
Abstract
Purpose:
To present our experience with the first 10 consecutive cases of laparoendoscopic single-site nephroureterectomy (LESSNU) with bladder cuff excision for upper tract urothelial carcinoma.
Patients and Methods:
Ten patients (6 men and 4 women; 6 renal pelvis and 4 ureter) underwent LESSNU by a single surgeon. We made a 4-cm single incision at the umbilicus using a homemade single-port device. The single-port device was made with a surgical glove and Alexis wound retractor. LESSNU was performed by the same technique of conventional laparoscopic NU.
Results:
The mean age was 62.79±7.93 years. The mean total operative time, time for nephrectomy, and time for bladder cuff excision were 225.63±65.87, 80.00±29.03, and 145.63±42.63 minutes. The mean estimated blood loss was 187.50±83.45 mL. On surgical pathologic examination, four patients were pT1N0, four patients were pT2N0, one patient was pT3N0, and one patient was pT3N2. There was one positive surgical margin in a pT3N2 patient. The mean number of lymph nodes dissected was 2.5 (range 0–9). One incision extension was performed because of complete renal hilar lymphadenectomy by open technique (for the pT3N2 patient), and one open conversion with a Gibson incision was performed because of severe adhesions around the distal ureter (the pT3N0 patient). There were one case of transient ileus and one of fever that were improved with conservative treatment. The mean hospital stay was 4.75±3.37 days. Eight patients who underwent LESSNU successfully were satisfied with their operations.
Conclusions:
LESSNU for upper urinary tract urothelial carcinoma seems to be feasible and safe, but it is still challenging for advanced cases.
Introduction
Recently, laparoendoscopic single-site (LESS) surgery that inserts all equipment through a one-port device by a single incision site has been attempted. There were some reports for LESS surgery, and these studies reported that it reduces the pain of the patient, shortens hospital stay, and elevates levels of patient satisfaction from the aspect of esthetic factors. 3 –5
Although there have been many reports on the feasibility of radical nephrectomy by LESS surgery in renal-cell carcinema, 6 few studies have been performed on the feasibility and safety of LESSNU with bladder cuff excision because of the technical difficulties in bladder cuff excision and repair. Therefore, this study was conducted to evaluate the feasibility and safety of an initial 10 cases of LESSNU using a homemade single-port device and to introduce our operative technique based on the oncologic principle.
Patients and Methods
Patients
A single well-trained conventional laparoscopic surgeon performed LESSNU on 10 of the patients who received a diagnosis of upper urinary tract urothelial carcinoma by abdominal CT and/or diagnostic ureteroscopic examination between April 2009 and August 2010. Informed consent was obtained from all patients after a complete description of various surgical methods, including NU, LNU, or LESSNU, and surgery using our homemade single-port device. The mean age of the patients was 62.70±7.93 years (range 54–75 y) and the male to female ratio was 6:4. Six tumors were detected in the left renal pelvis, and four tumors were detected on the right upper ureter (Table 1).
BMI=body mass index; EBL=estimated blood loss.
Operative technique
All the surgeries were performed via a transperitoneal approach. After induction of general endotracheal anesthesia, patients were positioned in the lateral flank position. A single 4-cm vertical incision was made on the umbilicus (Fig. 1A), and the peritoneum was resected using an open technique. A homemade single-port device was constructed using the Alexis® wound retractor (Applied Medical, Rancho Santa Margarita, CA) and a powder-free surgical glove (Fig. 1B). The wound retractor was inserted to the umbilicus incision site, the ring in the vicinity of the wound retractor was covered with a size 6 1/2 surgical glove, and subsequently, the surgical glove was folded and inserted to minimize the gap between the abdominal wall and the glove. Four fingers of the glove were cut; four trocars (2 12-mm trocars and 2 5-mm trocars) were inserted and immobilized with the rubber band. Intraperitoneal CO2 pressure was maintained as 15 mm Hg.
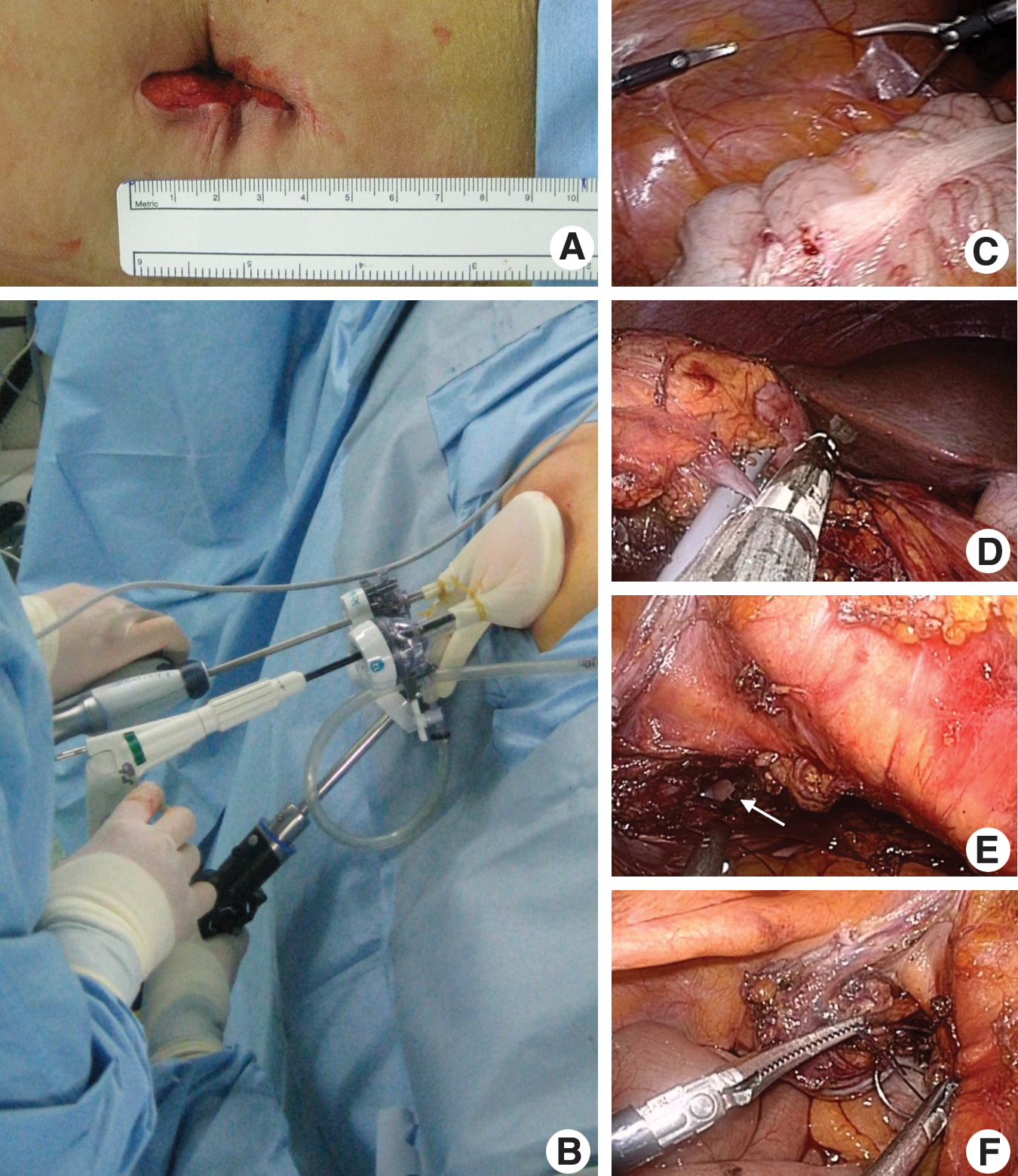
A 10-mm flexible laparoscope (EndoEye,® Olympus Surgical, Orangebur, NY) was inserted to the peritoneum through the 12-mm trocar of the homemade single-port device, and the overall peritoneum, including the surgery area, was examined. Through the remaining trocars, the flexible laparoscopic instruments—the Laparo-Angle™ (Cambridge Endo, Framingham, MA) and the Roticulator™ (Autosuture, Norwalk, CT)—were inserted and crossed to the peritoneal cavity through the single-incision port, and surgery was performed bending the tip area of the articular laparoscopic equipment (Fig. 1C).
The large bowel was dissected along the line of Toldt, and the kidney was exposed. While dissecting the area between the Gerota fascia and the lower pole of the kidney, the renal artery was identified by approaching the renal hilum, after which it was clamped with four to five Hem-o-lok clips (Teleflex Medical, Triangle Park, NC) and resected. The renal vein was then ligated by using an endovascular stapler (Echelon,® Ethicon Endo-Surgery, Cincinnati, OH
The bladder cuff was dissected circumferentially around the ureteral orifice and resected using laparoscopic endoshears by the extravesical maneuver (Fig. 1E). The ureteral orifice defect was exposed by pulling the stay stitches and thereafter closed using a conventional rigid needle driver and dissector in two layers with 2-0 polyglactin continuous suture (Fig. 1F). The integrity of the bladder closure was tested by filling the bladder with 150 mL of physiologic saline.
The specimen was moved to the lateral side of peritoneum, and the Lap-bag® (Sejong Medical, Seoul, Korea) was inserted to the peritoneum. The specimen was inserted into the bag and the bag was extracted. Afterward, the pressure within the peritoneum was decreased to lower than 5 mm Hg, and hemorrhage was assessed. A drainage tube was inserted, and the port device was removed. After the completion of surgery, the skin of the single incision site was sutured and wrapped with Dermabond® (Ethicon, Somerville, NJ).
Statistical analysis
The success rate of the 10 cases was evaluated. Cases that were converted to open abdominal surgery or conventional LNU, operative time, surgical complications, the dose of analgesics after surgery, hospital stay, the postsurgical recovery period, and the time needed to return to normal activity were analyzed. Safety was evaluated by assessing complications before and after surgery.
All patients were analyzed by the preoperative and postoperative visual analogue pain scale (VAPS) score. Pain patterns were examined by dividing the pain level from 0 to 10 points. Without pain was 0 points and the most severe pain selected was 10 points. Discharged patients were instructed to prepare the VAPS 1, 2, and 3 days after surgery at home and bring the results at the time of the visit to outpatient clinics.
Levels of patient satisfaction were evaluated by the classification method of four levels (very satisfied, somewhat satisfied, somewhat dissatisfied, and very dissatisfied). With regard to the classification of the satisfaction level in our study, “satisfaction” was considered as very satisfied or somewhat satisfied.
For the comparison of the VAPS scores before and after surgery, the Wilcoxon signed-rank test and Mann–Whitney U test were applied. Data analysis and statistical analysis were performed using the Open
Results
Of the 10 patients, 1 needed conversion to open surgery through a Gibson incision, 1 needed an additional incision, and the remaining 8 successfully underwent LESSNU using a homemade single-port device without additional incision or transcutaneous port. In these 10 cases, the mean total operative time for LESSNU was 255±87.24 minutes, and in the successful 8 cases, 225.63±29.03 minutes. Time for bladder cuff excision was 145±42.63 minutes in the successful eight cases. The mean estimated blood loss (EBL) of all cases was 260±206.56 mL. In successful cases, the mean operative time for the first four LESSNU surgeries was 248.74±91.69 minutes and that for the last four LESS NU surgeries was 202.50±17.08 minutes. This difference was statistically significant (P=0.014), which means that operative time decreased as the number of surgical cases increased.
In the 10 patients, the mean duration of hospital stay was 4.75±3.37 days. The Foley catheter was removed on postoperative day 7 after checking via cystography. The pathologic stage was pT1N0 in four patients, pT2N0 in four patients, pT3N0 in one patient, and pT3N2 in one patient. The mean number of lymph nodes dissected was 2.5 (range 0–9) (Table 1). All surgical margins, especially on the ureteral orifice, were negative, except for one positive in the patient with pT3N2 on the resected bladder cuff with carcinoma in situ. The patient with pN3N2 underwent one incision with extension for renal hilar lymphadenectomy by the open technique, and the patient with pT3N0 needed conversion to open surgery through a Gibson incision because of severe adhesion around the distal ureter.
There were two postoperative complications (one case of postoperative fever and one case of transient ileus), but there were no major complications. In the 10 patients, the mean VAPS score was 5.90±0.99 on postoperative day 1, 4.80±0.92 on postoperative day 2, and 3.20±0.79 on postoperative day 3 with a significant decrease over time (day 1 vs day 2, P=0.003; day 1 vs day 3, P<0.001). As for patient satisfaction, six patients reported “very satisfied” and two patients reported “somewhat satisfied,” all of whom underwent LESSNU. The mean wound size measured 1 month after surgery was 4.17±0.36 cm.
Discussion
LESS surgery is a challenging one of the minimally invasive surgeries, and it has been used increasingly in the treatment of patients with various urologic diseases. Until now, the goal of LESS surgery is to reproduce open surgeries with minimal invasiveness. In diseases of urologic malignancy, keeping the oncologic principle is also important during LESS surgery. NU for upper urinary tract urothelial carcinoma comprises two operations—ie, nephrectomy and distal ureterectomy. It also has a broad field of surgery from the kidney to the bladder.
LESSNU seems to be the most complex and challenging surgery in urologic LESS surgery. There are few reports for LESSNU. Desai and associates 7 reported their initial 100 patients undergoing LESS, surgery 2 of whom underwent LESSNU. The operative times were 90 and 200 minutes in the two patients, respectively, and there were no postoperative complications. An additional transcutaneous 5-mm port was established in one patient, and cystoscopic resection along with the use of a laparoscopic endostapler was performed for bladder cuff excision and repair. White and coworkers 8 reported their first 100 cases of LESS surgery, which included 7 cases of LESSNU surgeries for upper tract urothelial carcinoma, 6 of which were conventional LESS (C-LESS) surgery and 1 was robot-assisted LESS (R-LESS) surgery. They stated that the mean operative time was 198 minutes and that 1 case necessitated conventional laparoscopic conversion.
Park and associates 9 reported their first two patients undergoing LESSNU surgery, 1 of whom was our first patient. They identified the ipsilateral ureteral orifice after the intramural distal ureter was fully mobilized, and then a 1-cm bladder cuff was excised using flexible laparoscopic endoshears. The cuff excision site was repaired in one layer using 2-0 polyglactin interrupted sutures prepared with a Hem-o-lok and LaparoTy clips (Ethicon Endosurgery, Cincinnati, OH) at the terminal end; then urine leakage was identified using the 200 mL saline test. This bladder cuff excision and repair technique was the same as ours—transvesical maneuver without additional incision.
Ryu and colleagues 10 reported 14 cases of LESS, 2 of which were performed in 2 cases of renal pelvis tumors. They performed LESSNU surgeries through a Gibson incision and bladder cuff excision by the open technique through the same incision. Ponsky and coworkers 11 reported two cases of LESSNU surgeries through a 7.5-cm Pfannenstiel incision using a GelPort (Applied Medical Research, Rancho Santa Margarita, CA). They stated that the operative times of the two cases were 147 and 407 minutes, respectively, and that the bladder cuff was dissected and then the distal ureter was cut.
Jeon and colleagues 12 reported 50 patients undergoing C-LESS and R-LESS surgeries using homemade single-port devices, 4 of whom underwent one C-LESS surgery and 3 underwent R-LESS surgeries without detailed description of the bladder cuff procedure. Seo and associates 13 reported four cases of LESSNU surgeries with an additional lower abdominal midline incision and a bladder cuff procedure by the extravesical open technique. Lee and Lee 14 reported 70 patients undergoing LESS surgeries, 1 of whom underwent LESSNU surgery. They dissected a maximum amount of tissue including the bladder cuff, ligated with a Hem-o-lok and a LaproTy clip, and then cut the distal ureter. They stated that the operative time was 285 minutes and that there were no postoperative complications.
In this study, one (10%) patient needed conversion to open surgery, and the 8 successful cases of LESSNU had a mean operative time of 225.63±65.87 minutes, which showed the feasibility of this surgery (Table 2). All of the 8 patients reported “satisfactory,” and pain gradually decreased day by day. Bladder cuff excision, however, based on the oncologic principle must be considered in LESSNU unlike in LESS surgery for benign diseases.
They performed six conventional and one robot-assisted laparoencoscopic single-site nephroureterectomy.
One of two cases reported by Park et al is the first patient in our study.
They performed laparoendoscopic single-site nephroureterectomy through a retroperitoneal approach.
EBL=estimated blood loss.
Bladder cuff excision is the most important procedure during NU for malignancy. According to previous studies of LESSNU, the ideal methods are: (1) A method that hoes not need additional incision or transcutaneous ports for maintenance of scar-free conditions through the umbilicus, and (2) en bloc bladder cuff excision by an open technique using extravesical maneuver based on the oncologic principle.
Various techniques of distal ureterectomy have been used including open excision, transurethral resection of the ureteral orifice (pluck technique), transvesical laparoscopic detachment and ligation technique (Cleveland Clinic approach), 15 laparoscopic stapling, ureteral intussusceptions. 16 Among these methods for conventional laparoscopic NU, the most ideal method is the open technique that repairs the vesical mucosa with a resection margin of 1 cm around the ureteral orifice. 17 Our LESSNU technique keeps the two aforementioned methods based on the oncologic principle.
Several limitations apply to our study. First, this study is an initial report for LESSNU with a small number of cases. Second, this study has a lack of long-term follow-up data for oncologic outcomes.
Conclusions
Our LESSNU technique resembles an open surgical technique, suggesting that it is safe and adheres to oncologic principles. Our LESSNU may be an alternative minimally invasive treatment option for patients with upper urinary tract urothelial carcinoma, but it is still challenging for advanced cases.
Footnotes
Acknowledgment
This work was supported by the research fund of Hanyang University (HY-200800000008096).
Disclosure Statement
No competing financial interests exist.