
Abstract
Purpose:
The goal of this report is to describe our initial clinical experience performing a simple nephrectomy with the SPIDER (Single Port Instrument Delivery Extended Reach) laparoendoscopic single-site (LESS) surgical system.
Patient and Methods:
One patient with a nonfunctioning kidney secondary to a ureteropelvic junction obstruction underwent a simple nephrectomy through a single incision performed using the SPIDER surgical system. We assessed the technical feasibility, efficiency, and perioperative outcomes.
Results:
The SPIDER-LESS nephrectomy was performed successfully without additional skin incisions for laparoscopic ports, instrument clashing, or open conversion. Total operative time was 210 minutes with blood loss of 50 mL. The patient experienced no intraoperative or postoperative complications. Pathologic evaluation confirmed atrophic renal parenchyma.
Conclusions:
The SPIDER surgical system LESS nephrectomy is feasible and safe. Future refinements of the technology and prospective studies are needed to further optimize its application in urology.
Introduction
Several companies are striving to facilitate single-port laparoscopy by allowing triangulation by means of articulating and/or flexible instruments and creating access that provides more than three ports through the single incision for easier retraction and to free up both hands of the surgeon for dissection. It will likely take multiple innovations and several generations of product improvements to make the single-site approach easier to learn and propagate within the surgical community.
The North-Carolina–based TransEnterix medical device company has introduced the SPIDER® (Single Port Instrument Delivery Extended Reach) surgical system to facilitate single-port surgery. The product received Food and Drug Administration approval in 2009. Since then, it has been applied mostly in the general surgery community for cholecystectomy and bariatric procedures. 1,2 Applying our experience from a porcine nephrectomy model, 3 we proceeded to use this technology on a human case. We report our preliminary experience with the SPIDER surgical system in performing a simple nephrectomy.
Patient and Methods
Patient
The patient is a 26-year-old woman with a left ureteropelvic junction obstruction that resulted in an atrophic kidney, with less than 8% function seen on renal scintigraphy (Fig. 1). The patient was aware of her condition but had been asymptomatic for at least 4 years until her recent pregnancy, during which she began having severe left flank pain. Her pain did not subside after delivery and necessitated the chronic use of opioid analgesics. After consulting with our surgical team, the patient decided to proceed with a simple laparoscopic nephrectomy. She was counseled and signed an informed consent regarding the use of a LESS approach as well as the use of the SPIDER system.

Preoperative CT scan reveals a left hydronephrotic and atrophic kidney.
SPIDER device
The SPIDER surgical system has previously been described in detail. 1 In brief, the device is comprised of a multichannel port connected to flexible instrument delivery tubes. The main cannula has four instrument channels. The superior and inferior channels are 5 mm in diameter and allow for the passage of a bariatric-length endoscope and rigid laparoscopic instruments. The two lateral channels contain the instrument delivery tubes, which are the conduits for the passage of specialized flexible instruments designed specifically for the SPIDER device. The lateral channels provide for true left- and right-handed control over instruments. Using the SPIDER system, the surgeon need never operate cross-handed. The surgeon may adjust the angle of the instrument delivery tubes with a lever on the main external cannula. Relative to the center of the device, the delivery tubes can be fully manipulated between 0 and 45 degrees.
Surgical technique
After general anesthesia induction and Foley catheter placement, the patient was placed in a full flank position with a beanbag supporting the torso and Krause support for her left arm. The surgery was performed by an experienced attending laparoscopist. The GelPOINT system's Alexis wound retractor was then positioned through a 4-cm midline minilaparotomy at the umbilicus and covered with a GelSeal cap (Applied Medical, Rancho Santa Margarita, CA). Because the outer diameter of the SPIDER system is only 18 mm, the incision could have been as small as 2 cm. We preferred, however, to have the GelPOINT system as a safety measure in case we wished to add an additional port without making an extra incision.
We placed the sheathed SPIDER multichannel cannula through the GelSeal cap and positioned it into the body. Pneumoperitoneum was maintained through the GelPOINT device, although the SPIDER has three insufflation/smoke evacuation ports available. For vision, we used a rigid 30-degree, 5-mm Karl Storz bariatric endoscope with a right-angled fiberoptic light adaptor through one of the two rigid central ports of the SPIDER. The SPIDER device was attached to the reusable support mount that was attached to the operating table (Fig. 2).
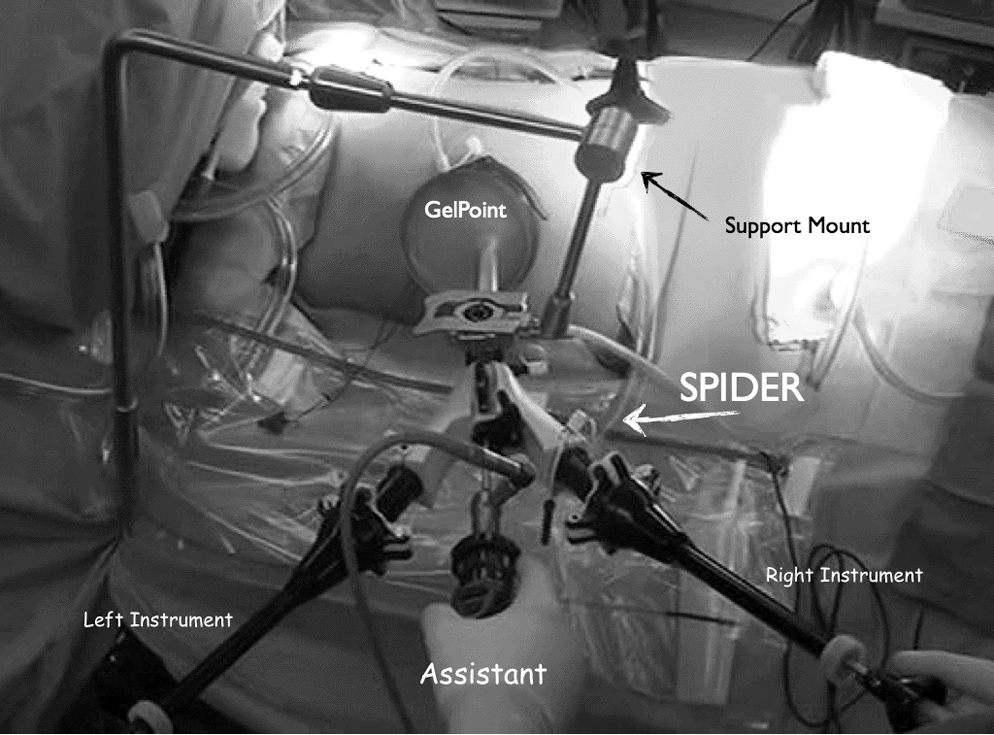
Operative setup: SPIDER is placed through the GelPoint and attached to a support mount.
A left simple nephrectomy proceeded in the standard fashion by first reflecting the descending colon medially, identifying the ureter and gonadal vein, dissecting superiorly toward the renal hilum, and identifying the renal artery and vein. These steps were all performed solely using the flexible SPIDER instruments: Atraumatic graspers, straight blunt-tipped scissors, hook electrocautery, Maryland dissector, and flexible suction (Fig. 3).
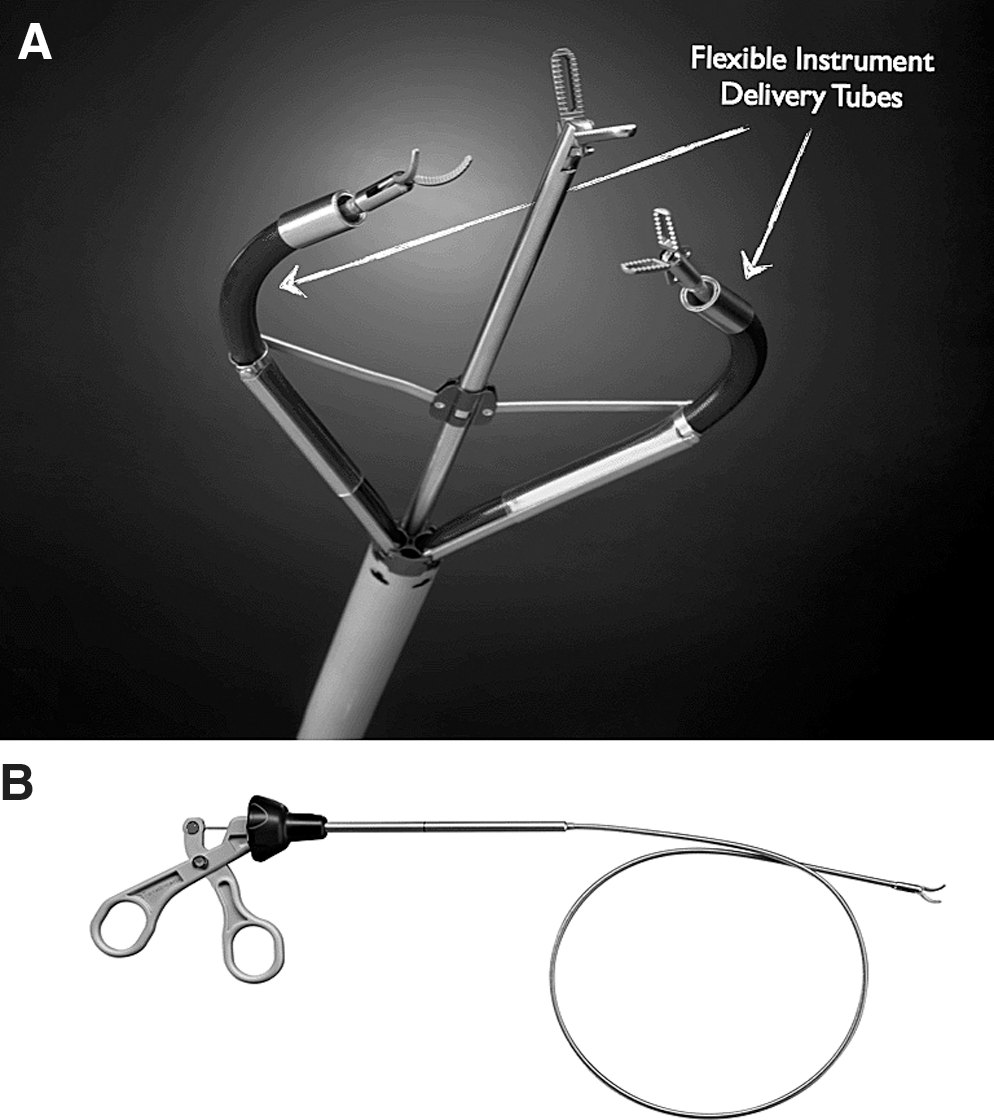
SPIDER flexible instrument delivery tubes
Two renal arteries and one renal vein were identified. We used the SPIDER flexible 5-mm Hem-o-lok clip (Teleflex Medical, Research Triangle Park, NC) appliers to ligate one of the arteries. One extra 12-mm port was placed through the GelPOINT for an assistant laparoscopic grasper and 10-mm Hem-o-lok clip application on one of the two renal arteries and a 15-mm Hem-o-lok clip on the renal vein. Harmonic shears (Ethicon Endo-Surgery, Cincinnati, OH) were used only for the final step of dissection between the kidney and the adrenal gland through the assistant port. We made no additional skin incisions. The specimen was removed intact through the original incision.
Results
There were no intraoperative complications, and estimated blood loss was 50 mL. Total operative time was 210 minutes. The patient was admitted overnight for observation and discharged to home in good condition within 24 hours. Although a visual analog score was not obtained, the patient did not need any additional analgesic other than our standard postlaparoscopic nephrectomy regimen with three doses of 15 mg ketorolac and one dose of 5/325 mg oxycodone/acetaminophen before discharge. Pathologic evaluation revealed atrophic renal parenchyma with changes consistent with chronic pyelonephritis. There were no postoperative complications at 30-days follow up.
Discussion
With the challenges of LESS surgery come innovation. After seeing the potential of the SPIDER surgical system in our porcine model, 3 we were excited to introduce this instrument to our patients. We found that one of the main advantages of the SPIDER surgical system is the ability to easily triangulate instruments because of its core design with flexible instrument delivery tubes (Fig. 3). We were able to maintain pneumoperitoneum and a small single incision, during the entire operation, without compromising our surgical steps or safety of the patient.
The flexible instruments were agile enough to perform a quality dissection with full skeletonization of the entire renal hilum. We found fine and delicate maneuvers with all the SPIDER flexible instruments to be feasible and safe. The instruments inside flexible ports are controlled in a very intuitive manner that is in line with the standard laparoscopic equipment. There was no instrument clashing or instrument malfunction. There are no additional finger or wrist maneuvers that must be learned by the surgeon to control the flexible instruments. These features make the SPIDER system easy to train on and quickly adopt.
The surgery, however, was not without challenges. The flexibility of the instruments, at times, did not provide enough torque when performing blunt dissection maneuvers or lifting the kidney. This, in part, was the reason for performing the superior pole dissection adjacent to the adrenal gland with the Harmonic shears. We thought this would be the safest approach to minimize hemorrhage and operative time. In addition, the SPIDER flexible or rigid 5-mm ports are not large enough to allow for ≥10-mm Hem-o-lok clip application or a laparoscopic vascular stapler; therefore, we were forced to use an accessory port through the GelPOINT to apply larger vascular clips.
The SPIDER does not need an assistant to hold the camera, because it allows for the lens to lock in place, which is useful with a 0-degree lens. When using a 30-degree lens as in this case, however, we found an assistant beneficial to provide different angles and wider scope of the operative field. In terms of ergonomics, this surgical system improves the ergonomics for the primary surgeon but does not solve the inconvenient position the assistant maintains throughout any LESS case holding the camera between the surgeon's arms.
With future planned cases, we hope to provide more clinical outcomes data, such as pain control and patient satisfaction surveys, to further assess any clinical benefit with this new technology.
Conclusion
LESS nephrectomy with current rigid laparoscopic instruments is limited by in-line visualization, restricting the ability to approach the target organs with proper angles and instrumentation. The SPIDER single-port access system with articulating arms and flexible instrumentation minimizes these constraints. We found the SPIDER to be a “surgeon-friendly” LESS platform and safe in performing a nephrectomy. The system offers improved ergonomics compared with traditional laparoscopic instruments, and no instrument clashing. This preliminary experience is encouraging. Further generation technology refinements are expected to optimize urologic applications of this LESS equipment.
Footnotes
Acknowledgments
We wish to acknowledge Brian McCarthy and Mohan Nathan of TransEnterix, Gonzalo Paez of Applied Medical, and Maya Bar-Dov.
Disclosure Statement
Raymond J. Leveillee: Angiodynamics, Inc., scientific study; Covidien, Inc., scientific study/consultant; Cook Medical, lecturer; Intuitive Surgical, proctor; Applied Medical, lecturer. No competing financial interests exist for the other authors.