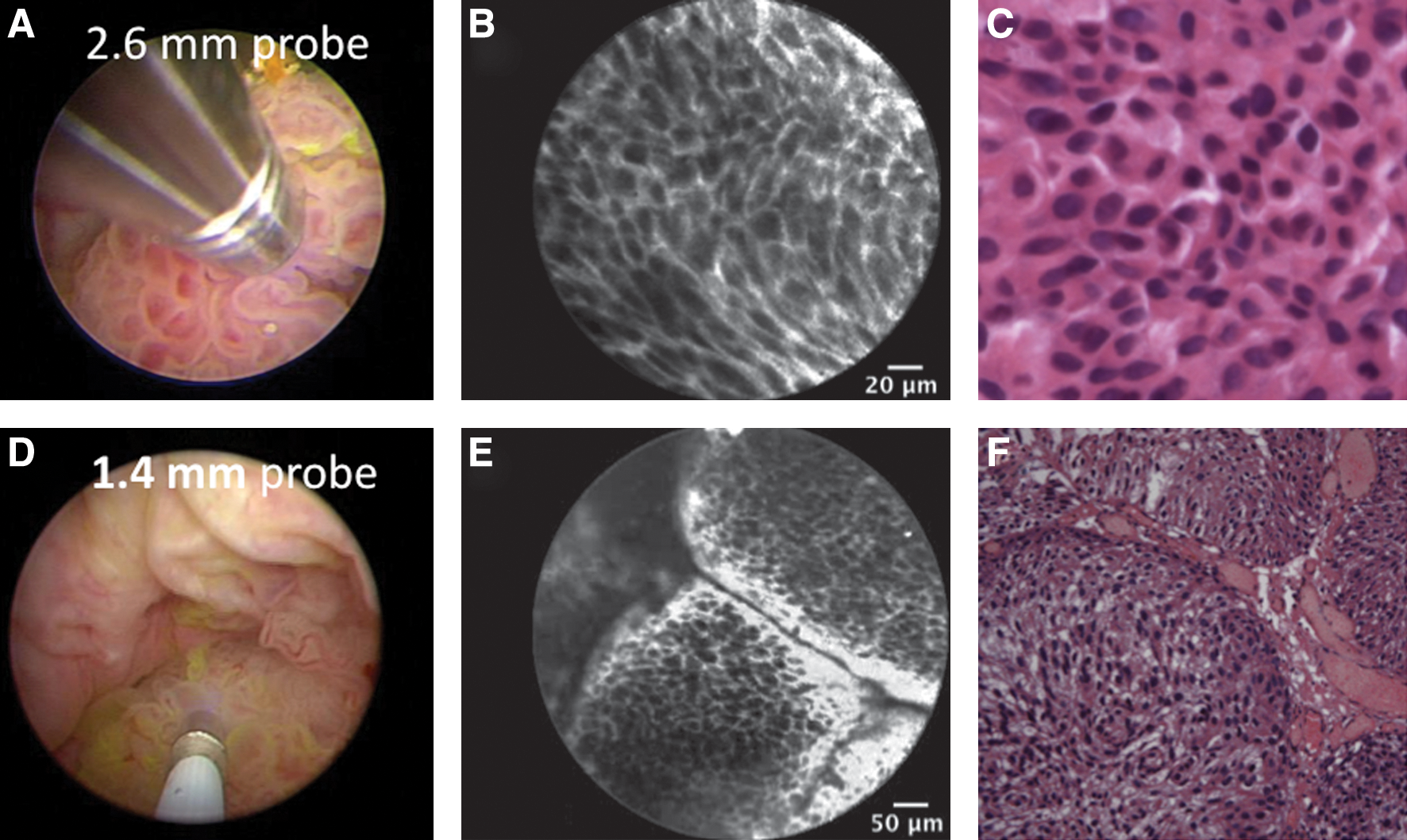
Comparison of the in vivo confocal images acquired with the 2.6-mm
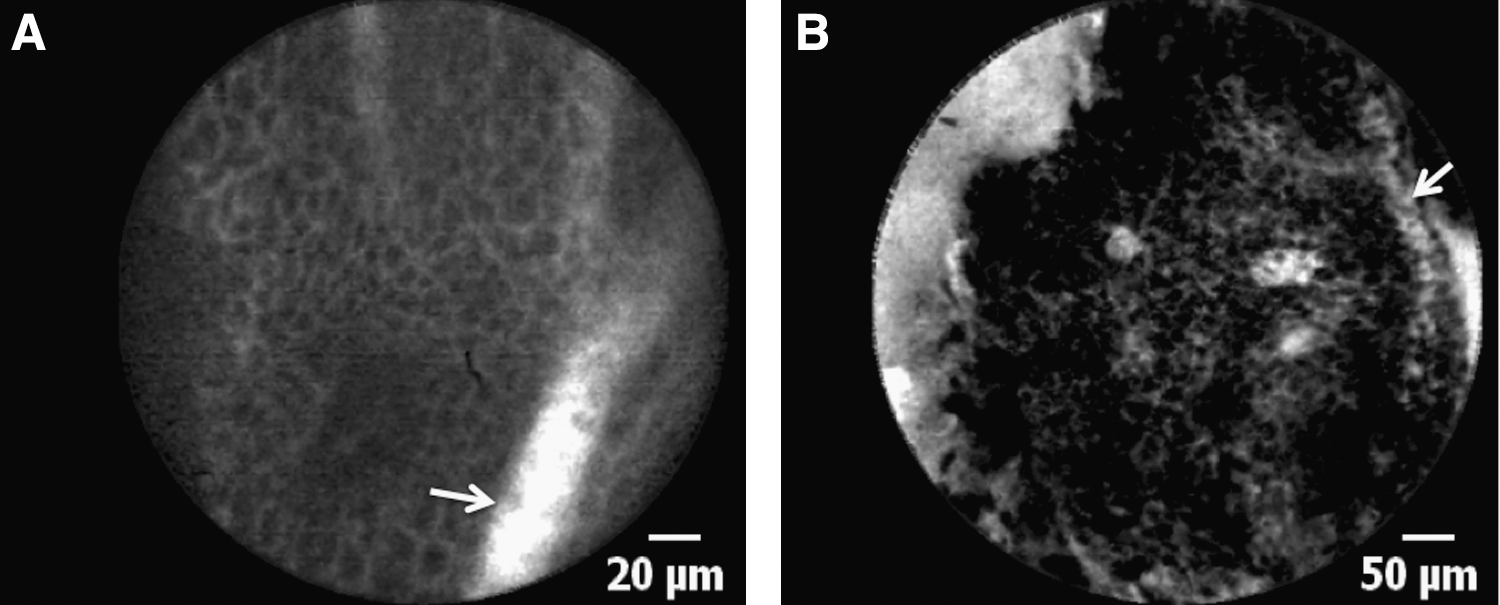
Comparison of the in vivo confocal images acquired with the
Discussion
The ability to obtain real-time histopathologic diagnosis in a noninvasive manner during endoscopy is an attractive concept that could reduce unnecessary biopsies in some clinical situations while improving biopsy yield in others. Potential applications of pCLE during endourologic procedures include differentiation of CIS from inflammatory lesions and confirmation of upper tract urothelial carcinoma, where current standard biopsy has suboptimal yield. Further, the ability to perform pCLE in an outpatient setting may potentially decrease unnecessary procedures under anesthesia, which carries nontrivial risks and potential complications.
In contrast to other optical imaging modalities, pCLE offers the versatility of different probe sizes and compatibility with standard endoscopes. Currently, use of the 2.6- and 1.4-mm probes and their corresponding optical specifications are established for gastrointestinal and respiratory tracts, respectively. The ideal imaging probe for the urinary tract is sterilizable and compatible with the diverse selection of flexible and rigid urological endoscopes, while still capable of generating high-resolution images that are easily interpretable. Although the probes are not specifically designed for the urinary tract, we previously demonstrated that the 2.6-mm probe can be used to image the urinary tract, and we now assess the feasibility of the 1.4-mm probe and compared the image quality obtained with the two probes.
As previously noted, 11 pCLE imaging of some tumors located at the anterior and lateral bladder walls with the 2.6-mm probe is challenging, since the probe needs to have en face contact with the tissue of interest. In contrast, the 1.4-mm probe is compatible with all cystoscopes, including flexible, and enables adequate maneuvering of the scope to image all parts of the bladder. While the 1.4-mm probe provides a greater FOV (600 μm) and thus improved delineation of microarchitecture, we found that the improved cellular resolution provided by the 2.6-mm probe was more helpful in determining a histological diagnosis. In effect, the 1.4-mm probe provides a low-power view, whereas the 2.6 mm provides a high-power view. Cellular and nuclear morphology, as opposed to microarchitecture, play a more critical role in the diagnosis and grading of bladder cancer. Since fluorescein is an extracellular stain, the improved assessment of cellular morphology with the 2.6-mm probe becomes particularly important.
Efforts are currently underway to evaluate the diagnostic accuracy of pCLE for bladder cancer and to assess interobserver variability. Other potential applications include pCLE for the upper urinary tract with the availability of probes <1 mm in diameter 16,17 and endoscopic molecular imaging with tumor-specific contrast agents. 18 –20
Conclusions
We report a feasibility study of pCLE in the urinary tract with a 1.4-mm probe and a comparative analysis with a 2.6-mm probe. Both probes were capable of generating histological-grade images of the lower urinary tract in vivo. We found that the optical specifications of the 2.6-mm probe were superior for urinary tract imaging, whereas the 1.4-mm probe was more versatile for various urological endoscopes. Development of imaging probes with optical specifications optimized for urological applications (improved maneuverability while retaining high resolution) may facilitate incorporation of pCLE as a useful tool for urinary tract endoscopic procedures.
Footnotes
Acknowledgments
We thank Kathy Mach for helpful discussions and critical review of the article. Funding support was provided by Stanford University Cancer Center Developmental Cancer Research Award (J.C.L.), and technical support was from Mauna Kea Technologies.
Disclosure Statement
None of the authors have any conflicting financial interest with regard to this technology.