
Abstract
Purpose:
We determined how surgical outcomes differ among children undergoing prone retroperitoneoscopic (RP) and open total and partial nephrectomies for benign renal disease.
Patients and Methods:
A retrospective analysis was performed, using medical records of children who were undergoing benign renal surgery at a single institution from 2001 to 2010. Patients were divided into open or RP cohorts, then subdivided into those who were undergoing total or partial nephrectomies. A further breakdown by age (<3 years and ≥3 years) was performed. Bilateral nephrectomies were separately evaluated. Surgical outcomes were compared across groups.
Results:
There were 308 (333 renal units) children who underwent RP (n=154) or open (n=154) total or partial nephrectomies, 25 of which were bilateral (20 RP, 5 open); 199 patients underwent total nephrectomies (RP n=118, open n=81), and 109 underwent partial nephrectomies (RP n=36, open n=73). After controlling for age and concomitant procedures, operative times were similar for the RP total and bilateral nephrectomy groups, but longer for the RP partial nephrectomy group, compared with their open counterparts. In both total and partial nephrectomies, the RP group had a shorter hospital stay. There were no open conversions in any of the RP groups and no differences in complications in the total, partial, and bilateral analyses. There were 13 patients who previously received peritoneal dialysis (8 bilateral RP, 3 unilateral RP, and 2 unilateral open), all of whom resumed dialysis in a mean of 1.11 days.
Conclusions:
This is the largest series to date that compares RP and open renal surgeries in children. The RP and open approaches were comparably safe and efficacious. Hospital stays were significantly shorter in the RP total and partial groups, although operative times were significantly longer in the RP partial nephrectomy group. Prone retroperitoneoscopic surgery should be considered a viable option for renal surgery at any age.
Introduction
The retroperitoneal approach offers similar advantages as those of the transperitoneal approach and can be performed with the patient in the flank or prone position. Advocates of the retroperitoneal approach claim that this approach also facilitates access to the kidney and hilar structures by using the potential retroperitoneal space, 3 while obviating the need for bowel retraction and intraperitoneal dissection. Furthermore, by avoiding the peritoneum, complications related to intra-abdominal adhesions (both preoperative and postoperative) are avoided, 7 the risk of ileus and inadvertent injury to the bowel and surrounding structures is minimized, 8 and peritoneal dialysis (PD) can theoretically be resumed sooner. 9,10 Retroperitoneal surgery has also been shown to have shorter operative times and postoperative analgesic requirements, compared with transperitoneal surgery. 11,12
When performing laparoscopic renal surgery, we prefer the prone retroperitoneal approach. With the patient lying prone, gravity directs the flow of blood away from the surgical field, reducing the need for suctioning. The renal artery presents before the vein, and the renal vessels are under traction from gravity, allowing for an easier hilar dissection. Furthermore, we find it conceptually easier to predict anatomic relationships within the retroperitoneum when the patient is prone as opposed to propped in the flank position. It is easier for us to conceptualize the posterior-to-anterior reconfiguration in the prone approach than it is to spatially reorient ourselves to the lateral shifts that occur with the flank approach. 7
Although several studies exist in the literature that have examined the clinical outcomes of children undergoing retroperitoneoscopic (RP) renal surgery, the majority are limited by small patient populations 13 –16 or lack of an appropriate comparison group. 17 –21 In addition, these studies remain limited in their scope, focusing on either total or partial nephrectomies, or on a specific age group.
We sought to evaluate the overall applicability and role of prone RP surgery in treating benign renal lesions in children. We therefore present our 10-year experience with prone RP total, partial, and bilateral nephrectomies in children of all ages with benign renal disease. This is the largest series to date examining RP renal surgery, complete with age- and procedure-matched comparisons with an open control group.
Patients and Methods
After obtaining appropriate Institutional Review Board approval, we performed a retrospective analysis of medical records of children undergoing benign renal surgery from 2001 to 2010 at a single tertiary children's hospital. Exclusion criteria included patients undergoing surgeries with a malignant renal pathology, living donor nephrectomies, transplant nephrectomies, and transperitoneal laparoscopic renal surgeries.
All of the prone RP surgeries were performed by a single surgeon (LJC), using a Visiport for direct access and two additional 5mm ports. The surgical technique is discussed in detail in Figure 1 and is modified from Borer and associates. 7 The open surgeries were performed with the patient in the flank or supine position by one of the experienced pediatric urologists at our institution.
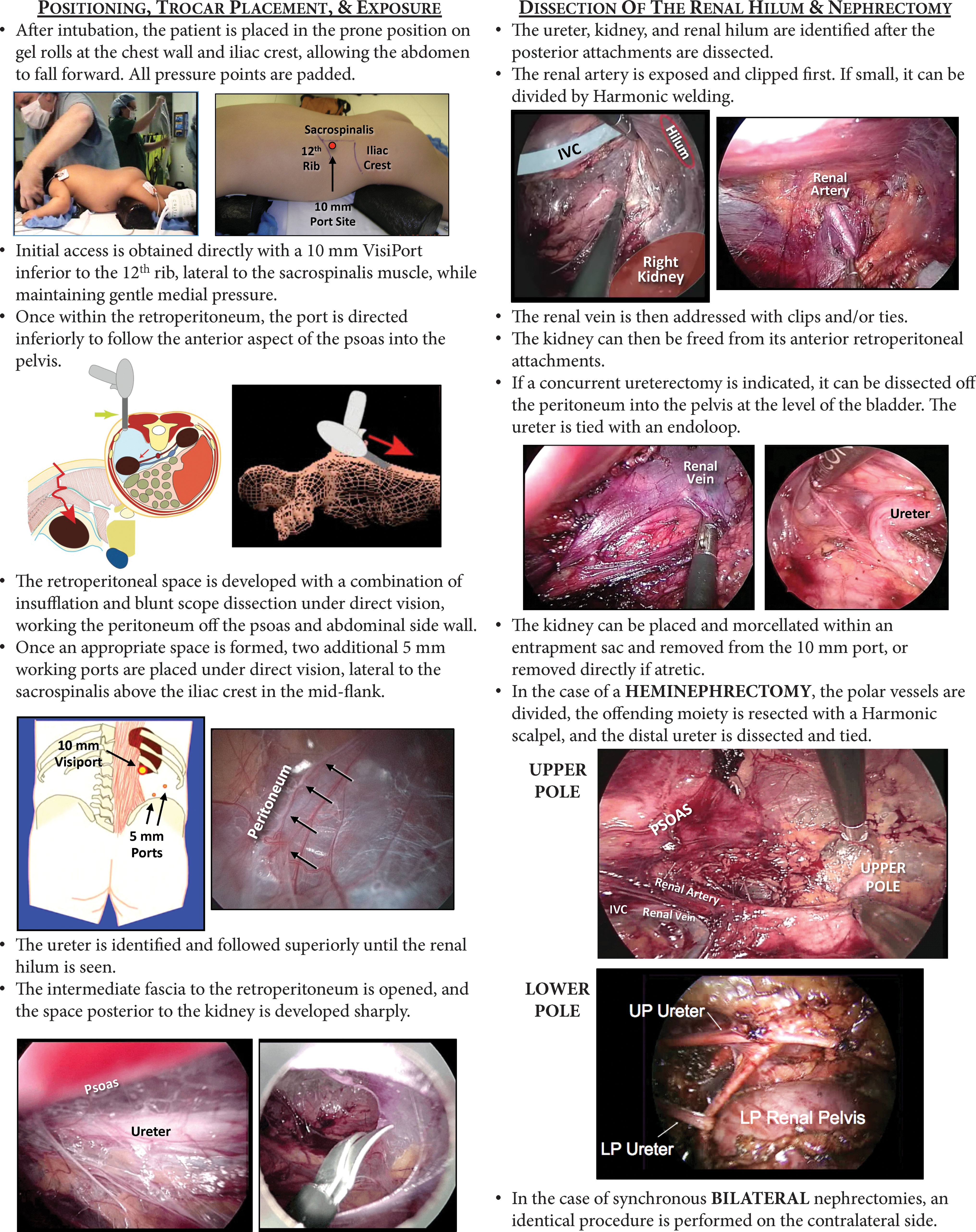
Surgical technique.
Patient demographics, comorbidities, clinical presentation, principal diagnosis, operative procedure, hospital course, and complications were recorded. Complications were defined as those potentially related to the nephrectomy performed. These were subdivided into intraoperative, perioperative (resulting in a prolonged hospital stay), and postdischarge complications (including emergency department admissions within a 30-day period), as well as those resulting in subsequent procedures.
Statistical analysis was then performed, using SPSS 16.0 (Chicago, IL). Chi-square and Fisher exact tests were used for categorical data. The Mann-Whitney comparison was used for nonparametric numerical data, and t-tests were used for comparison of parametric data. Analysis of variance and Bonferroni analyses were used for comparison across groups. Alpha values of ≤0.05 were considered significant.
Results
Table 1 depicts a broad overview of the study population. There were 308 children who underwent prone RP (n=154) or open (n=154) total or partial nephrectomies for benign renal disease; 25 of the patients underwent synchronous bilateral procedures (20 RP, 5 open), resulting in the resection of 333 renal units.
UPJ=ureteropelvic junction; UVJ=ureterovesical junction; UTI=urinary tract infection; d=days; y=years.
Fifty-four patients underwent a major concomitant procedure at the time of surgery. These were defined as any reconstructive or extirpative peritoneal or retroperitoneal surgery, while cystoscopic procedures, circumcisions, orchiopexies, posterior urethral valve resections, and other extra-abdominal procedures were considered minor. Ureterocele resection and ipsilateral ureteral reimplantations were deemed separate major procedures, as were augmentation cytoplasties, diverticulectomies, and contralateral pyeloplasties.
Nineteen patients had hospital stays longer than 10 days. Seven were in the neonatal intensive care unit from the time of birth and were hospitalized with multiple comorbidities, four had bilateral nephrectomies with transplant- or dialysis-related complications, and two were managed by the nephrology team for dialysis initiation; these patients were excluded from each of the LOS analyses. The remaining six patients were included.
The study population was initially divided into those undergoing either RP or open renal surgery, as shown in Table 2. Patients who were undergoing RP surgery at our institution were significantly older with a greater number of comorbidities. The RP group had a significantly higher percentage of patients who were undergoing bilateral procedures and significantly fewer patients who were undergoing an additional procedure, compared with the open group. There were no differences between groups based on clinical presentation, principal diagnosis, or complication rates. Of note, there were no conversions from the RP to the open approach.
RP=retroperitoneoscopic; UTI=urinary tract infection; EBL=estimated blood loss.
Given the likelihood that additional major procedures confounded patient outcomes, patients who were undergoing concomitant procedures or bilateral nephrectomies were excluded from the next two sets of analyses. Patients in both the RP and open groups were categorized into a total nephrectomy group (86 RP, 52 open) and a partial nephrectomy group (30 RP, 61 open). To control for the disparity in age between the RP and open cohorts, patients were further subdivided based on age (<3 years vs ≥3 years). Figure 2 provides a schematic of the study groups, and Tables 3 and 4 provide a more comprehensive comparison of the subgroups.

Overview of the study population.
Patients undergoing bilateral and additional procedures were excluded.
RP=retroperitoneoscopic; EBL=estimated blood loss.
Patients undergoing bilateral and additional procedures were excluded.
RP=retroperitoneoscopic; EBL=estimated blood loss.
Total nephrectomy analysis
Table 3 compares all subjects undergoing a unilateral total nephrectomy. For patients <3 years old, there were no differences in patient characteristics, principal diagnosis, estimated blood loss (EBL), operative times, or complications between the RP and open groups. One patient in the open group returned to the operating room for repositioning of his PD catheter, which was dislodged during the previous surgery. The RP group was found to have a shorter LOS (1.03 vs 1.63 d; P=0.001) than did the open group.
Similar results were found in patients ≥3 years old who were undergoing RP total nephrectomies—they were older with a significantly decreased LOS (1.52 vs 2.31 d; P=0.003). Otherwise, there were no differences in study parameters. The RP group had one intraoperative complication (deserosalization of the small bowel during kidney morcellation), two postdischarge complications (pyocystis and fevers related to a fluid collection), and one complication-related procedure (drainage of the fluid collection). There were no complications in the open group, but complication rates between groups were not significantly different.
Partial nephrectomy analysis
Data comparing RP and open patients undergoing partial nephrectomies are shown in Table 4. In both age groups, the RP group had a shorter LOS and longer operative times. Despite being subgrouped by age, the RP group was overall older than the open group in both age cohorts. The <3 year-old RP group had one postdischarge complication—an upper pole ureteral obstruction that necessitated prone RP ureterolysis. The open group had six perioperative complications (six febrile culture-proven urinary tract infections [UTIs]), three postdischarge complications (sepsis, UTI, and atrophy of the remaining kidney remnant), and one complication-related procedure (ureterocele excision). In children ≥3 years who were undergoing partial nephrectomies, complication rates were not significantly different. There was one postdischarge UTI in the RP group. For the open group, there was one intraoperative complication (venotomy, necessitating immediate repair), one perioperative complication (UTI), three postdischarge complications (two UTIs and sepsis), and two complication-related procedures (endoscopic ureterocele incision and distal ureterectomy with marsupialization of an ectopic ureter).
Bilateral nephrectomy analysis
A separate analysis was performed for patients who were undergoing bilateral synchronous nephrectomies (Table 5). There were 20 patients in the RP group, and 5 in the open group, and patients with concomitant procedures were included in this group, given the small numbers. It is important to note that the bilateral comparison was hindered by discrepancies in sample size, concomitant procedures, and combinations of total and partial nephrectomies. The open bilateral group was more likely to undergo a concomitant procedure (P=0.02). The RP group had 19 bilateral total nephrectomies and 1 bilateral partial nephrectomy, while the open group had 3 bilateral total nephrectomies and 2 combined total and partial nephrectomies. Despite these confounding variables, there were no differences in patient characteristics, operative times, complication rates (intraoperative, perioperative, or postdischarge), and hospital LOS between groups. LOS in bilateral patients was dominated by issues that were related to their anephric state and comorbidities rather than intrinsic to surgery (open or RP).
RP=retroperitoneoscopic; PD=peritoneal dialysis.
In the RP group, one patient had a perioperative complication (a transplant UTI), and three patients had postdischarge complications: Two patients had bilateral incisional hernias, and one had a unilateral incisional hernia, all from the 10mm port sites. Of interest, the two patients with bilateral hernias had been restarted on PD the day after surgery. All three patients underwent definitive operative repairs without event. There were no complications in the patients who underwent bilateral open nephrectomies.
Resumption of peritoneal dialysis
There were 13 patients on PD at the time of surgery who underwent 21 total nephrectomies (8 bilateral RP, 3 unilateral RP, 2 retroperitoneal unilateral open) who were on PD at the time of surgery. PD was resumed in an average of 1.13 days after RP surgery (range 0–3 d) and 1 day after open surgery. In the RP group, there was one peritoneotomy noted intraoperatively; the patient restarted his PD one day postoperatively without any complication.
Effect of experience on operative time and outcomes
We sought to determine whether outcomes in the RP arm evolved over the 10-year course as a result of surgical experience. The RP group was again divided into total and partial nephrectomy groups. Both groups were then subdivided into early (2000–2004), intermediate (2005–2007), and late cohorts (2008–2010). For the total nephrectomy group, there were 30 patients in the early group, 32 in the intermediate group, and 24 in the late group; for the partial nephrectomy group, there were 10 patients in each of the groups.
There were few differences in both the total and partial nephrectomy groups over time. The mean operative times significantly decreased (2:51:00 in the early, 2:11:00 in the intermediate, and 1:47:00 in the late groups. P=0.005) in the total nephrectomy group, but this did not hold true for the partial nephrectomy group (2:57:00, 3:10:00, 2:32:00, respectively. P=0.481). Patient comorbidities, EBL, and complication rates were also similar across time for both total and partial RP nephrectomy groups.
Discussion
We present our 10-year experience with prone RP and open renal surgery in children. On initial analysis, the RP group appears older with fewer concomitant procedures. The difference in age between groups may reflect an institutional practice of referring older patients to laparoscopic procedures. After controlling for age and concomitant procedures, however, our data suggest that the RP approach is comparable to the open approach in terms of efficacy and safety. There were no differences in complication rates, and while operative times were significantly longer in the RP arm of the partial nephrectomy analysis, hospital LOS was significantly shorter among both total and partial nephrectomy RP groups than in the open groups. In a separate analysis that focused on patients undergoing bilateral RP and open nephrectomies, there was no difference in operative times or complication rates between groups.
Despite the increased operative times in the partial nephrectomy analysis, we believe that the RP approach still carries several advantages over the open approach. In both total and partial nephrectomy analyses, the hospital LOS was significantly shorter, signifying a faster recovery time. Although our study did not address the issue of postoperative pain, previous reports have demonstrated that the analgesic requirements are decreased with a laparoscopic approach. 12 Cosmesis is arguably superior after laparoscopic renal surgery, with three small port sites (10 mm, 5 mm, 5 mm), compared with the larger incision needed in the open technique.
In the bilateral nephrectomy comparison, there was a large difference of operative times between the RP and open group (4:37:00 vs 2:33:00, respectively), which did not reach statistical significance (P=0.11). This was likely because of the discrepancy in sample sizes, surgical procedures (bilateral total, bilateral partial, and combined total and partial), and wide variance. There were two open bilateral total nephrectomies with operative times ≤2 hours, which skewed the comparison, and each was performed through a wide chevron incision because of concomitant liver transplants. It should be noted that in these cases, operative time did not include closure of the incision. Even if the larger incision improved operative times, it did so at the cost of patient morbidity.
We favor the prone RP approach because of the direct access to the kidney and renal hilum, the natural traction on the renal vessels from gravity, and avoidance of intraoperative repositioning when performing bilateral nephrectomies. By remaining extraperitoneal, the RP approach also decreases the risk of injury to the intra-abdominal organs (bowels, liver, spleen), postoperative intra-abdominal adhesions, postoperative ileus, and intraperitoneal contamination from the renal surgery, while obviating the need for bowel retraction. 13 Concerns about resuming PD are also minimized in this approach. Finally, we believe that a more complete ureterectomy can be accomplished with the RP approach than with the open approach—the ureter can be resected to the level of the iliac vessels through a single open incision, but can be taken down to the level of the bladder in females and the vas deferens in males using the RP technique. The more extensive ureteral dissection may also contribute to the longer operative times seen in the partial nephrectomy arm.
The mean operative times in the RP total nephrectomy group improved significantly over the course of the study, although this finding was not seen in the RP partial nephrectomy group. Over the 10-year period in which RP surgery was performed, surgical techniques varied slightly as experience accumulated. Although the initial direct access remained constant in both device and positioning, there was greater flexibility with the working ports over time. Two 2mm or 3mm ports were initially employed, necessitating frequent interchanging of instruments to allow for the use of the Harmonic scalpel and laparoscope; consequently, 5mm ports are now more consistently used. The positioning of the working ports has also been modified over time; the medial port has shifted inferiorly, and the lateral port is also arced inferiorly. These changes have allowed for greater access to the entirety of the retroperitoneum, facilitating dissection and exposure of the distal ureter.
There were no open conversions in the RP group, and complication rates did not vary in any of the comparisons between the RP and open groups. The low complication rates can be attributed to the rigorously held surgical techniques as described in Figure 1. In the total nephrectomy group, a deserosalization of the small bowel occurred during kidney morcellation but was noted and repaired at the time of injury, preventing further morbidity to the patient. In the perioperative period, a patient receiving PD was found to have pyocystis after removal of a nonfunctioning kidney, and another patient with a chronically infected kidney was found to have fevers related to a fluid collection in the surgical bed, which was effectively managed by drain placement by interventional radiology. In the partial nephrectomy group, one patient experienced an upper pole ureteral obstruction, necessitating prone RP ureterolysis. Another patient in the partial nephrectomy group presented with a nonfebrile UTI, as did a renal transplant patient in the bilateral nephrectomy group, both of whom were treated with antibiotics. In the bilateral nephrectomy group, three patients experienced incisional hernias at the 10mm port sites despite meticulous closure of the fascia at the time of surgery. Each had a history of multiple comorbidities (including chronic renal disease, PD, steroid use, and nephrotic syndrome-driven malnutrition), yet it was difficult to surmise the exact cause of the herniation. They each underwent definitive surgical closure without further complication.
Our complication rates differ from some of those published in the literature. One study on RP partial nephrectomies claimed a high open conversion rate, increased in younger patients, which contrasted with our experience. 17 Other groups have reported an increased risk of urine leak, hemorrhage, and loss of the ipsilateral renal moiety in RP heminephrectomies, 17,18 although we have yet to witness these complications. Atrophy of the kidney remnant was, however, observed in one patient in our open partial nephrectomy group.
The goal of our study was to compare the outcomes of patients undergoing RP and open total and partial nephrectomy with the fewest confounding variables possible. Critical to this endeavor was the exclusion of concomitant procedures from analysis, with a separate subgroup analysis of patients undergoing synchronous bilateral nephrectomies. We used our larger sample size to corroborate the findings of the existing literature—we found that the prone RP approach is associated with similar complication rates and a shorter LOS in children, compared with the open approach. 14 –16 We do not attribute the similar LOS in patients undergoing RP and open bilateral nephrectomies to the type of surgery undergone, given the treatment decisions made by the primary nephrology team regarding institution of dialysis, monitoring of blood pressure, and transplant-related management.
Furthermore, our study was bolstered by subgrouping patients based on age. Many of the benefits of laparoscopic surgery are usually described in the older population in which an open incision can be associated with a greater morbidity. Our data support that the RP approach is comparable to the open approach even in younger children, as shown by the similar complication rates. Although the operative times were longer, LOS and EBL were significantly less in the younger population of the RP partial nephrectomy group. It should be noted that an effort to remove the entire extravesical ureter was made in the RP group, while the open nephrectomies had limited ureterectomies because of the single incision.
Our experience with patients on PD aligns with that of the published literature. 9,10 PD can be resumed safely in the early postoperative period in patients undergoing a retroperitoneal nephrectomy, even in the case of a small peritoneotomy.
Despite our best efforts to create a sound comparison between the RP and open approach, there are several limitations to our study. This is a retrospective analysis that examines data over the past decade, and follow-up data are limited in some patients. In this series, there is a referral bias for patients who are older and with more comorbidities to undergo RP procedures and for younger patients to undergo open procedures. Although we actively controlled for these factors, the comparison may be complicated by this selection bias. Nevertheless, we clearly show that the RP approach is a suitable option in all age groups and may lead to a clinically significant shorter LOS.
Conclusions
Prone RP renal surgery for benign renal disease compared favorably with open surgery in all ages. Complication rates between the open and RP groups were similar in all analyses (total, partial, and bilateral nephrectomies). RP partial nephrectomies were associated with longer surgical times, but the RP approach had a significantly shorter LOS across all age groups for total and partial nephrectomies. The prone RP approach should be considered a viable option for patients who are undergoing benign renal surgery at any age.
Footnotes
Disclosure Statement
No competing financial interests exist.