
Abstract
Flat-panel detector CT (FD-CT) provides cross-sectional CT-images while offering an improved workspace using fluoroscopic guidance for thermal probe placement such as for radiofrequency ablation (RFA) needles and thermal sensors. The purpose of this article is to test the feasibility of FD-CT in the application of renal tumor ablation in a “hybrid operating room” environment. Eleven patients with renal masses diagnosed preprocedurally with contrast-enhanced CT scan underwent core biopsy and simultaneous CT-RFA under general anesthesia with FD-CT guidance in the cardiac catheterization laboratory. Scans were taken preablation for tumor targeting, intermittently for probe placement and guidance of temperature sensors, and postablation. Perioperative and postoperative outcomes, pathologic results, and radiographic follow-up were recorded for each patient. Target temperatures >60°C to guide treatment end point were reached for each tumor periphery. Biopsy pathology showed 6/11 (55%) to be renal-cell carcinoma, and 2/11 (18%) to be benign; 3/11 (27%) had an indeterminate biopsy result. Three Clavien grade I complications occurred. One patient showed evidence of recurrent disease on postoperative CT scan. In our experience, we have found FD-CT–guided ablation of small renal tumors to be feasible using this advanced targeting system.
Introduction
Despite current advancements, needle placement guidance still has room for improvement. Using standard CT platforms for renal tumor ablation necessitates that the operator create a mental image of the three-dimensional (3-D) relationship between the tumor, adjacent structures, and needles. If the needle path is not in a direct line with the scanning slice, assumptions are made as to where the exact probe tip lies and may result in targeting errors.
Flat-panel detector CT (FD-CT) allows manipulation of the axial, sagittal, and coronal images to create visualization along the plane of the needle for optimal placement. Multiplanar capability allows planning of needle trajectory across one or more planes using “down the barrel technique.” We present a cohort of 11 patients who underwent percutaneous RFA for renal mass treatment with needle guidance via FD-CT with 3D reconstruction to assess the feasibility of FD-CT.
Patients and Methods
This study was approved by an Institutional Review Board. Eleven patients who received a diagnosis of renal tumors via enhancement on contrasted CT scan from January to September 2010 were offered CT-RFA based on tumor size, anatomic location, patient comorbidities, and patient preference. Tumors with clearly defined borders were primarily selected. Patients received counseling on currently available treatment options and the risks and benefits of FD-CT RFA. Eleven renal tumor ablations were performed under general anesthesia with guidance from the FD-CT system.
The Siemens Artis Zee Biplanar System with DynaCT® software is a C-arm–based four-panel scanner that provides cross-sectional CT images while offering an improved workspace and two-dimensional fluoroscopic guidance for radiofrequency (RF) probes and thermal sensors. Scans were taken preablation for tumor targeting (Fig. 1), post-RFA probe placement (Fig. 2), and postablation (Fig. 3). All scans were performed with the physician behind protective lead glass. Patients were positioned prone with arms tucked by their side, and preliminary scanning was performed without the use of intravenous contrast. Preoperative scan image fusion was not available for use but would also help cut down on exposure time.
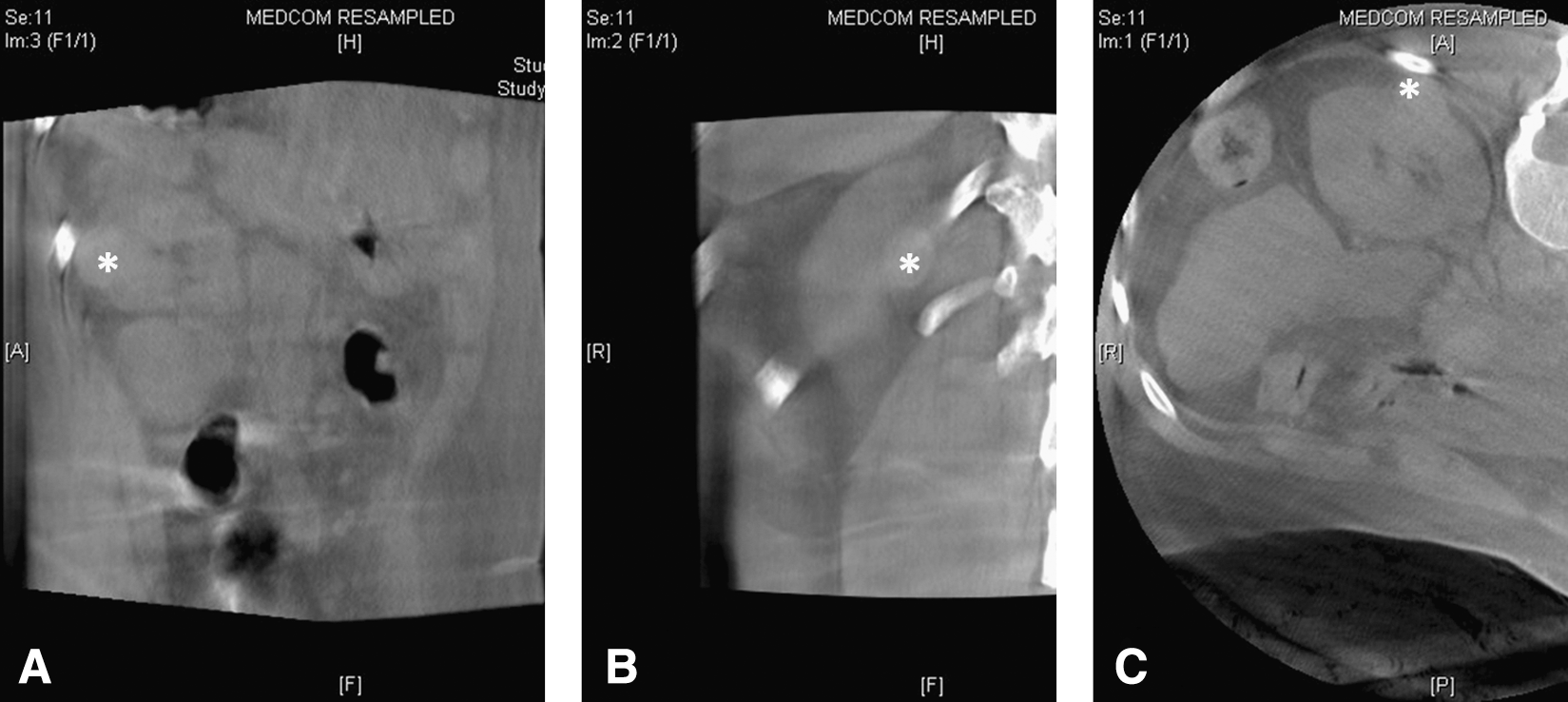
Preablation scan. Three-dimensional image reconstructions of the renal tumor before ablation with white asterisk in tumor center in the sagittal
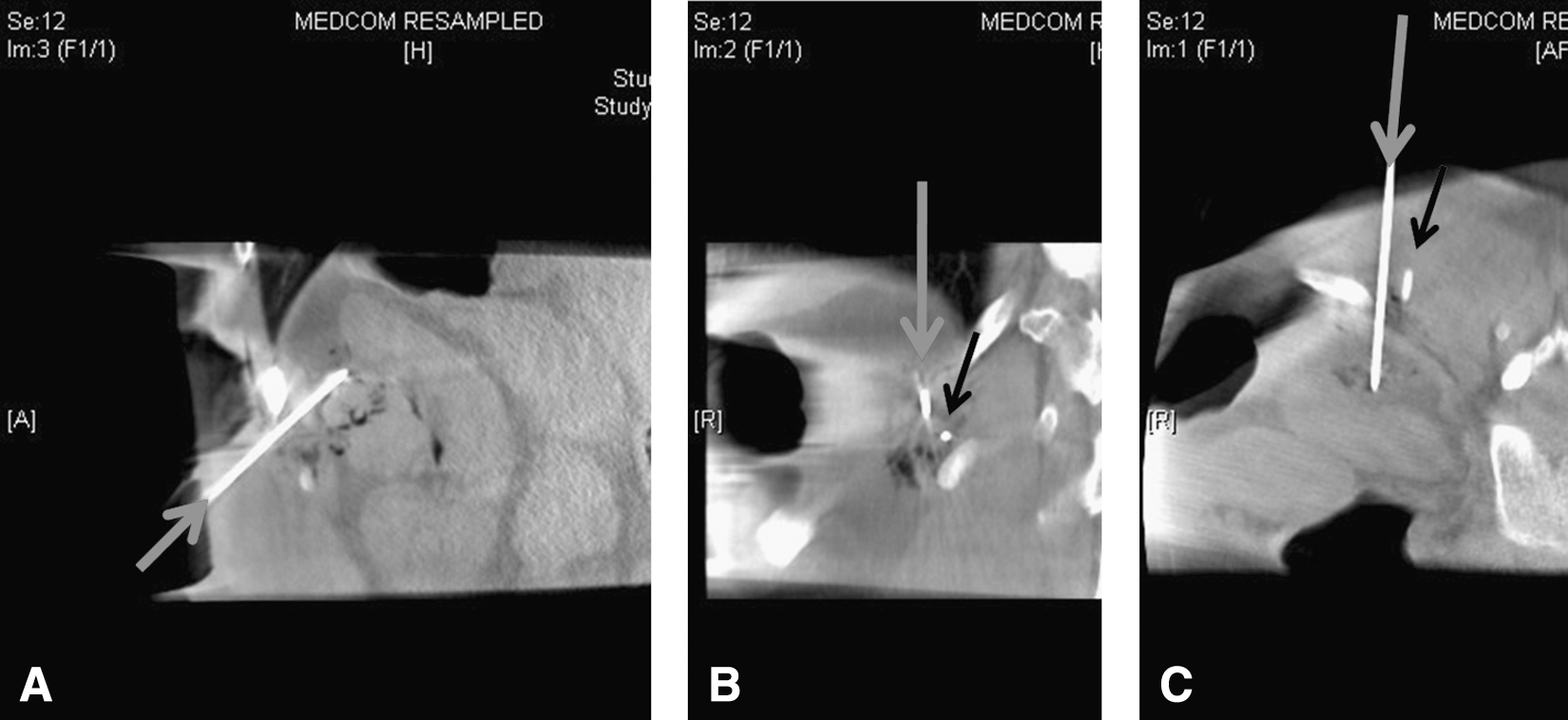
Placement of radiofrequency ablation (RFA) needle. Three-dimensional image reconstructions of the renal tumor before ablation with RFA needle and peripheral thermometer sheath in place are shown in the sagittal
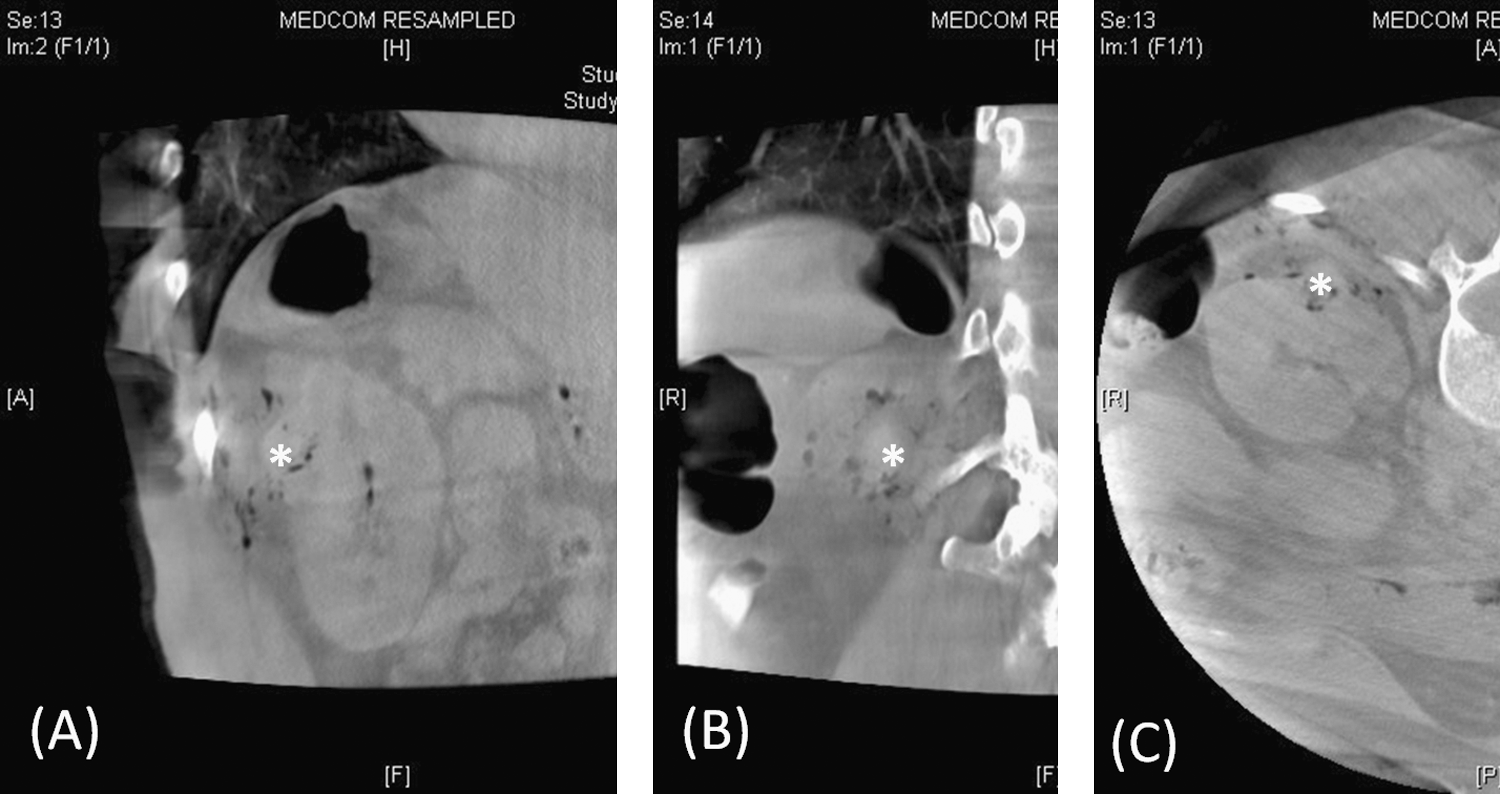
Postablation scan. Three-dimensional image reconstructions of the renal tumor before ablation with white asterisk in tumor center in the sagittal
After visualization of the target tumor, a treatment plan for placement of probe, biopsy needle, and peripheral thermal sensors was created by the ablation team. Fiberoptic thermal sensors (Lumasense, Santa Clara, CA), which we routinely use to help determine end points of treatment, were placed 5 mm from the tumor margin with CT-image manipulation using a coaxial guide needle with radiopaque sheaths (Yueh, Cook Vascular, Inc, Vandergrift, PA). An example is shown in Figure 4. Before ablation, several 16-gauge core biopsies (2–5) were taken for permanent histologic staining.

Needle positioning. The RFA needle is referenced by a blue arrow. Placement of the RFA needle and peripheral thermometry in the skin
One or two 3-cm Cool-tip™ water-perfused ablation probes (Covidien Inc, Boulder, CO) were advanced into the tumor and RFA commenced with simultaneous peripheral fiberoptic thermometry to determine treatment end points of >60°C. Ablation times varied with each case and were based on reaching temperature end points. Three cases needed probe repositioning because the temperature goals were not reached after one cycle.
Results
A total of 11 patients had FD-CT RFA of their renal masses including 4 females and 7 males. Mean tumor size was 2.5 cm (range 1.1–3.3 cm) with six left-sided and five right-sided lesions, and tumors in various kidney locations (four upper pole, five interpolar, two lower pole). Intraoperative core biopsy revealed 55% (6/11) renal-cell carcinoma (RCC), 18% (2/9) nonmalignant (1 angiomyolipoma, 1 oncocytoma), and 27% (3/11) “nondiagnostic” (two normal renal tissue, one necrotic tissue). RCC subtypes were clear-cell (n=2, Fuhrman grade 1-2), papillary (n=3), and chromophobe (n=1, Fuhrman grade 2).
One to four thermal sensors were used, and one or two probes were used during ablations as determined by tumor size and location. Eight of 11 ablations needed only one ablative probe deployment, while three necessitated repositioning (two deployments) to achieve the intraoperative target temperature (periphery) >60°C.
There were no perioperative complications. There were three Clavien grade I postoperative complications (one dysuria, two acute urinary retention). Mean clinical follow-up time was 3.6 months (0.5–9 mos) with postoperative contrast-enhanced CT performed on all patients at a mean of 1 month postoperatively (Fig. 5); two patients had scans at 6 months. One patient demonstrated minimal enhancement at the periphery of the ablation zone on follow-up contrasted CT scan, and reablation is planned. All other patients showed no radiographic evidence of enhancement on follow-up.
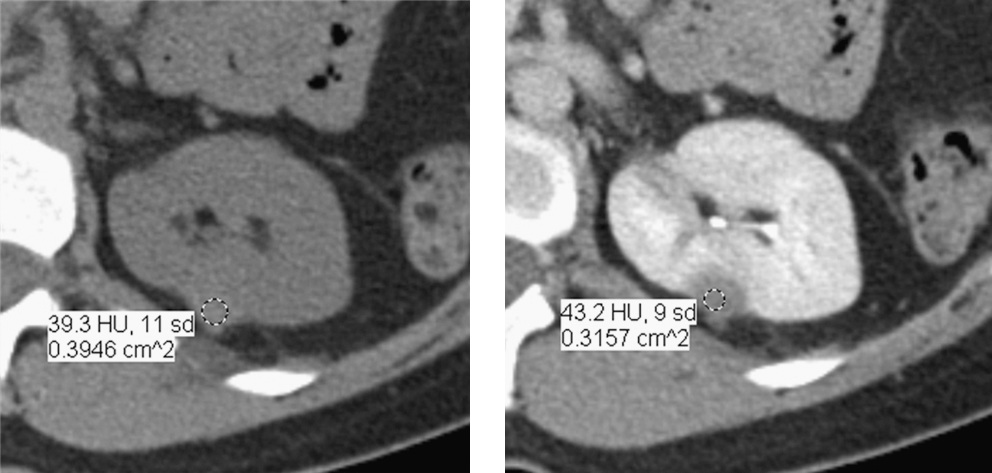
Follow-up scan. CT scan showing follow-up imaging of ablated area precontrast (left) and excretory phase postcontrast (right) with Hounsfield units (HU) increasing from 39 HU to 42 HU postcontrast administration.
Discussion
We used the FD-CT system to aid in guidance of needle ablation probes and fiberoptic peripheral thermal sensors in a cohort of 11 patients with mean renal tumor size of 2.5 cm. FD-CT with 3D reconstruction has reported use in other medical specialties, 6,7 but this is a novel use in RFA of renal tumors. This series did include one patient with radiographic failure. It is unclear whether the source of the failure is the imaging guidance system used, failure of RFA, inaccurate temperature monitoring, or simply small sample size.
The purpose of using ultrasonographic or CT guidance during RFA is to spatially place the ablation probe to allow creation of a thermal field during deployment that encompasses the entire tumor and achieves adequate tumoral temperatures. 1 To achieve complete tumor ablation, the ablation zone of the RF probe should encompass the entire tumor and a small margin surrounding the tumor. This necessitates precise probe placement. Misplacement of the probe in any sagittal, coronal, or axial coordinate can cause incomplete ablation. If the treatment end point is not attained, multiple or larger ablation probes are typically needed, but result in less NS.
Accuracy of peripheral thermal sensor placement in heterogenous tissues such as the kidney is important because ablation zones may be nonuniform, 8 and temperature monitoring helps to ensure uniform tumor ablation. 4 Misplacement of the thermal sensors closer to the ablation needle than intended could result in falsely elevated temperature monitoring, resulting in incomplete ablation. On the other hand, more distant placement of the temperature sensor from the ablation needle than intended can cause inaccurately low temperature readings, resulting in unnecessary removal and repositioning of the ablation needle and additional healthy tissue ablation with additional nephron damage.
The advantage of a FD-CT system and conventional CT systems with 3D reconstruction software is the rapid availability of reformatted images in multiple planes. The FD-CT system allows reorientation of any plane (Fig. 4), where the axial plane is rotated to include the entire probe length, clearly defining the exact tip of the needle/probe. Once a needle or sensor is placed and images taken, the position can be determined in 3D space in a continuous fashion. 3D reconstruction software currently exists for conventional CT as well but is underused.
Improved planning and better guidance across multiple planes may result in fewer total scans. Conversely, FD-CT produces a narrower image field when compared with conventional multidetector CT, which can scan from chest to pelvis in one breath hold. Proper alignment with preoperative scan reference can lead to a reduced number of scans, which relates to the procedure time.
One important limitation of the FD-CT technique is lower contrast resolution and increased streak artifacts compared with the conventional CT. This technique should be used initially for well demarcated, predominantly exophytic lesions if one wishes to avoid the use of intravenous contrast during the ablation procedure. For deeper lesions, a contrast-enhanced study should be used to better differentiate the tumor margin from the adjacent normal renal parenchyma.
When using FD-CT, the patient is stationary, and the wide aperture allows easy access to the patient without the need to be inside the CT gantry. Optimal resolution is obtained when the target (tumor) is positioned in the isocenter of the C-arm rotation, which may limit our ability to perform this technique on large or obese patients because the input field of view is 30 cm×40 cm.
FD-CT is a new technology with no reported clinical application to the field of urology. It has been used primarily in IR and invasive cardiology arenas. Its use in the guidance of ablation probes and temperature sensors represents a novel use in RFA of renal masses, and application in endourology. A potential advantage over traditional spiral CT is improved ergonomics from increased surgical workspace and potential for more rapid ablation times because the probe placement is facilitated with the use of 3D spatial targeting augmented with real-time low-dose fluoroscopy to advance needles without the need for the radiologist to leave the bedside and scan from behind a leaded shield, and make fine tune adjustments with repeated scans inside the conventional CT gantry. This is also unlike CT fluoroscopy, which has very high exposure to physician and support staff such as anesthesiologists and nursing staff.
We present an initial case series demonstrating the feasibility of the use of FD-CT for the performance of percutaneous guided RFA of renal masses. To determine the equivalency of FD-CT and conventional CT in the guidance of tumor ablation probes, further prospectively randomized studies are warranted. The technique presented is experimental and was performed as a feasibility study.
Conclusion
The technique of CT-guided, percutaneous RFA of solid renal masses can be improved on. Use of the FD-CT in the cardiac catheterization laboratory as used in this study aids the procedure with (1) treatment planning using multiplanar views; (2) guidance and localization of probe/needle tips when “in-line” viewing is used; and (3) improved work space environment because of open C-arm access. FD-CT proves to be a safe and feasible guidance system for percutaneous RFA. It may have a role in performing ablative therapies in the hybrid operating room environment. Future prospective studies are needed, however, to assess its targeting ability and total radiation exposure.
Footnotes
Acknowledgment
We would like to thank Kymberlee Manni, R.N., Ph.D. and Mr. George Benelli for assistance in facilitating this project.
Disclosure Statement
No competing financial interests exist.