
Abstract
Background and Purpose:
In addition to their lipid lowering effects, HMG-CoA reductase inhibitors (statins) have been shown to exert antithrombotic effects through downregulation of the coagulation cascade. Because statin use is widespread, it is important to understand the impact of these drugs on blood loss (BL) during surgery. We studied the impact of statin use on BL during robot-assisted radical prostatectomy (RARP) and open radical prostatectomy (ORP).
Patients and Methods:
A retrospective review was conducted of a database approved by the Institutional Review Board for patients who underwent RARP or ORP at a single academic institution. Patients were categorized as statin-users or statin-naïve at the time of surgery. Patient demographic information was recorded as was perioperative data, including preoperative and postoperative hematocrit (Hct) value. BL was defined as % Hct change presurgery vs postsurgery. In addition, the outcome of ≥10% drop in Hct was studied. The t test and chi-square analysis were used to compare variables across statin use groups. Univariate and multivariable logistic regression analyses were used to identify factors that impacted BL.
Results:
From 1987 to 2010, 3578 patients underwent prostatectomy for prostate cancer (RARP=945 and ORP=2633). Of these, 676 men were identified as statin-users and 2902 as statin-naïve. Mean patient age was 60.2±7.0 years. Statin-users were found to be older (P<0.001), have lower mean preoperative prostate-specific antigen (PSA) levels (P=0.002), and have higher pathologic Gleason sum scores (P<0.001). For ORP, statin use was associated with increased BL with Hct % change of 20.7% for users vs18.6% for nonusers, (P<0.001). For RARP, no significant change in Hct was seen with statin use with % changes of 12.6% and 12.5%, respectively (P=0.9). When controlling for age, Gleason sum, surgeon, date of surgery and PSA level, statin use was associated with increased BL (P=0.04).
Conclusion:
Even when controlling for age, Gleason sum, surgeon, date of surgery, and PSA, statin use is associated with increased BL during RP. This information may impact preoperative planning and patient counseling for men who are taking statins while preparing for RP.
Introduction
Because statins are widely used, many patients undergo surgical procedures while receiving statin therapy. It is therefore imperative to better understand their effects on this population. Surgical outcomes for patients receiving statin therapy have been explored to some extent. Preoperative statin therapy has been associated with a reduction in the risk of all-cause mortality after cardiac, vascular, and noncardiac surgery. 8 Specific to their impact on coagulation, statins have been found to be associated with an increased risk of postoperative wound hematoma/hemorrhage in patients who have undergone inguinal herniorrhaphy. 9
The role that statins may play intraoperatively, however, has not yet been examined. Given that statins have been shown to produce an antithrombotic effect as well as increase the risk of postoperative bleeding, it was postulated that intraoperative blood loss (BL) might be affected by statin use. The purpose of this study was to examine the impact of statin use on BL during robot-assisted radical prostatectomy (RARP) and open radical prostatectomy (ORP).
Patients and Methods
This study was a retrospective review conducted of an urologic oncology database that was approved by the Institutional Review Board for patients who underwent RARP or ORP at a single academic institution. All patients who were undergoing radical prostatectomy (RP) (n=4680) between 1987 and 2010 were screened for inclusion into the study. Patients were excluded if they were missing either a preoperative or postoperative hematocrit (Hct) level. Blood samples for Hct analysis were taken preoperatively and within 24 hours after surgery. A total of 3578 patients were included in the final analysis. Preoperative statin use was determined by the medication list in the postoperative discharge summary, and patients were categorized as statin-users or statin-naïve at time of surgery.
Patient demographic information was recorded including age, race, and body mass index (BMI) as was perioperative data including preoperative prostate-specific antigen (PSA) level, pathologic Gleason sum, and preoperative and postoperative Hct. Patients were also stratified into quartiles based on the date of surgery to evaluate the impact of time on BL and statin use. BL was defined as a % change of Hct before vs within 24 hours after surgery. In addition, the outcome of a ≥10% drop in Hct was studied as a marker for clinically significant BL. Two sample t tests and Pearson chi-square analyses were then used to compare variables across statin groups, and univariate and multivariable logistic regression analyses were used to identify factors impacting intraoperative BL.
Results
Between 1987 and 2010, 3578 patients who underwent prostatectomy for prostate cancer (RARP=945 and ORP=2633) were found to meet the inclusion criteria for this study. Of these patients, 676 (18.9%) men were identified as statin-users and 2902 (81.1%) as statin-naïve. Patient demographic information is summarized in Table 1. The mean patient age was 60.2±7.0 years. Sixty-two percent of patients were Caucasian, 13.2% were African American, 10.8% were Hispanic, and 14.0% were described as “other race.” Mean BMI for the entire cohort was found to be 29.5±3.6 kg/m2. Mean preoperative PSA level was found to be 8.0±7.9 ng/mL, and the pathologic Gleason sum breakdown for the cohort was 32.8% <6, 54.7%=7, and 12.5% >7. Mean preoperative Hct was 41.1±4.3%, and the mean postoperative Hct was 34.2±5.0%.
Two sample t test.
Pearson chi-square test.
Pre-tx=before therapy; PSA=prostate-specific antigen; BMI=body mass index.
Statin-users were found to be significantly older (61.1±6.5 vs 59.9±7.0 y, P<0.001), have lower preoperative PSA levels (7.1±6.4 vs 8.2±8 .2 ng/mL, P=0.002), and be more likely to have Gleason sum score ≥7 (74.7 vs 65.4%, P<0.001). In addition, a greater percentage of patients undergoing RARP were found to be statin-users compared with men undergoing ORP with usage rates of 29% vs 15% (P<0.001), respectively. No significant differences were found across statin-user groups for race, BMI, preoperative Hct, or postoperative Hct.
For ORP, statin use was associated with increased BL with Hct % change of 20.7% vs18.6%, respectively (P<0.001) (Fig. 1). For RARP, no significant % change in Hct was seen with statin use with % changes of 12.6% and 12.5%, respectively (P=0.9) (Fig. 2). In addition, statin-users were significantly more likely to drop ≥10% in Hct compared with nonusers in the ORP group with percentages of the ORP patients meeting this outcome of 33.6% vs 27.7%, respectively (P=0.02). This significant difference was not seen for RARP patients (P=0.6). Although % change in Hct and change in Hct ≥10% were the primary outcome measures for this study, results are also reported for other measures of BL in Table 2. For patients who were undergoing RARP, statin use was associated with a decreased postoperative Hct compared with nonstatin-users with means of 37.8±4.5% vs 38.8±4.2%, (P=0.01). ORP statin-users had a greater absolute drop in Hct compared with nonusers with changes of 8.6±4.6% vs 7.7±4.4%, respectively (P<0.001). No significant differences were seen across statin-user groups for the outcome of estimated BL.
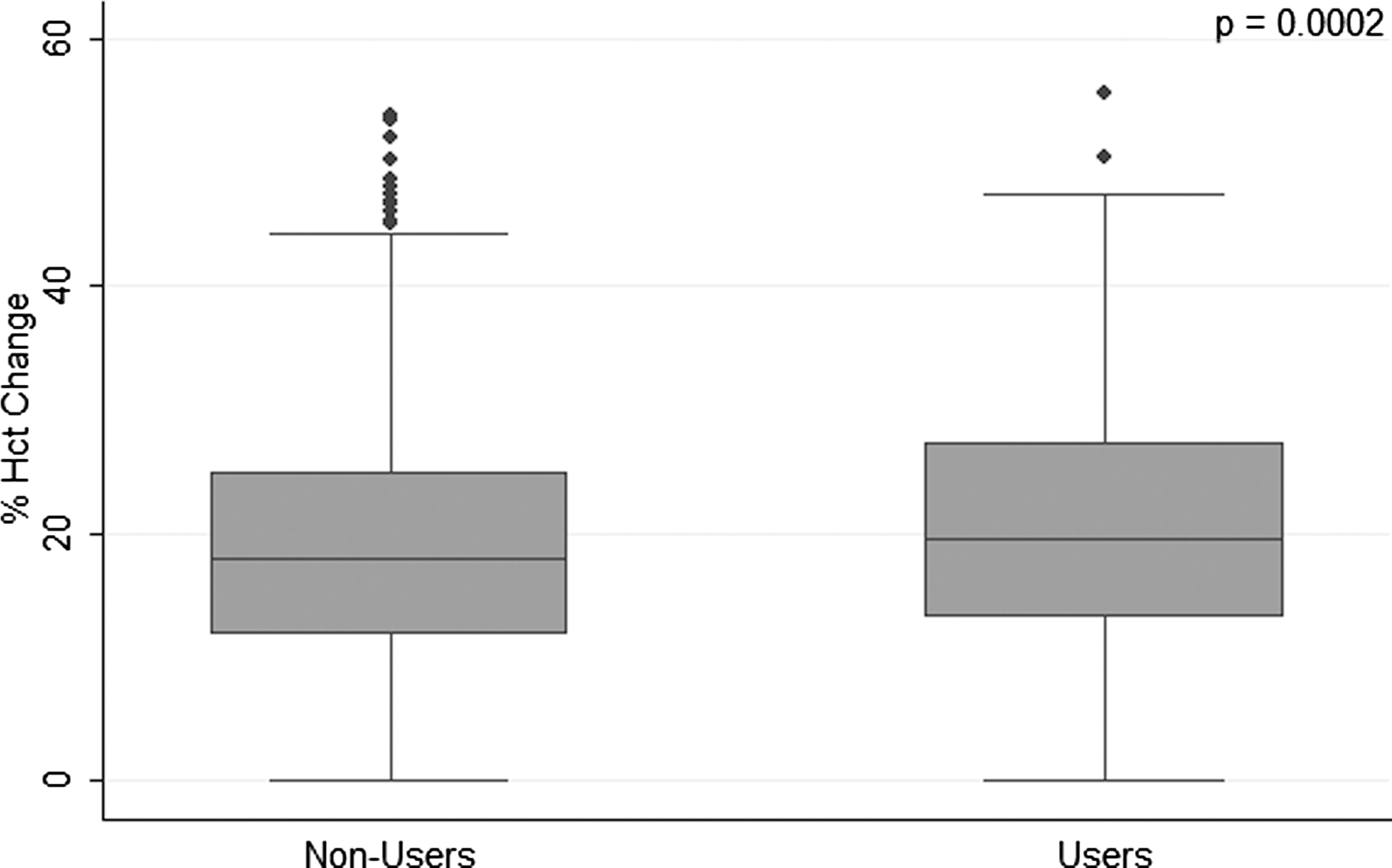
Box plot of hematocrit percent change during open radical prostatectomy: Statin-users vs statin-nonusers.
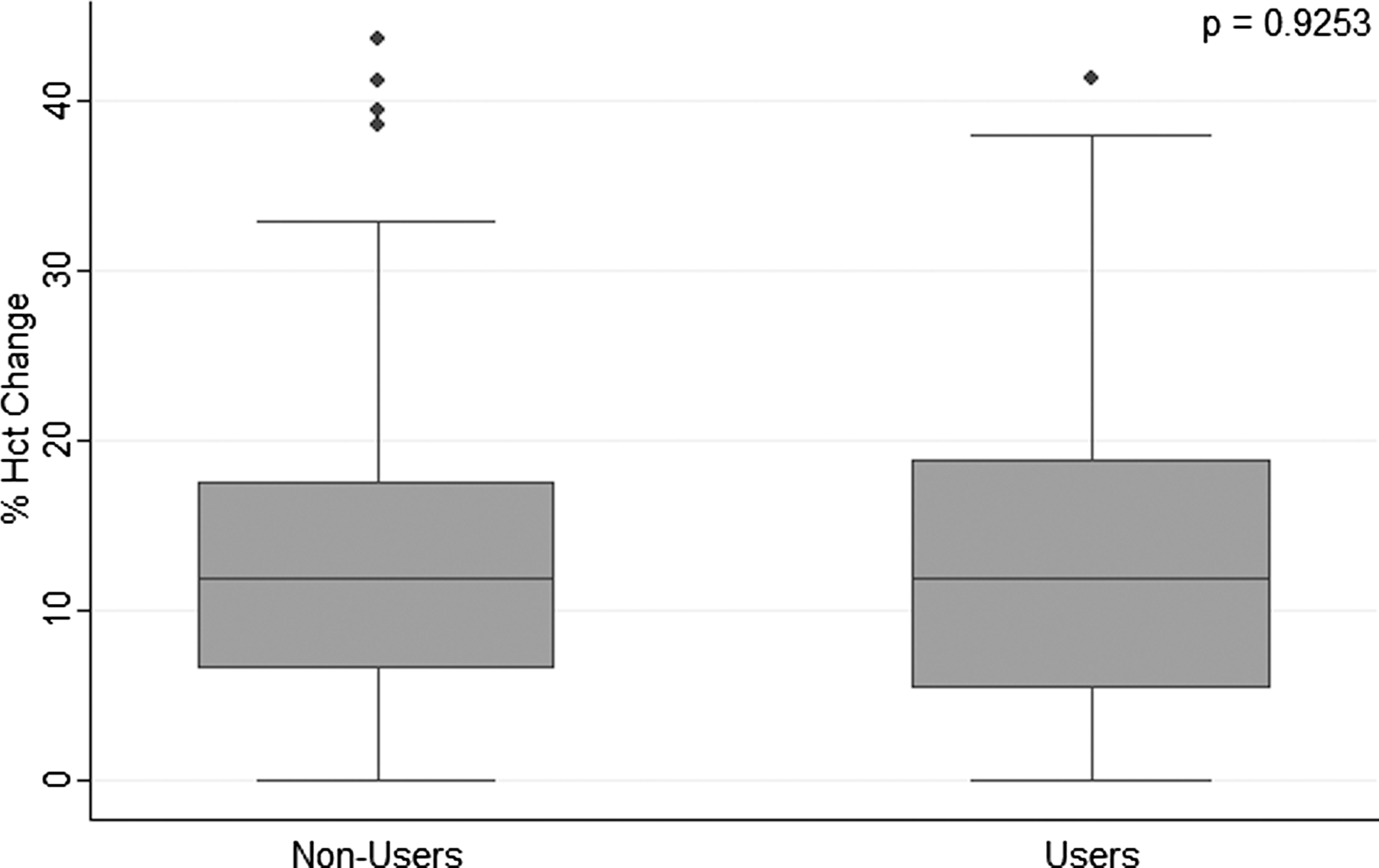
Box plot of hematocrit percent change during robot-assisted radical prostatectomy: Statin-users vs statin-nonusers.
Denotes significance.
ORP=open radical prostatectomy; RARP=robot-assisted radical prostatectomy; SD=standard deviation; postop=postoperative.
The impact of date of surgery on BL and statin use is detailed in Table 3. For patients who were undergoing ORP, there was a significant difference across quartile groups for Hct % change, increasing from 13.0±7.0% in the first quartile (1987–1997) to 25.3±9.4% in the fourth quartile (2006–2010), (P<0.001). In contrast, there was a significant decrease in the % change Hct for RARP from 13.9±9.2% in the third quartile (2001–2006) to 11.9±8.0% in the fourth quartile (2006–2010), (P<0.001). In addition, the prevalence of statin use in the entire cohort significantly increased over the study time period from 7.8% in the first quartile to 30.8% in the fourth (P<0.001).
Denotes significance.
Hct=hematocrit; SD=standard deviation; RARP=robot-assisted radical prostatectomy.
A significant difference in BL was seen across surgeons using the open approach, with means of % changes in Hct ranging from 19.4% to 26.2% (P<0.001). This intersurgeon difference was also seen for the % of patients with a ≥10% drop in Hct after ORP, with ranges from 12.6% to 67.4% (P<0.001). A significant difference in BL across surgeons was not seen for the robotic approach for either the % change in Hct (P=0.4) or the % of patients with ≥10% drop in Hct (P=0.5).
On univariate analysis of the full cohort using the clinical event of ≥10% drop in Hct, increased BL was found to be significantly associated with Gleason grade ≥7 (P=0.01), open surgical approach (P<0.001), younger age (P=0.03), and more recent date of surgery (P<0.001). No significant association with BL was seen for statin use (P=0.5), preoperative PSA level (P=0.5), or BMI (P=0.9). On multivariate analysis of the entire cohort (Table 4), when controlling for statin use, Gleason sum, surgical approach, surgeon, date of surgery, race, age, and preoperative PSA level, increased odds ratio for BL was found to be significantly associated with statin use (P=0.04), black race (P=0.05), surgeon (P=0.02), open surgical approach (P<0.001), and more recent date of surgery (P<0.001). On multivariate analysis of the entire cohort, no significant association with BL was seen for Gleason sum, age, or preoperative PSA level.
Denotes significance.
Statin use is compared to nonstatin-users. Gleason=7 and Gleason>7 compared with Gleason <7. Race compared with Caucasian race. Surgeons (2–7) compared with Surgeon 1. Surgical approach: Open radical prostatectomy compared with robot-assisted radical prostatectomy.
OR=odds ration; CI=confidence interval; Sx=surgery; PSA=prostate-specific antigen.
On subsequent stratification by surgical approach using the clinical event of a ≥10% drop in Hct as outcome, univariate analysis for ORP showed increased BL to be significantly associated with statin use (P<0.02), Gleason grade ≥7 (P<0.001), younger age (P=0.01), and more recent date of surgery (P<0.001). No significant association was seen for the incidence of a ≥10% drop in Hct after ORP for preoperative PSA level (P=0.2) or BMI (P=0.1). On multivariate analysis (Table 5) of ORP patients, when controlling for statin use, Gleason sum, surgeon, date of surgery, race, age, and preoperative PSA level, increased odds ratio for BL was found to be significantly associated with black race (P=0.02), surgeon (P<0.001), and more recent date of surgery (P<0.001). A borderline significant association was seen in the multivariable analysis for statin use on increased odds ratio for BL after ORP (P=0.06).
denotes significance.
denotes borderline significance.
Statin use is Compared to Non-Statin Users. Gleason=7 and Gleason >7 Compared to Gleason <7. Race Compared to Caucasian Race. Surgeons (2-5 for ORP and 2-4 for RARP) Compared to Surgeon 1. Note, Surgeons in ORP and RARP are different.
Univariate analysis for RARP patients showed no increased BL associated with statin use (P=0.6), Gleason grade (P=0.8), age (P=0.9), or preoperative PSA value (P=0.5). Increased odds for BL was seen for older surgery date (P<0.001). On multivariate analysis for RARP patients (Table 5), when controlling for statin use, Gleason sum, surgeon, date of surgery, race, age, and preoperative PSA value, only surgeon (P<0.001) and older date of surgery were found to be associated with increased odds ratio for BL (P<0.001).
Discussion
Statin use continues to increase in the United States with a total estimated use of these drugs by 24 million men and women. 10 –12 Recent studies suggest that statins may alter components of the coagulation cascade, thereby producing an antithrombotic effect. This may be best understood by considering why lipids may be prothrombotic. Lipoprotein(a), which is commonly associated with circulating low-density lipoprotein-cholesterol and postprandial triglyceride-rich particles, is structurally and functionally homologous to plasminogen; this suggests a potential for competitive binding to fibrin and hence to impaired fibrinolysis. 13 Factor VII coagulant (FVII:C) may also play a role, because postprandial lipemia has been associated with transient changes in FVII:C activity. 14 The antithrombotic effect of statins may be because of their function in modulation of this activity, because statin use has been shown to be associated with decreased concentrations of FVII:C. 15 Furthermore, indirect markers of thrombin generation, such as prothrombin fragment F1.2, have been shown to be significantly reduced with statin therapy. 16 This may be because of the ability of statins to inhibit platelet-derived protease-activated receptor-1 and tissue factor upregulation, leading to thrombin generation. 17 Given this current understanding of the role of statins in coagulation, it is important to consider the impact of these drugs on intraoperative BL.
Numerous studies comparing intraoperative BL during prostatectomy between the robotic and open approaches have agreed that greater BL is seen during ORP than RARP, with means ranging from 418 mL to 970 mL vs 103 mL to 329 mL (P<0.05), respectively. 18 –22 It is widely accepted that factors contributing to decreased BL for the robotic approach include improved visualization of the dorsal venous complex and other veins, facilitating intraoperative ligature as well as the tamponade effect of the pneumoperitoneum during laparoscopy. An important limitation of these studies, however, is the use of estimated BL, a measure that, while informed by objective data including number of surgical sponges used and amount of fluid in the suction device minus the amount of irrigant used intraoperatively, is still by definition a subjective estimation that is prone to bias.
Furthermore, while some studies have attempted to use more objective measures of BL, including absolute change in Hct (postoperative minus preoperative Hct), 20 hemoglobin level at discharge, 19 or percent of patients with ≥10% drop in Hct, 23 even these measures fail to account for individual variation of the magnitude of red blood cell concentrations at baseline. In an effort to take this variability into consideration while objectively measuring intraoperative BL, we choose to use the percent change in Hct before vs postoperative day 1 as one of the primary outcome measures for this study. We also used the clinical outcome of a ≥10% drop in Hct, because this event has been shown in a previous study to be correlated with the need for transfusion in men after RP. 23 We used this surrogate clinical end point because no patients in our study needed transfusion. Finally, to allow comparisons with previously published studies, we also report absolute change in Hct, Hct level at discharge, and estimated intraoperative BL (Table 2).
Recently, there has been growing interest on the impact of statin use on prostate cancer progression, with some researchers suggesting that statin-users may have a lower risk of advanced prostate cancer than nonusers. 24 –27 Specifically, studies demonstrate that statin-users have significantly lower PSA values 24,28 compared with nonusers. It is hypothesized that this may be, in part, because statins' ability to inhibit inflammation, 29 angiogenesis, 30 cell proliferation, 31 migration/adhesion, 32 invasion, 33 and to promote apoptosis in tumor cells. 28,34 In line with these previous reports, there were significant differences in our study cohort between statin-users and nonusers. Specifically, statin-users were found to be older, have lower PSA levels, and higher Gleason sum scores. For this reason, it was imperative to control for these significantly different variables through a multivariable analysis.
After univariate analysis, factors significantly associated with increased BL including increased Gleason grade, surgeon, date of surgery, open surgical approach, race, and younger age were then included in a multivariable model to control for these significant variables. In addition, date of surgery was also used as a control for the increasing rate of statin use seen in our patient population over the study period (Table 3). Although statin use was not found to be significantly associated with increased BL on univariate regression analysis, once these significant confounders were accounted for in the multivariate model, a significant association was uncovered with statin-users being at greater risk for BL compared with nonusers for the entire population of men undergoing RP (P=0.04). Further examination of the multivariate model highlighted a significant contribution of surgical approach on BL (P<0.001).
For this reason, we stratified the study population by approach to appropriately control for this variable and reran the univariate and multivariate models. After stratification, a significant association was seen in the univariate model for statin use on BL for the ORP group (P=0.02) but not for the RARP group (P=0.6). Given that the frequency of the clinical event of a ≥10% drop in Hct was more than two times greater for the open approach compared with the robotic approach, with prevalence rates of 28.6% vs 9.5%, respectively, it is possible that the decreased statistical power for RARP was too small to detect a significant difference. In addition, on multivariable analysis of only the ORP group when controlling for all confounders, only a borderline significant association was found with statin use (P=0.06), which could also be a result of the decreased power after the loss of sample size in the multivariate model.
In addition to statin use, our analysis also found a significant association for increased BL with increased Gleason sum, younger age, black race, and more recent date of surgery for ORP and older date of surgery for RARP. It is possible that the impact of younger age is driven by the fact that younger patients are more likely candidates for enhanced nerve sparing, which can result in increased bleeding because of the nature of the delicate dissection. In addition, the relationship of increased Gleason sum could be because patients with more invasive disease need a larger excision, which can result in increased BL.
Finally, the impact of surgical date on BL seen in our study was found to be opposite for RARP and ORP. Decreased BL was seen in the most recent quartile compared with earlier surgeries for the RARP approach, likely driven by the surgical learning curve. In contrast, for the ORP approach, greater BL was seen in the most recent surgeries possibly because of the increased use of nerve-sparing techniques that can result in more BL. Because of these differences, it was important to control for these effects in the multivariate model.
Perhaps the most troubling and perplexing finding is the impact of race on BL. While it is possible that the differential increased BL that was seen in black patients at our institution is a result of a genetic variation or underlying comorbid medical condition impairing coagulation, this finding could also be a result of some unseen systemic problem, resulting in the disparity. Certainly, future study is needed to better elucidate and understand the causes of these findings.
There are important limitations to consider when interpreting the results of this study. First, the clinical significance of the increased BL in the statin-user groups is most likely negligible, given that there was only a difference in Hct % change of 2.1% in the ORP patients. Although this magnitude in the general population may not contribute to overall survival or negative outcomes after surgery, it may become more important in patients with clotting disorders, putting them at increased risk for intraoperative bleeding. In such cases, the knowledge that statin use may lead to increased risk of intraoperative bleeding may affect the surgical approach used or the aggressiveness of intraoperative hemostatic techniques. In addition, given the significant differences seen at baseline between the statin-users and nonusers, it is difficult to ascertain whether the cause of the detected difference in intraoperative BL is because of an impact on the coagulation cascade or simply reflects a physiologic difference in the cancerous tissue itself, presumably from chronic statin use.
Future larger studies that evaluate the impact of statin use on intraoperative BL in both cancer and noncancer patient models may help to elucidate the mechanism of action of this effect. In addition, future studies that focus on patients with diagnosed clotting disorders may help to identify a clinically significant contribution of statin use on intraoperative BL, thus informing surgical planning and management. Other important limitations include the lack of data on intraoperative intravenous fluid administration, clinical stage, degree nerve spare, as well as the patients' American Society of anesthesiologists scores, which could impact the outcome measures of % change in Hct and/or the clinical event of a ≥10% drop in Hct and should ideally have been included in the multivariate model.
Conclusion
Even when controlling for age, race, Gleason sum, surgeon, date of surgery, and preoperative PSA level, statin use is associated with increased intraoperative BL during prostatectomy. Although this information may impact preoperative planning and patient counseling for men who are taking statins while preparing for RP, future larger studies are needed to elucidate the mechanism of action for this finding.
Footnotes
Disclosure Statement
No competing financial interests exist.