
Abstract
Purpose:
We developed step-by-step standardization of left adrenalectomy using laparoendoscopic single-site surgery (LESS) and evaluated the efficacy and safety of this surgical procedure.
Patients and Methods:
To simplify the procedure, we used a technique that involved handling one straight operating instrument and crossing over another articulated assistant instrument intracorporeally. We classified the reciprocal positions of the two instruments into four types. The surgical procedures were divided into six steps, and we applied one of the four types of position to each step.
Results:
Seven patients with left adrenal tumor underwent LESS by two operators. Five received left total adrenalectomy, one left partial adrenalectomy, and one bilateral total adrenalectomy. Mean operative time was 178 minutes. Blood loss was minimal (≤50 mL), and convalescence was uneventful in all patients.
Conclusions:
Although there is inevitably a learning curve, LESS left adrenalectomy can be safely introduced by beginners using a step-by-step standardized technique.
Introduction
The adrenal gland is an ideal target organ for learning the LESS technique in the field of urologic surgery, as it was when conventional laparoscopic surgery was introduced in the early 1990s. We propose a simplified method of instrument handling and standardization of left adrenalectomy using the LESS approach.
Patients and Methods
Handling instruments
We used a flexible 5-mm laparoscope (Endoeye; Olympus, Tokyo, Japan) and two instruments, which were grasped by each of the surgeon's hands. One was the main operating instrument, which included scissors, coagulator with irrigating function (EndoPath, Surgery Probe Plus II; Johnson & Johnson, Tokyo, Japan), vessel sealing system (LigaSure V; Covidien Japan, Tokyo, Japan), and clipping device. All of these devices were straight in shape. The other instrument was used for support of the main instrument. This instrument was an articulated grasper (Roticulator Grasper; Covidien Japan).
During the surgical procedure, these two types of instruments were crossed over each other intracorporeally. We classified the positions of the two instruments into four types (Fig. 1). If the surgeon had the main operating instrument in his/her right hand and the supporting instrument grasped in the left hand crossed above the main instrument, the position of the instruments was “A.” If the supporting instrument grasped by the left hand crossed under the main instrument, the position was “B.” If the main straight instrument was in the left hand and the supporting instrument grasped by the right hand crossed under the main instrument, the position was “C.” If the supporting instrument grasped by the right hand crossed above the main instrument, the position was “D.”

Reciprocal positions of two instruments. Type A: Main straight instrument in the right hand, the supporting articulated instrument in the left hand crossing above the main instrument. Type B: Main straight instrument in the right hand, the supporting articulated instrument in the left hand crossing below the main instrument. Type C: Main straight instrument in the left hand, the supporting articulated instrument in the right hand crossing below the main instrument. Type D: Main straight instrument in the left hand, the supporting articulated instrument in the right hand crossing above the main instrument.
Thus, the upper-right area on the monitor was supported by the second articulated instrument in position A, and areas supported by positions B, C, and D were ordered clockwise. Extracorporeally, we took care to grasp the hand-pieces of the two instruments as they were in the opposite direction from each other, which avoided the instruments colliding and interfering with each other (Fig. 2).
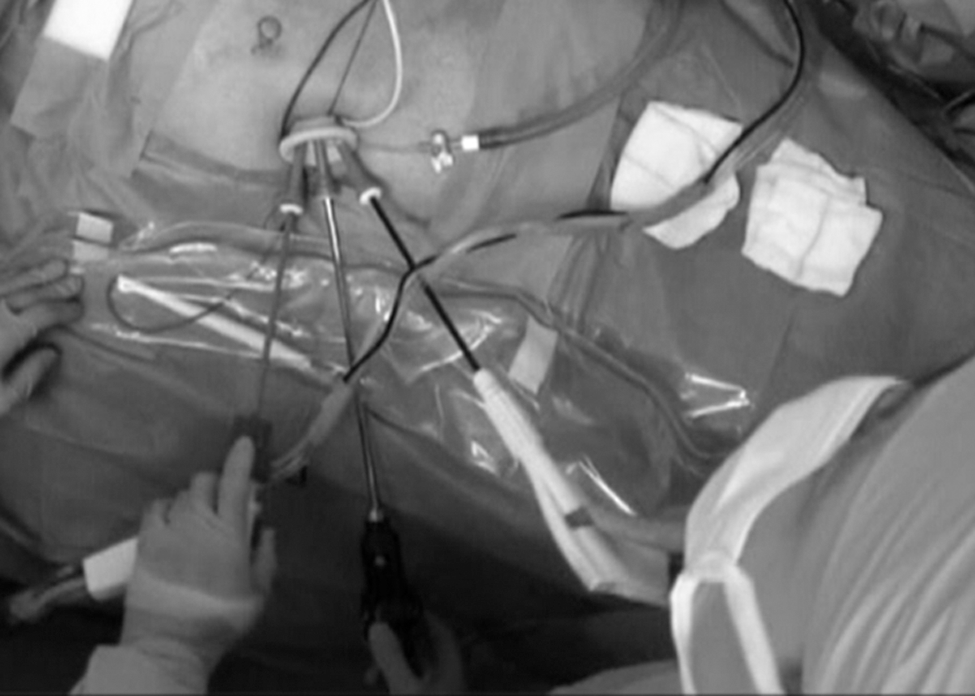
Extracorporeal view. Note that the hand-pieces of the two instruments are directly opposite each other.
Step-by-step surgical procedure
The patient was secured in the right lateral position, and the abdominal wall was sterilized with povidone iodine and draped.
Step 1. Skin incision and pneumoperitoneum
A 2.5-cm single longitudinal skin incision was made. We made this incision in the upper left portion of the abdominal wall or at the umbilicus. We then made a subsequent incision of the fascia and peritoneum, the length of which was identical to the skin incision. Two pieces of gauze were inserted into the peritoneal cavity under direct vision. A SILS™ port (Covidien Japan) was placed, and pneumoperitoneum was achieved. A 5-mm flexible laparoscope was inserted into the peritoneal cavity via the uppermost trocar, and the operative field was visualized in an upside-down manner.
Step 2. Peritoneal incision lateral to the descending colon and dissection between fusion fascia and anterior renal fascia
The peritoneum lateral to the descending colon (white line of Toldt) was incised caudally from the midportion of the left kidney. For this step, the type B position of the instruments was applied. The articulated grasper held a portion of the peritoneum just lateral to the white line and retracted it in a lower right direction on the monitor, when the peritoneum was incised (Fig. 3-I). Dissection of the plane between the fusion fascia and the anterior renal fascia (so-called Gerota fascia) was also performed at this level. Next, the peritoneal incision was lengthened in a cephalad direction around the spleen up to the stomach, with the instruments in the type C position. Dissection of the plane was subsequently performed, with type C position instruments as well. The portion of the peritoneum that was grasped by the articulated instrument, with the right hand of the surgeon, was retracted in a lower left direction on the monitor (Fig. 3-II).
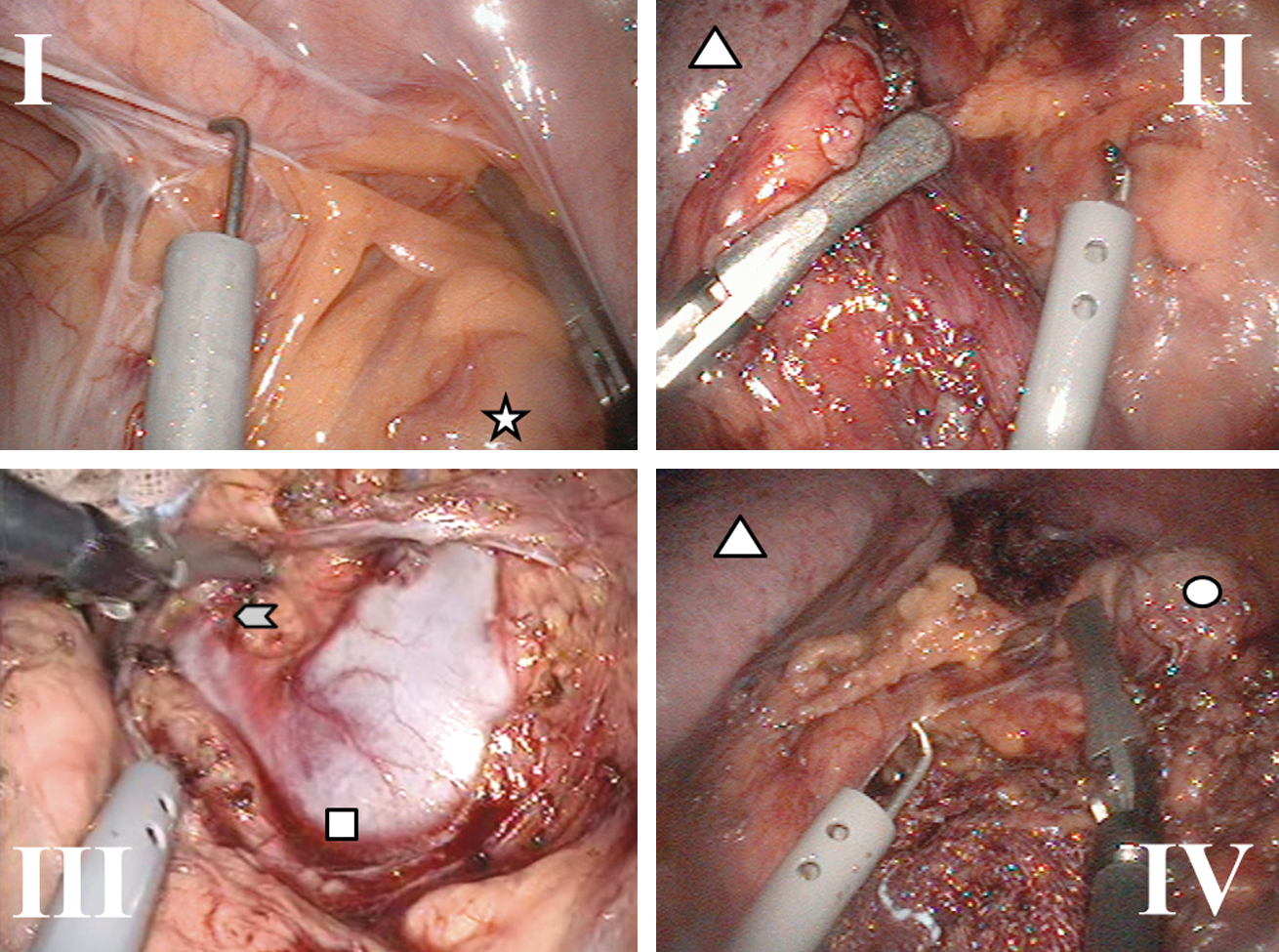
Intraoperative view.
Step 3. Incision of anterior renal fascia, exposure of left renal vein, and transection of left adrenal vein
To open the anterior renal fascia, the instruments were in the type D position to hold the fascia that contained the lymphatics. The fascia was retracted in an upper left direction on the monitor. The left renal vein was fully exposed, and the left adrenal vein was identified. Adequate tension to the adrenal vein was necessary to clip and transect it. The instruments were also in the type D position for this step (Fig. 3-III).
Step 4. Division of the tissue surrounding the adrenal gland
After transection of the left adrenal vein, the avascular space caudal and dorsal to the adrenal gland was opened to expose the fascia of quadratus lumborum muscle. A piece of gauze was packed in this space to elevate the gland. Further elevation of the adrenal gland could be obtained by a support instrument in type A or D position, according to the laterality of the tissue being treated (Fig. 3-IV). Medial and lateral wings that contained small vessels were divided using LigaSure V, and the gland was completely freed.
Step 5. Removal of specimen and insertion of drain
The specimen was enclosed in an endoscopic pouch and removed. After the absence of active bleeding and organ injury was confirmed, a suction drain was placed.
Step 6. Wound closure
After removal of the SILS port, the peritoneum, the rectus fascia, and the skin were closed with 3-0 polyglactin sutures.
Results
We performed LESS left adrenalectomy in seven patients. The characteristics of the patients and the operation profiles are shown in Table 1. For case 3, we performed partial left adrenalectomy. Until exposure of the left adrenal vein, the surgical procedure was identical to total adrenalectomy. Despite transection of the left adrenal vein, the adenoma was excised with a LigaSure V device. The patient with ectopic adrenocorticotrophic hormone syndrome from carcinoid (case 4) underwent simultaneous bilateral adrenalectomy, because the excess secretion of adrenal steroids and its activity could not be controlled by medical treatment. In the following results, the left adrenalectomy part of the whole operation was analyzed.
TA=total adrenalectomy; PA=partial adrenalectomy.
The operative procedures of six patients were completed according to our standardized technique. Sufficient medial mobilization of the spleen and the pancreas could not be obtained by LESS alone in case 4; therefore, an extra trocar was added. Mean operative time was 178 minutes. Although step 2 was the longest procedure in all cases, it occasionally took a relatively long time to perform the procedures of steps 3 and 4 (Table 1). Blood loss was ≤50 mL, and convalescence was uneventful in all cases.
Discussion
Laparoscopic adrenalectomy has been the treatment of choice for various adrenal tumors for a long time, because it is less invasive than open surgery. 4 Although LESS can be even less invasive than conventional laparoscopic surgery, the superiority of LESS adrenalectomy over conventional laparoscopic adrenalectomy should be evaluated, because it is harder for general urologic surgeons to master the LESS technique than the conventional laparoscopic technique.
The main difficulties encountered in LESS arise from collision and interference of the instruments used. To avoid this problem as much as possible, we used only four instrument positions, which were based on the technique in which two instruments crossed over each other intracorporeally (intracorporeal crossing technique).
There are several techniques other than intracorporeal crossing, such as parallel and extracorporeal crossing techniques. Although the parallel technique, in which there is triangulation but not crossing, provides a natural position of two instruments similar to that in conventional laparoscopic surgery, the angle made by the two instruments is narrow. The extracorporeal crossing technique yields a wide angle of the two instruments, with a main straight one in the surgeon's dominant hand. In this technique, however, the surgeon has to cross his hands extracorporeally.
The intracorporeal crossing technique makes a wide angle of two instruments without crossing the surgeon's hands. The drawback of this technique is the necessity to handle the main straight instrument with the non-dominant hand. As a result, extra attention should be given—especially in step 3, in which meticulous handling of the tissue is mandatory. This defect can be easily overcome with experience, however, and other types of manipulation, such as handling of an articulated instrument for meticulous dissection by the dominant hand, would be more difficult to master.
We paid particular attention to the direction of the hand-piece of the instruments as well. In whichever direction the tips of the instruments were facing, placing both hand-pieces in the opposite direction minimized any unnecessary extracorporeal collision and interference of the instruments.
The duration of the operation naturally depends on the individual surgeon. In case 7, it took 291 minutes to perform all procedures. This time could have resulted partly from it being a relatively difficult case and partly because the operation was carried out by an inexperienced operator. Including case 7, however, bleeding was minimal, and convalescence was uneventful in all cases. Although our mean operative time was 178 minutes, including case 7, it was almost equal to that of conventional laparoscopic adrenalectomy, which has been shown to be 156 to 227 minutes, 5 –9 and that of transperitoneal LESS adrenalectomy, which has been shown to be 82 to 200 minutes. 10 –12
Overall, our simplified and standardized technique is effective for surgeons who are beginners with LESS. Although a learning curve is inevitable even after adoption of a standardized surgical procedure, the risks of initial patients should be minimal. With the future development of more sophisticated devices, it is expected that LESS will become more comfortable for surgeons. LESS adrenalectomy, however, can be performed safely using currently available devices.
Conclusions
We developed and introduced a standardized procedure of LESS left adrenalectomy with simplified instrument handling techniques. Our limited experience suggests the safety and feasibility of LESS left adrenalectomy to those who are beginners with the technique, although the superiority of LESS adrenalectomy over conventional laparoscopic adrenalectomy should be evaluated in the future.
Footnotes
Disclosure Statement
No competing financial interests exist.