
Abstract
We describe a new renal displacement technique using an 18-gauge needle to facilitate superior calix puncture and consequently to decrease intrathoracic morbidity. Initially, a lower or middle calix is punctured with an 18-gauge needle. Then, the proximal end of the needle is progressively pushed in the cephalic direction. Therefore, the kidney is pushed caudally by the lever maneuver. This technique has also been used to immobilize the kidney or to reorient complex and malrotated kidneys.
Introduction
Thus, many techniques for minimizing the potential morbidity of the supracostal approach have been reported. For instance, the triangulation technique has been reported by vanSonnenberg and associates 2 using a subcostal angulation of the needle. Karlin and Smith 3 have described a technique for caudal renal displacement, by rotating back an Amplatz dilator and sheath cranially, placed through a central or lower pole calix. Furthermore, an occlusion balloon catheter in the renal pelvis can be used to apply gentle caudal traction and downward kidney displacement. 4
We describe a renal displacement technique using an 18-gauge needle to make the superior calix easily reached between the 11th and 12th ribs or even below the 12th rib.
Technique
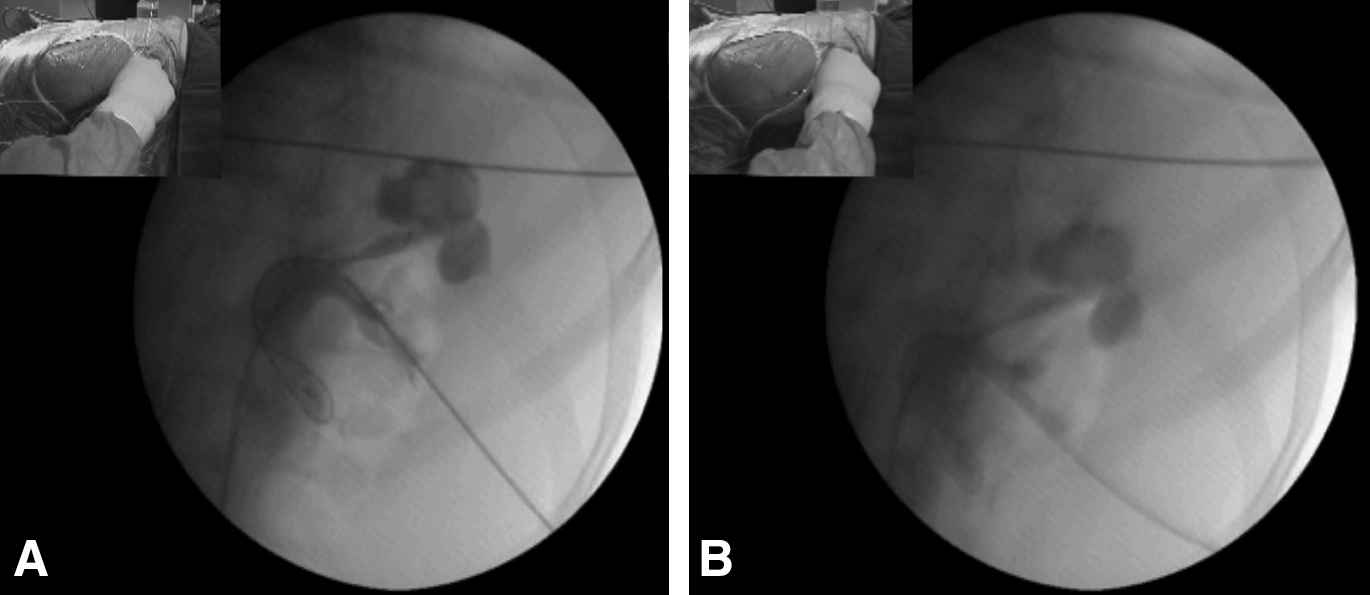
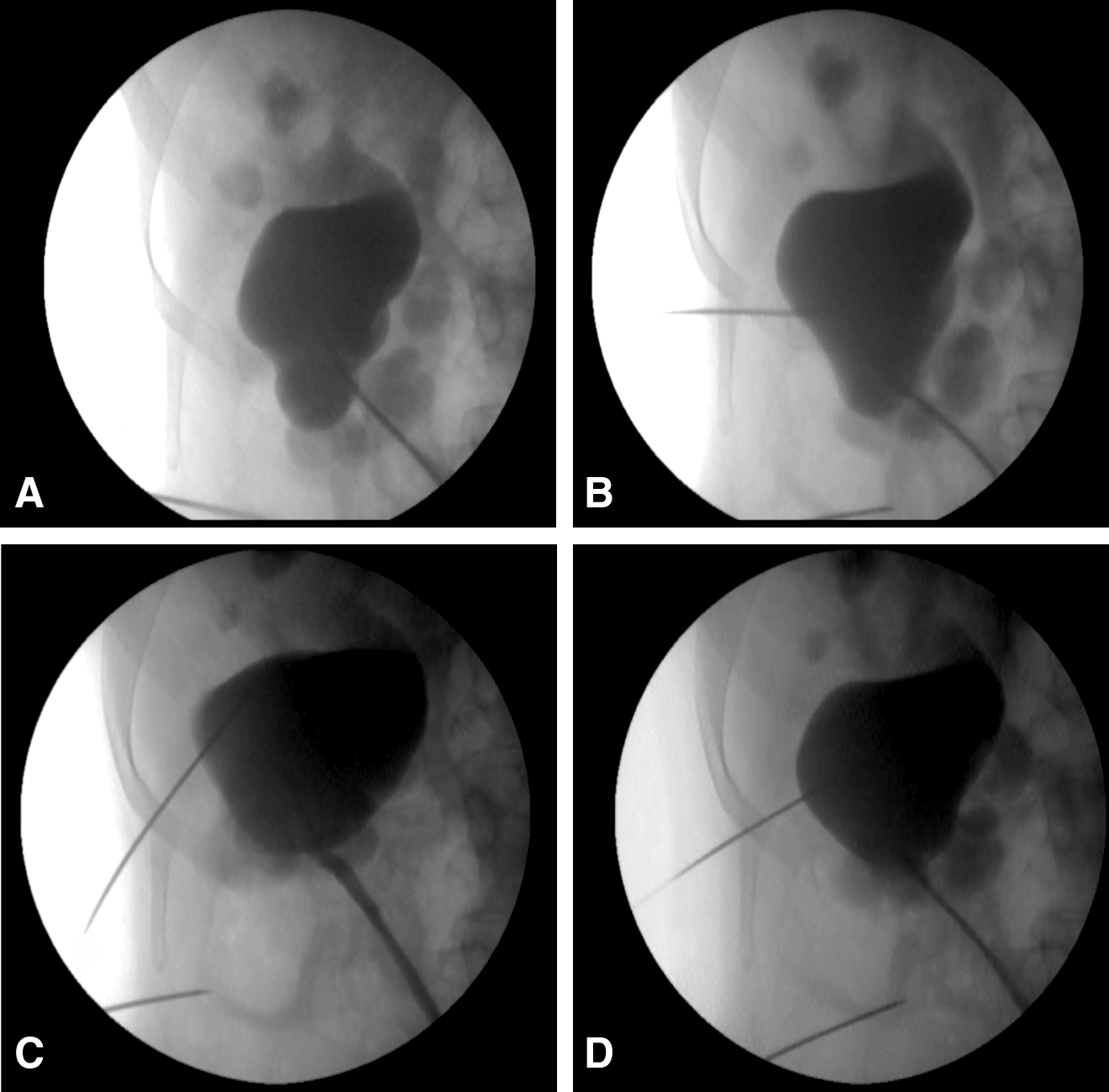
The needle renal displacement technique is performed under fluoroscopic guidance, with the X-ray beam perpendicular to the tract. Initially, a lower or middle calix is punctured with an 18-gauge diamond-tipped needle. Then, a stiff shaft hydrophilic guidewire is inserted (Fig. 1A). The needle's proximal end is progressively pushed in the cephalic direction, under continuous fluoroscopic monitoring. Consequently, the kidney is pushed caudally by the lever maneuver (Fig. 1B). Simultaneously, the body of the needle is gradually bent and fixed to the drape by a forceps (Fig. 2).

The body of the first needle is gradually bent and fixed to the drape. Then the puncture of the superior calix is performed close to the entry of the first needle.
Secondly, the upper pole calix is punctured, and tract formation is performed (Fig. 3). Besides, there is also a slight inversion of the normal axis of the kidney, as the lower pole is tilted medially and the upper pole is oriented laterally. Thus, the upper calixes are reoriented downward and nearer to the cutaneous entry. Therefore, there is a better presentation of the targeted calix (Supplementary video of this technique is accessible online at
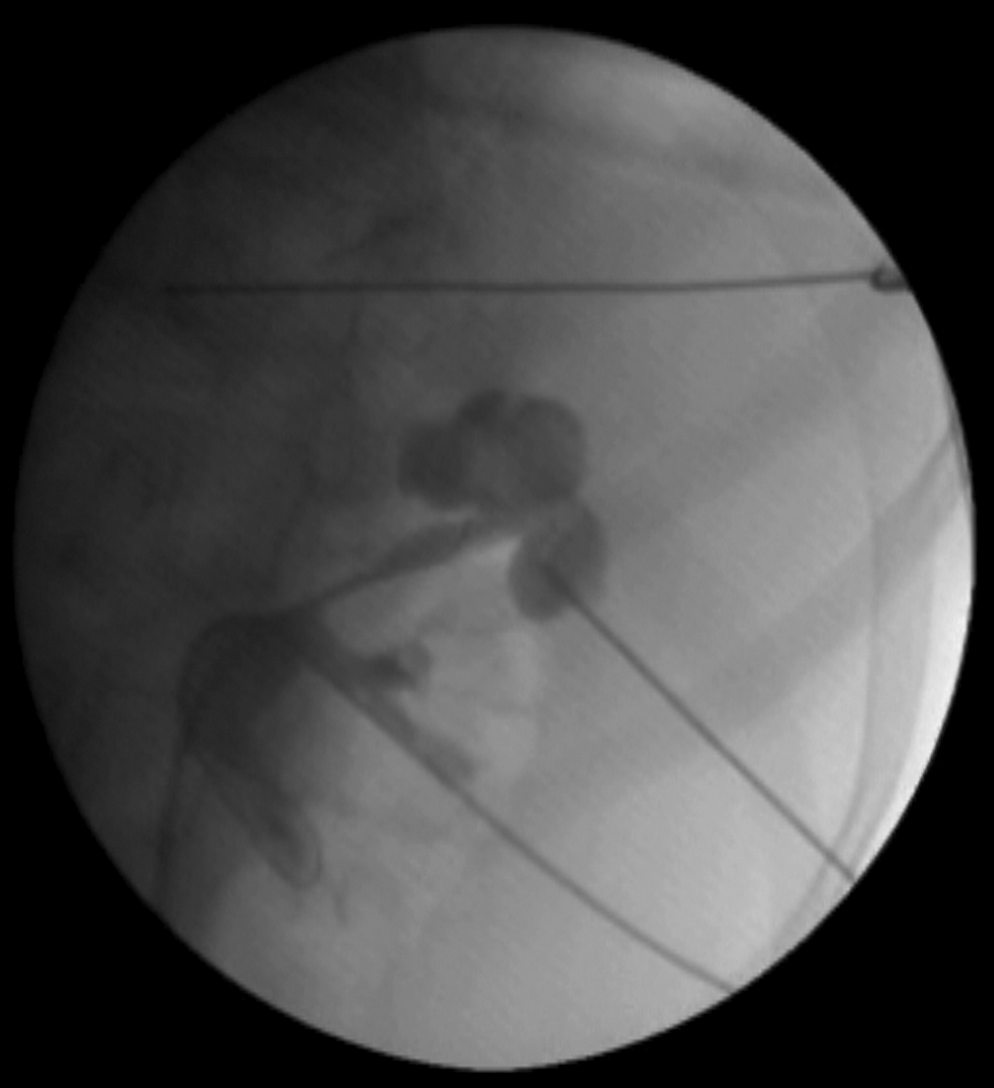
After caudal renal displacement, the kidney is many millimeters lower and the upper pole calix is more accessible.
Discussion
In the beginning of our experience, we had a concern about the risk of urothelium or renal parenchyma shear injury by the needle's distal end. Therefore, endoscopic control of the first point of entry was performed by flexible or directly rigid nephroscope whenever possible. No hemorrhage or urothelium laceration was noted, nor any complication related to the technique. Accordingly, a stiff shaft hydrophilic guidewire is used to push urothelium and calix in the needle-tip pressure point. On the contrary, a Chiba-tip needle must not be used because of its sharp tip (Fig. 4).
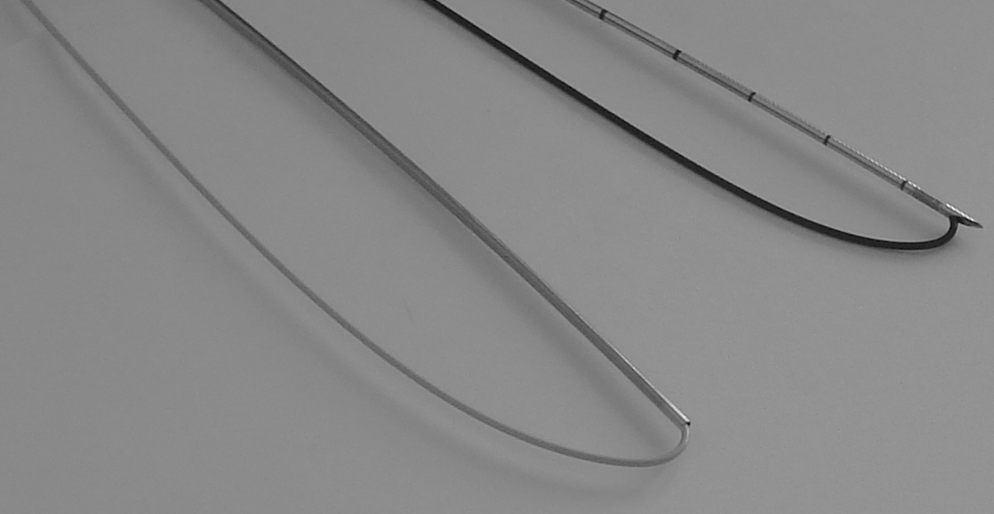
Comparing the tips of two 18-gauge needles: On the left, a diamond-tipped needle with a hydrophilic guidewire (two-part trocar needle and Roadrunner,® Cook Medical) with a smooth transition after bending of the guidewire. On the right, a Chiba-tip needle with its sharp tip protruding after bending of the guidewire (HiWire,® Cook Medical), with risk of urothelium injury if used for the needle displacement technique.
This displacement technique has always been possible in kidneys with no surgical history. It failed, however, when the kidney had been fixed by postsurgical adhesions. Furthermore, the displacement was also effective in patients with previous percutaneous surgery. Thus, a displacement of many millimeters to many centimeters might be gained for a direct upper calix puncture. Otherwise, at least a decrease in angulation of the needle is achieved. Still, for some large hydronephrosis, the renal displacement was unsatisfactory, maybe because the kidney is more elastic. Consequently, another needle renal displacement was performed via a middle calix (Fig. 5). No difference of renal displacement between right and left kidneys was noted. Moreover, this displacement technique has been used with the same effectiveness during percutaneous surgery in the prone position or in the split-leg modified lateral position. 5 In addition, the needle renal displacement technique has been performed, the other way around, to reorient a medial lower calix by displacing the kidney in the cephalic direction via a central calix (Fig. 6).
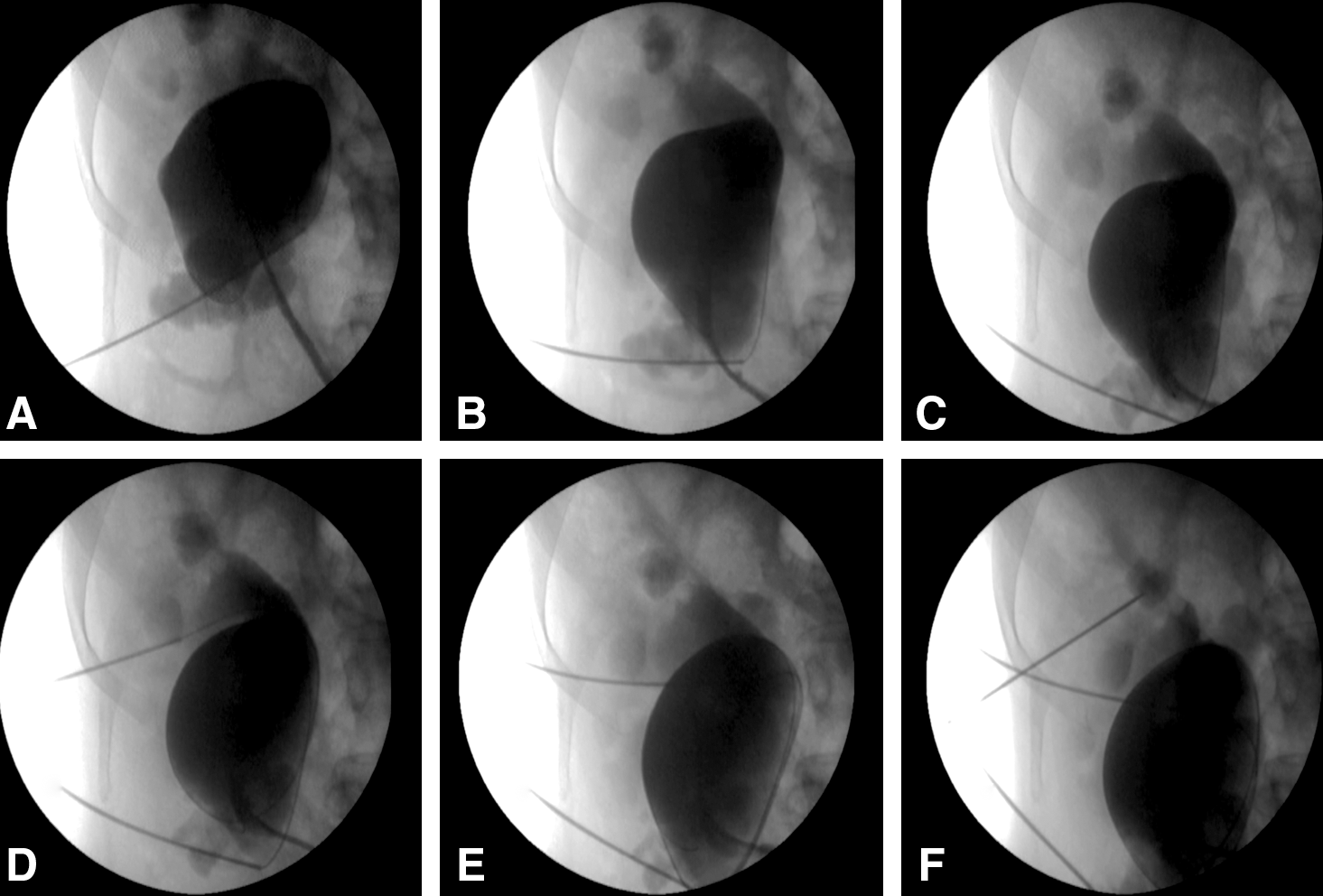
Right large hydronephrosis and malrotated kidney.
A cephalic mediorenal needle displacement is performed to reorient a lower calix and to immobilize the kidney.
Although a comparative study is necessary, the needle renal displacement technique seems less invasive and less time consuming than Amplatz sheath and dilator renal displacement. 3 In fact, these two techniques are complementary. In some patients, renal displacement has been performed, with success, by the nephroscope and Amplatz sheath, after the needle displacement failure. Actually, renal displacement techniques make the superior calix accessible while avoiding intrathoracic complications. Yet, such techniques are effective only when the kidney is mobile.
Footnotes
Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.