
Abstract
Purpose:
To determine whether the overall ureteral flow through an obstructed ureter using the 3F MicroStent™ that uses a novel film occlusion anchoring mechanism is comparable to the flow using a conventional 3F and 4.7F Double-J stent.
Materials and Methods:
An in vitro silicone ureter model and an ex vivo porcine urinary model (kidney and ureter) were used to measure the overall flow through obstructed and unobstructed ureters with either a 3F Double-J stent (Cook), 3F MicroStent (PercSys), or 4.7F Double-J stent (Cook). Mean flow rates were compared with descriptive statistics.
Results:
Mean flow rates through the obstructed silicone ureter (12-mm stone) for the 3F MicroStent, 3F Double-J stent, and 4.7F Double-J stent were 326.7±13.3 mL/min, 283.3±19.2 mL/min, and 356.7±14.1 mL/min, respectively. In the obstructed ex vivo porcine ureter model, the flow as a percentage of free flow was 60%, 53%, and 50 %, respectively. In both ureteral models, flow rates of the 3F MicroStent and 4.7F Double-J stents were not statistically different.
Conclusions:
The 3F MicroStent demonstrated drainage equivalent to a 4.7F Double-J stent, in both in vitro silicone and ex vivo porcine obstructed urinary models. We have demonstrated the crucial first step that this 3F stent, using a novel film occlusion anchoring mechanism, has equivalent, if not slightly improved, drainage rates when compared with its larger counterpart.
Introduction
Stones that obstruct the ureter result in disruption of flow, hydronephrosis, and pain, with prolonged obstruction potentially resulting in renal dysfunction. Intolerable pain and infection associated with acute renal colic are indications for urgent intervention, and ureteral stent placement is one of the first-line actions taken to relieve such obstructions.
Placement of a ureteral stent within an impacted ureter can facilitate restoration of urine flow as well as stone and/or fragment passage by triggering dilation of the ureter from the foreign-body reaction of the urothelium to the presence of the stent. Because the size of stones or stone fragments that can pass is dependent on the space between the ureteral wall and the stent surface, it would be advantageous for a ureteral stent to create maximal dilatation while occupying as little space as possible within the lumen of the ureter.
The commonly used ureteral stents have retention “pigtail” curls on their proximal and distal ends so that when in position, the curls reside in the renal pelvis and the bladder to limit migration. The two curls give these stents their common designation of Double-J stents. A novel stent that consists of a 3F cannula with a distal bladder anchoring coil and a unique proximal film component, designed to facilitate anchoring in the ureter immediately proximal to a ureteral calculus, rather than in the renal pelvis, has been designed. A 4.7F Double-J stent is the smallest size typically used in adult patients, but data are lacking as to why 3F ureteral stents are not used in adults. The film anchor of the MicroStent device is a variant of the film occlusion used on the Accordion Stone Management Device (Percutaneous Systems), but rather than occlude the lumen of the ureter to limit stone fragment migration during lithotripsy, the film anchor of the MicroStent device contains holes in the film to facilitate fluid flow and is an open-ended spiral when the anchor is engaged (Fig. 1).

The 3F MicroStent disengaged (left) and engaged (right), showing the holes in the film occlusion that facilitate urine flow through the ureter.
We compared the flow characteristics of this 3F film stent to that of conventional 3F and 4.7F Double-J stents in obstructed in vitro ureter and ex vivo porcine ureter models to determine whether the use of a small diameter stent with a novel anchoring component is sufficient to decompress an impacted renal system.
Materials and Methods
The flow rates past an obstruction of a 3F MicroStent (Percutaneous Systems), a 3F Double-J stent (Sof-Flex Double Pigtail Stent, Cook Medical), and a 4.7F Double-J Stent (Sof-Flex Double Pigtail Stent, Cook Medical) were tested in an in vivo simulated ureter and an ex vivo porcine urinary model.
Deployment of MicroStent
The undeployed MicroStent was advanced over an integrated 0.035 inch diameter core guidewire and observed under fluoroscopic imaging. Radiopaque markers delineated the position of the anchoring film and stent. Once the film was beyond the stone, the film anchor was deployed by retracting the guidewire. After full removal of the guidewire and anchoring of the stent, the stent positioner was removed, leaving the stent anchored via the film anchor above the stone and the pigtail retention curl within the bladder.
Flow around an obstruction in a simulated ureter
The simulated ureter consisted of a silicone-based cannula, with wall thickness and elasticity characteristics similar to those of porcine ureters. 3 A 12-mm sphere, molded from UltraCal 30 material, was inserted into the simulated ureter to mimic an obstructing ureteral calculus.
The in vitro renal system consisted of a reservoir connected to the simulated ureter. A constant head pressure of 20 cm of water was maintained using a circulating water pump that was set to maintain the water level in the reservoir at a height of 20 cm above the simulated ureter (Fig. 2). This pressure setting was based on the fact that it was previously reported in obstructed renal systems using the Whittaker test. 4 Once the obstruction was in place, the 3F Double-J stent, 4.7F Double-J stent, or 3F MicroStent device was advanced past the simulated obstruction in the artificial ureter. Once the stent was in position, flow in the obstructed ureter was measured over 3 minutes using the performance standard established for assessing Foley catheter flow (ASTM F623-99). As per the standard, three measurements of flow were collected with the stent in an initial position, and then the stent was removed and reinserted at an alternative position (approximately 90 degrees circumferentially from the initial position) and three additional flows were measured for a total of six flow measurements per stent. Even though ASTM F623-99 specifies that clinicians are to collect flow over 3 minutes, urologists typically assess urine flow as mL/min, so the data were divided by three to bring the values in terms of mL/min before analysis.
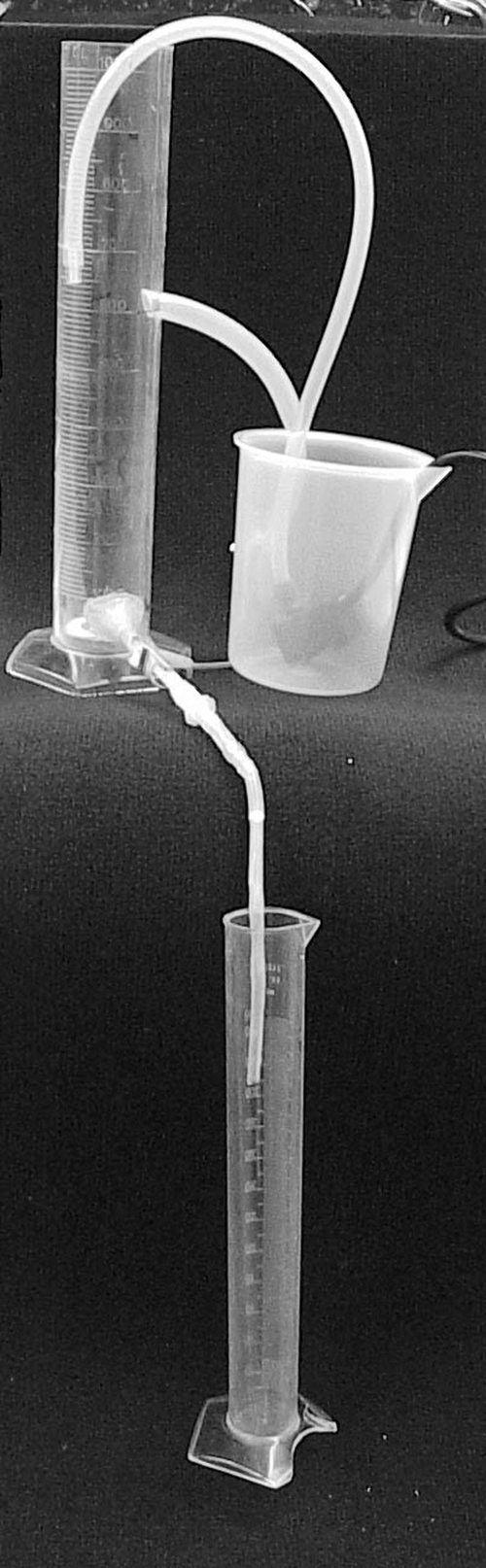
The simulated ureter model. The system consisted of a reservoir connected to the simulated ureter. A constant head pressure was maintained using a circulating water pump that moved water between the graduated cylinder and the reservoir.
Ex vivo porcine ureter experiments
Porcine urinary systems were harvested en bloc from three pigs for ex vivo testing of flow rates and drainage characteristics in unobstructed and obstructed ureters. Continuous flow with a consistent head pressure of 20 cm of water was generated as described above. The flow rates realized by the porcine ureters were measured under four scenarios: an unobstructed ureter with no stent or stone to provide a benchmark of the flow rate possible through the excised ureters; an unobstructed ureter with an indwelling stent only; a ureter obstructed with a 5-mm simulated stone but with no stent; a ureter obstructed with a 5-mm simulated stone and an indwelling stent. Flow was recorded at 1-minute intervals for a total of five separate measurements. To reduce the potential for flow to increase over time because of repeated uses of just one excised ureter, three independent experiments were performed in three different ureters for a total of 15 measurements per stent.
Initially, the flow through an unobstructed ureter was measured in order. Next, the ureter was obstructed using a 5-mm stainless steel ball bearing that was carefully advanced up the ureter, to a position approximately 10 cm proximal to the ureteral orifice. A ball bearing was chosen based on the fact that the smooth surface would cause minimal damage to the ureteral wall. The extent of the obstruction was measured by allowing water to flow through the system and measuring the output. Next, each of the stents was inserted past the obstruction using the respective guidewires, and flow with the stent in position was measured at 1-minute intervals. The extent of obstruction was verified before the next stent was inserted. Flow rates were tabulated for both the simulated and ex vivo model, and descriptive statistics (t test) were used to compare the rates realized with the ureteral stent used. Statistical significance was set at P≤0.05.
Results
Simulated ureter experiments
Flow rates in the obstructed silicone ureteral model were not significantly different between the 3F MicroStent and either the 3F or the 4.7F Double-J stents (Table 1), but the 3F Double-J stent drained significantly slower than its 4.7F Double-J counterpart (P<0.01).
12-mm obstruction averaged over six collections of 3 minutes each.
Ex vivo porcine ureter experiments
The mean flow rate for the excised ureters without any obstruction present was 101 mL/min. After insertion of each of the stents into the unobstructed ureter, no significant changes in the mean flow rates were observed (Table 2). When viewed as a percentage of unobstructed flow, the presence of the cannula of the 3F MicroStent and 4.7F Double-J stent only reduced the flow by 20%.
Placement of a 5-mm stone phantom within the lumen of the ureter resulted in a 95% reduction in flow compared with the mean flow of the unobstructed ureters, verifying that our obstruction model was appropriate. Insertion of the 4.7F Double-J stent past the ostruction provided a flow that was significantly higher than that measured with a 3F Double-J stent (P=0.02). In contrast, no significant differences in flow rates between the 4.7F Double-J stent and the 3F MicroStent were observed (P=0.33) (Table 3). When compared with the flow rate of the 3F Double-J stent, the 3F MicroStent was found to provide significantly higher flow (P=<0.01) (Table 3), possibly because of the configuration of the film anchor.
Discussion
The purpose of this study was to compare the flow characteristics of the novel 3F MicroStent with those of similar conventionally used Double-J stents. For flow comparison, we chose 3F and 4.7F stents rather than the more commonly used 6F Double-J stent because we wished to show equivalence in drainage of the 3F MicroStent to clinically used stents with similar diameter. In addition, we wanted to determine whether the 3F MicroStent would provide sufficient drainage to empty the kidney even though it may not have the same rate of drainage provided by a larger 6F stent.
The 3F MicroStent device had similar, if not improved, flow in both the in vitro and ex vivo flow models when compared with the conventionally used 4.7F Double-J stent, and had higher flow than the 3F Double-J stent. These findings seem rather counterintuitive, given the fact that the cross-sectional area of the cannulae of both the 3F Double-J stent and the 3F MicroStent devices is comparable, making a statistically higher flow rate with the MicroStent device less likely. One possible explanation for this difference may be the increase in “tenting” of the ureteral tissue adjacent to the stone created by the MicroStent's film anchor (Fig. 3a), which is absent for the Double-J stents (Fig. 3b). This capability of the MicroStent to push the urothelium away from the stone surface is an advantageous characteristic, permitting a larger volume of urine to leak past the stone, presumably resulting in adequate decompression of the kidney in an obstructed renal system to facilitate adequate flow in an obstructed renal system.

Even though Double-J stents are manufactured with side holes and a lumen, research has noted that extraluminal flow (along the outside of a stent's cannula) is higher than intraluminal flow, 5 –7 possibly because of the extremely small lumen of these stents. The fact that flow did not differ significantly between the 3F MicroStent and the larger 4.7F Double-J stent likely is attributable to the majority of fluid flow being extraluminal, suggesting that entirely extraluminal drainage may be adequate to relieve intrinsic ureteral obstruction. An additional advantage of complete extraluminal flow is the increased bulk flow of urine that it creates. In the case of stents that contain an open lumen, the fluid that flows intraluminally does not contribute to the force generated by fluid flow across the outside of the stent, presumably decreasing the force acting on a stone fragment that is moving down the ureter. In the case of lumenless stents, all of the flow is around the outside of the device, meaning that the force acting on the fragment is greater, thus increasing movement of stone fragments down the ureter.
In addition, deployment of the film anchor of the MicroStent also may assist in facilitating expedited stone expulsion when compared with Double-J stents. The potential for larger stone fragments to pass alongside the stent may be increased as a result of the extent of tissue tenting and ureteral dilatation caused by the film anchor. Interestingly, even though the presence of a Double-J ureteral stent results in ureteral dilatation, passage of stones or stone fragments is impeded by the stent, and either will take longer than if no stent is present 8 or will occur only after the stent is removed. 9 The film anchor component of the MicroStent alone may provide enough ureteral dilatation to facilitate fragment passage.
Another factor that affects stone passage is ureter peristalsis, the force that propels a bolus of urine down the ureter and therefore also facilitates the movement of stone fragments with the drag caused by bulk urine flow. Indwelling Double-J stents have previously been shown to prevent ureteral peristalsis. 5,6,10 So-called poisoning of peristalsis by Double-J stents not only creates backpressure on the kidney, leading to hydronephrosis, but also contributes to patient discomfort. Devising a ureteral stent that uses an anchoring mechanism that does not affect peristalsis and yet limits migration of the stent may be more beneficial to patient comfort and stone fragment passage than current Double-J stent designs.
Previous research with in vivo porcine models has shown that standard Double-J stents reduced the frequency of ureteral peristalsis significantly. 5,10,11 Given the similarity between human and porcine ureteral anatomy and physiology, the presence of a ureteral stent is believed to impair calculus passage in humans. 5 This is thought to be because of physiologic changes originating in the renal pelvis and ureter secondary to the presence of a ureteral stent and has been shown to cause a delay in the transit time necessary for a stone to pass to the bladder. 8,9,12 It has been shown previously that smaller diameter stents interfere less with peristalsis and that this is likely because of the smaller contact surface with the ureteral wall. 10,13 In addition, the presence of the proximal coil of a Double-J stent in the renal pelvis may also interfere with peristalsis, as the “pacemakers” for peristalsis are believed to be located in this area. 14 –17
Given that the MicroStent device has a smaller diameter and the novel film component designed to anchor proximally to the ureteral calculus, surface contact with the renal pelvis is absent, and contact with the proximal ureter is limited, potentially reducing the impairment of this stent's design on ureteral peristalsis. It is unclear, however, what effect, if any, the film anchor of the MicroStent device to the urothelium may have on peristalsis.
Ureteral stents are designed to prevent obstruction of the ureter after procedures used to break up urinary calculi. Although effective, typically urologists will place a 6F Double-J stent (2-mm diameter) to produce flow around an indwelling ureteral stone, with a 4.7F Double-J stent being the smallest size that will be used in adult patients. When in position, the cannula or shaft of the Double-J stent facilitates passage of urine around the stone or obstruction, which, over time, results in the decompression of the kidney and symptom relief.
Even though they provide a means to decompress the kidney, indwelling ureteral Double-J stents are associated with significant morbidity, with the most bothersome symptoms being bladder pain, storage symptoms, and hematuria. 18 –20 More than 80% of patients report Double-J stent-related pain sufficient to affect daily activities, and the mean quality-of-life scores for these patients are reduced significantly after stent insertion. 21 Stent symptoms are believed to be triggered in part by local inflammation of the local urothelium from stent movement. Chew and associates 22 have shown that local irritation of the urothelium by the stent is accentuated by patient movement, which is in part facilitated by the fact that ureteral Double-J stents are not anchored in place but instead allow some movement because of the flexing of their renal and proximal curls.
Current research into ureteral stent design has been directed toward the development of stents that improve the function and diminish patient symptoms associated with the use of conventional 6F Double-J stents. Our results show that the 3F MicroStent device improved the flow in an obstructed ureter by 60% (Table 3), a value similar to the Double-J stents. Although there are no data regarding symptoms evoked by a 3F MicroStent, its smaller size may reduce stent-associated symptoms while providing a level of kidney decompression that is clinically acceptable. In addition, it is theorized that in using a stent with a smaller diameter, tolerability and patient comfort would be improved.
El Nahas and colleagues 23 have shown that crossing of the lower coil to the other side of the bladder, caliceal position of the upper coil, stent length, and larger stent diameter are all risk factors for ureteral stent symptoms. Use of a shorter 3F stent that would not cross that plane, potentially could improve patient comfort. Dunn and coworkers 24 demonstrated a significant reduction in irritative voiding symptoms using a 7/3F tailed stent compared with a 7F stent. These findings however, were not corroborated by other studies that examined the effects of stent diameter on patient symptoms. 25,26
Considering that our results show that a 3F stent with a film anchor permitted flow rates comparable to those of a 4.7F Double-J stent, it is worth investigating whether adult patients tolerate a 3F stent better than a 6F Double-J stent. 19 Further study into the effects of the MicroStent device on reducing stent symptoms is needed.
One of the advantages of the Accordion stone management device, which uses a similar occlusion mechanism, is its ability to prevent retrograde stone fragment migration, and at least one study has shown its effectiveness in ureteroscopy. 27 Because many patients receive a stent after ureteroscopy, these patients may undergo ureteroscopy with a MicroStent device in place, which would serve a dual purpose of preventing retrograde stone migration and facilitate antegrade passage of stone fragments during and after the procedure. Postoperatively, the stent would be able to provide drainage of the upper tract.
Conclusion
The 3F MicroStent device with a novel film-anchoring component provided equivalent drainage to that of a 4.7F Double-J stent. These results were seen in both a simulated ureteral model as well as in excised ex vivo porcine renal systems. We have demonstrated the crucial first step that this 3F novel stent provides adequate drainage that is equivalent to a 4.7F Double-J stent. Future studies should be undertaken to determine its effect on peristalsis, capacity to decompress a hydronephrotic kidney, patient tolerability, and specific flow characteristics that may affect stone passage rates.
Footnotes
Disclosure Statement
No competing financial interests exist.