
Abstract
Background and Purpose:
Percutaneous nephrolithotomy (PCNL) is considered standard therapy for large and complex renal calculi. The optimal patient position and puncture site for collecting system access remains controversial. This purpose of this retrospective review is to analyze our PCNL series with respect to puncture tracts, success, and complications using our novel prone-flexed position.
Patients and Methods:
Perioperative data were collected on consecutive PCNL cases for renal calculi performed in the prone-flexed position from 2004 to 2009. Patient demographic, stone, operative, postoperative, and follow-up data were collected. Successful treatment was defined as stone free or sandlike (≤1 mm) particles visible on CT scan at 3 months.
Results:
A total of 318 patients, with a mean age of 52.9 years and body mass index of 27.8 kg/m2, underwent PCNL in the prone-flexed position (57.9% male). Sixteen tracts were above the 11th rib, 138 were above the 12th rib, and 164 were infracostal. Multiple tracts were used in 16 patients. There were no significant differences between patients undergoing supracostal vs infracostal puncture with respect to side, stone area, number of tracts, number of stones, or the presence of staghorn or struvite calculi. Success in the supracostal group (89.8%) was not statistically different from the infracostal group (94.1%), P>0.05. Overall complication rates across groups was low (11.6%), with a significant difference in complications between the supracostal and infracostal puncture groups across Clavien grades, P<0.01. No patients needed blood transfusions or angioembolization.
Conclusion:
Regardless of supracostal or infracostal renal access, our novel prone-flexed position assists with percutaneous renal access and ease of nephrolithotomy, while maintaining excellent success rates and minimizing procedural morbidity.
Introduction
While the prone position is generally considered standard for PCNL, there have been several position modifications including the lateral decubitus position, 7 modified lateral, 8 reverse lithotomy, 9 split leg, 10 and the supine Valdivia position. 11 Each of these positioning modifications impacts the relative anatomy of the kidneys and surrounding structures, thus possibly altering the incidence of the various procedural-related complications. This current study follows from an earlier article published by our group examining the relative renal anatomy on abdominal CT images of patients in the supine, prone, and prone-flexed positions, which concluded that the prone-flexed position lowers the kidneys in relation to the chest, while providing improved access to the upper pole, facilitates access and the movement of instruments during lower pole PCNL. 12
Although success rates after PCNL range from 75% to 95%, periprocedural and intraoperative complication rates of up to 83% have been described. 13 Although major complications are relatively rare and include, but are not limited to, septicemia (0.3%–4.7%), 14 –17 colonic, spleen, liver (0.2%–0.8%), 2,14,18,19 or pleural injuries (0%–3.1%), 2,14,18 minor complications are relatively common and include urinary extravasation (7.2%), 14 –17 transfusions (0.8%–17.5%), 14,16,20,21 and fever (21.0%–32.1%). 13 –15,17,22 Complications are sometimes categorized temporally, based on the various parts of the procedure (ie, obtaining access, stone removal, etc), or based on whether they are considered major or minor complications. With the increased interest in the urologic literature on harms and complications, coupled with the inherent biases associated with gross categorization of complications as major or minor, however, urologists have been turning toward the Clavien classification system to define their procedure-related complications. 23
Originally proposed in 1992, the Clavien classification system is a universal classification system based on therapy-oriented severity grading of complications after general surgical procedures. 24 Various groups have since adopted the classification scheme for urologic procedures, including PCNL, 25 thus standardizing the reporting of complications to facilitate comparisons within and between different centers and treatment modalities. The current study examines the success and morbidity in a series of consecutive patients who were treated with PCNL in our novel prone-flexed position, while specifically comparing supracostal with infracostal renal punctures.
Patients and Methods
A retrospect review identified 318 consecutive patients who underwent PCNL at a single tertiary-care academic center from May 2004 to June 2009. Patient demographics, stone, and operative information were documented prospectively. Postoperative information, including length of stay, complications, auxiliary treatments, stone composition, postoperative drop in hemoglobin level, and need for transfusions were recorded.
Prone-flexed positioning
Once retrograde access is obtained, a ureteral occlusion balloon is inflated at the ureteropelvic junction and secured to a Foley catheter. The patient is repositioned prone with adequate padding under the pressure points of the head, chest, knees, and feet. The anesthetist places ocular padding to prevent corneal abrasion and supports the head and endotracheal tube with a 7" headrest pillow (Mizoho Osi, Union City, CA). To prevent brachial plexus injury, the arms are positioned below the level of the chest and are both externally rotated at the shoulder and flexed at the elbow.
In the prone position, the natural lordosis of the spine can lead to interference from the gluteal muscles with the rigid nephroscope when using a lower pole access. In an effort to minimize this, the table is flexed 30 degrees at the level of the patient's midlumbar region to open the space between the 12th rib and the posterior iliac crest (Fig. 1), dropping the gluteal muscles from the working plane. Flexion of the patient not only flattens the back, but it also increases the working space on the patient's flank. Furthermore, this prone-flexed position also results in inferior displacement of the kidneys in the retroperitoneum and rotates the ribs cephalad to increase the potential working space and may convert an otherwise supracostal to an infracostal puncture, or a super-11th rib access to one above the 12th rib.

Comparison of the supine to prone-flexed position before percutaneous access and stone removal.
Procedural technique
All PCNL procedures were performed by one of two urologists (RJH, KTP) in a teaching environment using the same technique under general anesthesia with the patient in the prone-flexed position. Percutaneous access was obtained at the time of surgery by the operating urologist in all 318 cases, without assistance from interventional radiology or ultrasonographic guidance. Based on the stone location, size, burden, and pelvicaliceal anatomy, the site of caliceal entry and number of access tracts were chosen at the procedure's commencement. Because of the retrospective nature of this study, we cannot comment on the surgeon's rationale nor the indication for puncture location.
The architecture of the collecting system is delineated by contrast infused through the ureteral occlusion balloon catheter with the patient supine. Three images are captured: One in the anterior-posterior plane and two 30-degree oblique images. Comparing these images gives a three-dimensional appreciation of the collecting system and the ability to choose a suitable posterior calix. A bull's-eye technique is used to gain access directly into the center of the papilla of the chosen calix, once the patient is placed in the prone-flexed position.
Once intrarenal access is obtained, the tract is sequentially dilated from 6F to 10F, and a safety guidewire is inserted using a dual-lumen catheter. Using the Ultraxx balloon dilator (Cook Urological, Bloomington, IN), the tract is dilated to 30Fr under fluoroscopic guidance, and access into the collecting system is confirmed by rigid nephroscopy. Once access is gained, a combination of the Olympus LUS-2 ultrasonic lithotripter and the Stonebreaker™ (Cook Urological) is used to fragment the stone, with occasional use of electrohydraulic or Holmium laser lithotripsy. Tri-radiate forceps (Storz) and a 2.4F or 4.5F N-circle nitinol tipless stone extractor (Cook Urological) are used to render the patient stone free. Careful flexible nephroscopy is used to confirm a stone-free state. An 8.5F to 6F nephroureterostomy tube (Cook Urological) is positioned in an antegrade fashion with a loop in the renal pelvis and a curl in the bladder. 26 All patients with supracostal access underwent fluoroscopy of the chest to exclude hydrothorax.
Postoperatively, the nephroureterostomy tube is capped on the first postoperative day, and the patient is typically discharged from the hospital. Patients remain on antibiotic therapy until the nephroureterostomy tube is removed at 1 week postoperatively. In no patients was a second-look nephroscopy performed. Because every calix is checked at the end of the procedure, residual stones were either within papillae or small and inaccessible via the available tract or tracts, where it was considered unreasonable to insert an additional tract.
Outcomes and statistical analysis
Complications were assessed using the original Clavien complications classification system. Successful treatment was defined as stone free or sandlike particles 1 mm or less in greatest diameter, as seen on radiography of the kidneys, ureters, and bladder 1 week postoperatively and subsequently on noncontrast CT at 3 months postoperatively. All data were analyzed with logistic regression, chi-square analysis, and analysis of variance, where appropriate, using SPSS 16.0 (Chicago, IL).
Results
Of the 318 consecutive patients undergoing percutaneous nephrolithotomy, 154 (48.4%) supracostal punctures were performed to gain access into the collecting system. Of those, 16 punctures were above the 11th rib with the remainder being above the 12th rib. There were no punctures in this recent series above the 10th rib, although this is occasionally necessary. Because of the low number of patients undergoing supra-11th rib puncture, those patients were combined with the supra-12th rib puncture to comprise the group of patients undergoing supracostal access. These were, however, analyzed separately. There were no differences between those patients undergoing supracostal vs infracostal puncture with respect to body mass index, age, patient side, stone size, or complexity of stone (Table 1). Of the single tract punctures into the upper pole calix (n=141), 21 (14.9%) were above the 11th rib, 96 (68.1%) were above the 12th rib, and 29 (21.0%) were infracostal. In addition, there were no differences in the number of additional tracts needed between the two groups, with an overall rate of 5.0% for secondary tracts. There were stones in a caliceal diverticulum in one patient in the supracostal puncture group, whereas two patients with infracostal punctures had stones in caliceal diverticula.
Data are expressed as mean±standard deviation or n (%), where applicable.
BMI=body mass index.
With regard to 88 (27.8%) full or partial staghorn calculi, 58.0% were accessed through a supracostal puncture, whereas 42.0% were managed through an infracostal access. For upper tracts with multiple stones, 43.6% were accessed through a supracostal puncture, whereas the remaining 56.4% were managed through an infracostal access.
Rigid criteria were used in determining success rates and stone-free status 2 weeks post-PCNL. The difference in success and stone-free rates was not statistically significant between groups (Table 2). There were no differences in the postoperative length of hospitalization (mean 2.4 d) nor in the rate of struvite stones managed in either group (mean 10.7%). Finally, there were no differences in the rates of auxiliary treatment, regardless of puncture site.
Data are expressed as mean±SD or n (%), where applicable.
SWL=shockwave lithotripsy; PCNL=percutaneous nephrolithotomy.
There were no significant differences in overall complication rates when comparing the group of patients who underwent a supracostal vs an infracostal puncture (Table 3 and Fig. 2). Overall, there were 37 (11.6%) complications, regardless of access. None of the 318 patients underwent blood transfusions. There was no difference in the relative increase in postoperative creatinine level, with a mean overall change of 10.3 μmol/L (standard deviation 16.3). Despite pleural complications being significantly higher in the supracostal group (P=0.038), the overall incidence was low at 3.2% of supracostal punctures. When further examined, only one of the five pleural complications was in the group of patients with a puncture above the 11th rib. The remaining four pleural complications were in those patients with an access directly above the 12th rib.
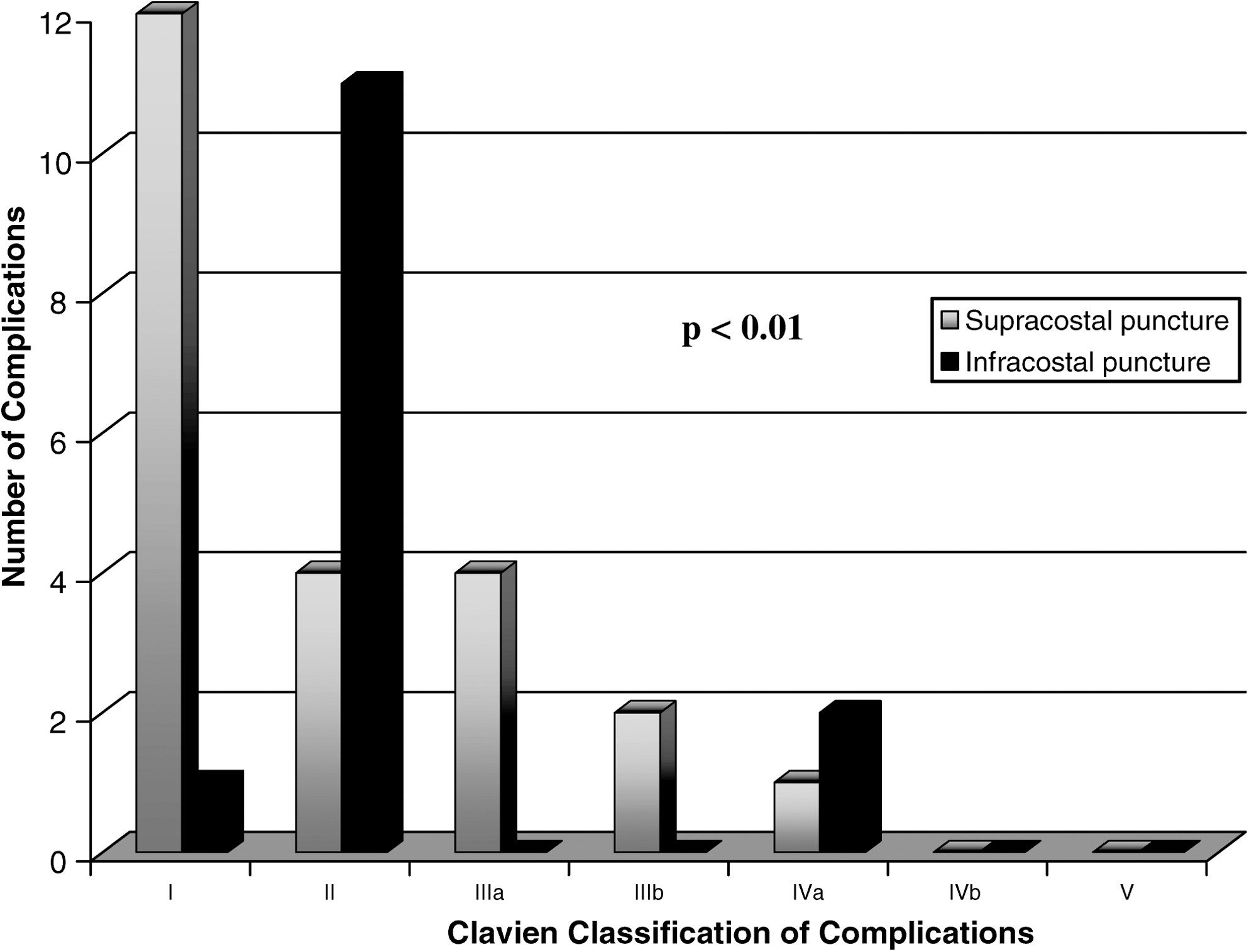
Histogram of Clavien classification of complications specific to supracostal and infracostal puncture.
Data are expressed as mean±standard deviation or n (%), where applicable.
Febrile infections were more common in infracostal punctures (P=0.043), with 5.6% of patients needing antibiotic treatment as opposed to prophylaxis postoperatively. Of the nine patients in the infracostal puncture group with infections, eight had urinary tract infections and one had pneumonia (Table 4). In neither group were there any injuries to the liver, spleen, colon, or any other adjacent organs. There were neither adverse events nor complications arising from being placed in the prone-flexed position for the length of the procedure.
Adapted from Ann Surg 2004;240:205–213.
NYD=not yet diagnosed; UTI=urinary tract infection.
When examining the complications as categorized by the Clavien classification system, grade I complications are considered minor risk events not necessitating therapy (excluding analgesic, antipyretic, antiemetic, and antidiarrheal medications). There were 12 events in the supracostal access group, whereas only 1 was seen in the those with infracostal punctures (P<0.01). Clavian grade II complications are those needing pharmacologic intervention with drugs not allowed for grade I complications, and there were 4 events in the supracostal access group and 11 events experienced by those in the infracostal puncture group (the majority of which were urinary tract infections (P<0.01).
Grade III complications are those necessitating surgical, endoscopic, or radiologic interventions. There were six grade III complications in the supracostal group vs none in the infracostal access group (P<0.04). Grade IV complications are life threatening and include either single or multiorgan dysfunction. There were three myocardial infarctions, with one in the supracostal group and two in the infracostal puncture group (P>0.05). This incidence of myocardial infarction is likely a reflection of the patient population who were treated in our tertiary referral unit for complex stone disease. Grade V complications are death, and there were none in our series. Table 4 shows specific complications seen in each Clavien category.
Discussion
With randomized controlled trials, such as the Lower Pole Study Group I demonstrating the effectiveness of managing larger stone with PCNL, 27 the procedure has become the treatment of choice for large, complex stones and for patients with upper tract anatomic anomalies. Over the past three decades, many refinements in both technique and patient positioning have improved the outcomes while decreasing the incidence of adverse events related to PCNL. Although major complications are quite rare, such as septicemia (0.3%–4.7%), 14 –16 colonic, spleen, liver (0.2%–0.8%), 2,14,18,19 or pleural injuries (0%–3.1%), 2,14,18 minor complications are more common and include urinary extravasation (7.2%), 14 –16 transfusions (0.8%–17.5%), 14,16,20,21 and fever (21.0%–32.1%). 13 –15,22
Because the rates of adverse events during PCNL remain relatively high, modifications to the procedure have been introduced in an attempt to limit the degree of perioperative morbidity. These recent technical advances include the use of balloon dilators during percutaneous renal access, 28,29 the injection of hemostatic agents into the nephrostomy tract, 30 assisting percutaneous access with the simultaneous use of retrograde ureteroscopy, 31 and the miniaturization of nephroscopes for use in the mini-PCNL. In an attempt to further facilitate the ease with which the procedure is performed and decrease the incidence of perioperative complications, there have been many modifications to patient positioning, including the lateral decubitus position, 7 modified lateral, 8 reverse lithotomy, 9 split leg, 10 and the supine Valdivia position. 11
Our modification in patient positioning is designed to not only decrease the morbidity of the procedure, but also to facilitate access and the manipulation of instruments during PCNL. The advantages of PCNL in the prone position, as opposed to supine, include access to the entire flank and the ease of access into the upper pole. The upper pole access is advantageous, especially in obese patients and in those with staghorn calculi or horseshoe kidneys, because it allows the surgeon to work down the renal access with minimal torque on the renal parenchyma and infundibula, thus decreasing the potential for renal parenychmal splitting and hemorrhage. Lastly, upper pole access is facilitated by the angle with which the kidneys are fixed by attachments within the Gerota fascia in the retroperitoneum, because the upper pole lies more medial and superficial to the skin, in comparison with the lower pole.
By modifying the prone to the prone-flexed position, the patient is flexed approximately 30 degrees at the level of the lumbar spine. The added advantages of this position include an increased distance between the posterior-superior iliac crest and the 12th rib, inferior displacement of the kidneys facilitating upper pole access (which may be converted to an infracostal from a supracostal access), and flattening the flank, which eliminates interference of the rigid nephroscope by the gluteal muscles during lower pole access. 12 There is the potential for position-related complications, however, including difficulty in maintaining the patient's airway and increased airway pressures. We have, on occasion, had to decrease the degree of flexion but never had to revert to the flat prone position. In addition, this position can cause prolonged elevations in intraocular pressures, leading to ischemic optic neuropathy 32 and brachial plexus injuries. 12 All of these complications, however, are also found in the flat prone position, and with the exception of the increased airway pressures, are not worsened in the prone-flexed position.
In reviewing the literature, it is apparent that there is no universal agreement on how to position a patient for PCNL or on how to perform the technical aspects of the procedure. Both positioning and technique may depend partly on the availability of specific instruments and operating tables as well as stone and patient-based factors. In addition, within the literature on PCNL outcomes, there appears to be a wide discrepancy in how perioperative adverse events are reported and categorized. Terms such as major and minor complications are widely subjective and are not standardized among surgeons nor institutions. In the era of pay-for-performance and government-mandated reporting of adverse events, complications must be categorized in a standard fashion to be valid and relevant.
In 1992, Clavien and associates 23,24 proposed and validated a standardized categorization of complications based on therapy-oriented severity grading of complications after general surgical procedures in an attempt to minimize the subjectivity in reporting and classifying complications. This novel Clavien classification has been slowly adopted over the past 5 years by the urologic community and has been used in the reporting of outcomes of laparoscopic radical prostatectomy, donor nephrectomy, and PCNL. 17,25
By using the universal system for reporting perioperative complications, both Tefekli and colleagues 25 (2008) and de la Rosette and coworkers 17 (2008) facilitate comparisons between institutions and countries. With the overall complications in our series at 11.6%, the Clavien graded complications are lower than the two aforementioned published studies (Table 5). Our Clavien grade IIIa, IIIb, and IVa complications, however, are higher than those reported by de la Rosette and colleagues. 17
It is our belief that this is, at least, partially because of our high rate of upper pole access, which is planned to increase stone clearance through a single access, especially for staghorn stones, and to reduce hemorrhage and the need for transfusions. We had a large incidence of staghorn calculi (88, or 27.8%), and our incidence of second tract insertion was 5%, with no second-look procedures. In our series, there were no perioperative complications specifically related to performing the PCNL in the prone-flexed position. With the inferior displacement of the kidneys in the prone-flexed position, we were able to gain access to the upper pole calix in a infracostal fashion in 21% of cases, and above the 12th rib in more than two-thirds of cases. In no case was the tract angled superiorly in an attempt to avoid a supracostal access. It is our belief that angulation of the nephroscope inferiorly along the axis of the kidney, via a superiorly angled track, results in parenchymal splitting and an increased risk of hemorrhage. In the supracostal access group, 4.8% of supra-11th rib access puncture vs 3.2% in the supra-12th rib puncture patients had pleural complications necessitating intervention.
Regardless of puncture location, all patients had 8.5F to 6.0F nephroureterostomy catheters placed intraoperatively on completion of the case. Our data suggest that, when compared with the previously used 24F Malecot catheter, patients with nephroureterostomy catheters have decreased pain and length of hospitalizations while maintaining ureteral patency and nephrostomy access. 26 In the current era of tubeless PCNL, supracostal access has not been shown to portend an increased risk of postoperative intrathoracic complications. 33,34 Thus, we are presently leaving ureteral stents in uncomplicated PCNLs instead of the nephroureterostomy tubes, rather than leaving the patients totally tubeless. Since changing our practice, we have not noticed an increase in intrathoracic complications.
As a retrospective review, despite the fact that most of the data were captured prospectively, there are some limitations of the current study. A prospective, randomized controlled trial would be ideal to compare the prone with the prone-flexed position using the Clavien system for reporting complications, or to compare supracostal vs infracostal access. Also, because this case series reviews the outcomes of two endourologists (one trained by the other in a standardized method for PCNL), in an academic center with an accredited fellowship program, the external validity and generalizability are uncertain. Another limitation, brought forward by Tefekli and associates, 25 is the application of a system for classifying complications that was originally based on general surgical procedures to an endourologic procedure such as PCNL. Although the need for auxiliary procedures after PCNL (ie, shockwave lithotripsy, ureteroscopy, etc.) would be strictly defined as grade III, because of the need for subsequent therapy, it is not truly a perioperative complication and as such is not included in the current or previously published analyses using this system for PCNL complications. Lastly, it is difficult to capture some of the long-term complications after PCNL (ie, secondary ureteropelvic junction obstruction, infundibular fibrotic stenosis, etc), because these complications take longer to mature and become identified.
Conclusions
The current study demonstrates that incorporating the recently described technique of performing PCNL in the prone-flexed position allows for a safe and effective procedure with minimal complications. The prone-flexed position has several advantages over the flat prone position, with no real disadvantages. Supracostal percutaneous renal access is a safe alternative to infracostal access where appropriate, with a small, but acceptable risk of pleural complications. Furthermore, the application of the Clavien classification of complications facilitates an objective and reliable means with which to compare outcomes between surgeons, hospitals, and various international institutions.
Footnotes
Disclosure Statement
Dr. Honey: consultant, Cook Urological. No competing financial interests exist for the other authors.