
Abstract
Purpose:
To introduce transurethal partial cystectomy with a 2013 nm thulium laser as a treatment for paraganglioma of the urinary bladder in adults.
Patients and Methods:
Three patients with pheochromocytomas were treated transurethrally with a 2013 nm thulium laser under general anesthesia. A 2013 nm thulium laser was used to incise the full-thickness bladder wall around the tumors. The entire bladder wall was peeled between the detrusor muscle layer and outer connective tissues. Tumors with full-thickness detrusor muscle layers at the base were removed together. Intraoperative fluctuation of blood pressure, preoperative values of 24-hour urine catecholamine (CA) and vanillylmandelic acid (VMA), and postoperative complications were observed, and postoperative followtwoups were performed.
Results:
All operations were successful. Operative time was 25 to 32 minutes. Perioperative blood pressure was stable in two cases while blood pressure fluctuated in the third case. When the entire tumor and the full-thickness bladder wall at the base were freed, blood pressure reverted to stability. All values of 24-hour urine CA and VMA were within normal limits postoperatively. Patients were followed for 7 to 9 months postoperatively with no recurrence. This series included highly selected patients who were treated by a single senior surgeon who is rich in experience in performing 2013 nm thulium laser procedures.
Conclusions:
To our knowledge, this is the first report of a 2013 nm thulium laser used to treat bladder pheochromocytoma. It can be applied to precisely vaporize and incise the full-thickness bladder wall and cut down the blood supply of the tumor, then peel it while blood pressure remains stable, thus completing partial cystectomy for bladder pheochromocytoma safely.
Introduction
In 1953, Zimmerman and associates 4 reported the first case of bladder pheochromocytoma. These lesions cause generalized symptoms, such as headache, visual burning, diaphoresis, and heart palpitation. The most common symptoms are hematuria and paroxysmal hypertension during micturation. Although clinical symptoms occur in approximtely 83% of cases 5 and elevated levels of urinary metanephrine or resting plasma CAs can suggest the diagnosis of pheochromocytoma (97% sensitivity for the urinary CAs and 99% for plasma CAs), 6 some pheochromocytomas are clinically silent and, in most of those cases, levels of CAs and their metabolites in the blood and urine are found to be normal. 7
In traditional surgical management, most pheochromocytomas are removed by open partial cystectomy. In a review of 100 cases, 7 pheochromocytomas were removed by transurethral resection and 7 by total cystectomy, but most were removed by open partial cystectomy. 5 Some reports showed that while transurethral resection of the bladder tumor (TURBT) is feasible, more rigorous surgical indications and higher surgical techniques are necessary. 8 After TURBT, however, the risk of residual tumors was approximately 23%, checked by open surgery or TURBT again. 9
Because of the endocrine characteristics of pheochromocytoma, touching, squeezing, or resecting of pheochromocytoma may produce a sudden rise in blood pressure, resulting in adrenal crisis. Ensuring the safety of the operation is key, in addition to using α-adrenergic-antagonists, increasing blood volume, and controlling heart rate preoperatively. Suturing the bladder wall around the tumor and blocking the tumor's feed arteries and veins were undertaken in traditional open surgery.
Last year, we developed a new method, transurethral partial cystectomy with a 2013 nm thulium laser, to treat patients with bladder tumors. Because of the laser's characteristics of simultaneous precise vaporization as well as resection, we decided to use the 2013 nm thulium laser for endourologic management of bladder pheochromocytoma.
Patients and Methods
From October to December 2009, three men with pathologically suspected bladder paraganglioma were enrolled in this study. The three men were ages 39, 40, and 62 years. Two of the patients had typical syndromes such as paroxysmal hypertension, dizziness, and heart palpitation related to urination. The third patient presented with a history of dysuria and also had experienced two episodes of dizziness and heart palpitation during urination.
Physical examination showed normal blood pressure. Preoperatively, CT bladder scans showed two patients with exophytic masses behind the trigonal region, and one with an exophytic mass in the anterior wall. Mass diameters were between 1.0 and 3.0 cm. In the plain CT, the densities of the masses were all well distributed soft tissues, with an average CT value of 46.75 Hounsfield units (HU) (Fig. 1). Contrast-enhanced images showed well-distributed reinforcement in mass field, and the average CT value was 81 HU (Fig. 2). The lesions were round or roundish, and had sharp borders. No cystic changes, necrosis, hemorrhage, or calcification was detected.

A oval-shaped lesion located in the left posterior bladder wall was observed with homogeneous signal intensity compared with the gluteus maximus muscle.

Contrast-enhanced images showed well-distributed reinforcement in the same lesion.
These patients were also examined for CA and VMA in total volume urine, which revealed two results in the higher than normal level and one result in the normal range (Table 1). We did perform a biopsy on the first two patients before surgery. Considering the tumor could be pheochromocytoma, we took just a little tissue for biopsy to avoid bleeding, so we could not exactly confirm the pathologic result; the third patient had no biopsy, because the tumor was located on the anterior bladder wall. All patients were given phenoxybenzamine for 2 weeks preoperatively.
BP=blood pressure; Ca=cancer; CA=catecholamine; standard range: 59.1∼266 nmol/24 h; VMA=vanillylmandelic acid; standard range: 8.6∼76.3 μmol/24 h.
We performed transurethral partial cystectomies with the RevoLix 2013 nm thulium continuous-wave medical laser surgery treatment system. Energy is transmitted through a 550 μm optical fiber, and power was set to between 40 and 50 W. We used a 26F 30-degree laser resectoscope (Karl Storz, Tuttlingen, Germany). Surgery was performed using general anesthesia. Patients were placed in the lithotomy position. Glycine solution (15 g/L) was used as the operative rinse solution.
After inserting the laser resectoscope into the bladder, we observed that the tumors were completely covered by mucous membrane, with a smooth surface and some enlarged veins (Fig. 3). The two lesions located in the posterior vesical wall were not touched by the fiber probe while the normal mucous membrane, submucosa, muscle layer, and fibrous connective tissues in the outer bladder layer about 0.5 to 1.0 cm from the tumors were being vaporized and incised. Then, the tumors were immediately peeled. Blunt stripping was performed with the laser resectoscope tip along the loose spaces between the detrusor muscle and the outer connective tissue layers. These procedures were continued until the entire tumor and the full-thickness bladder wall at the base were freed.
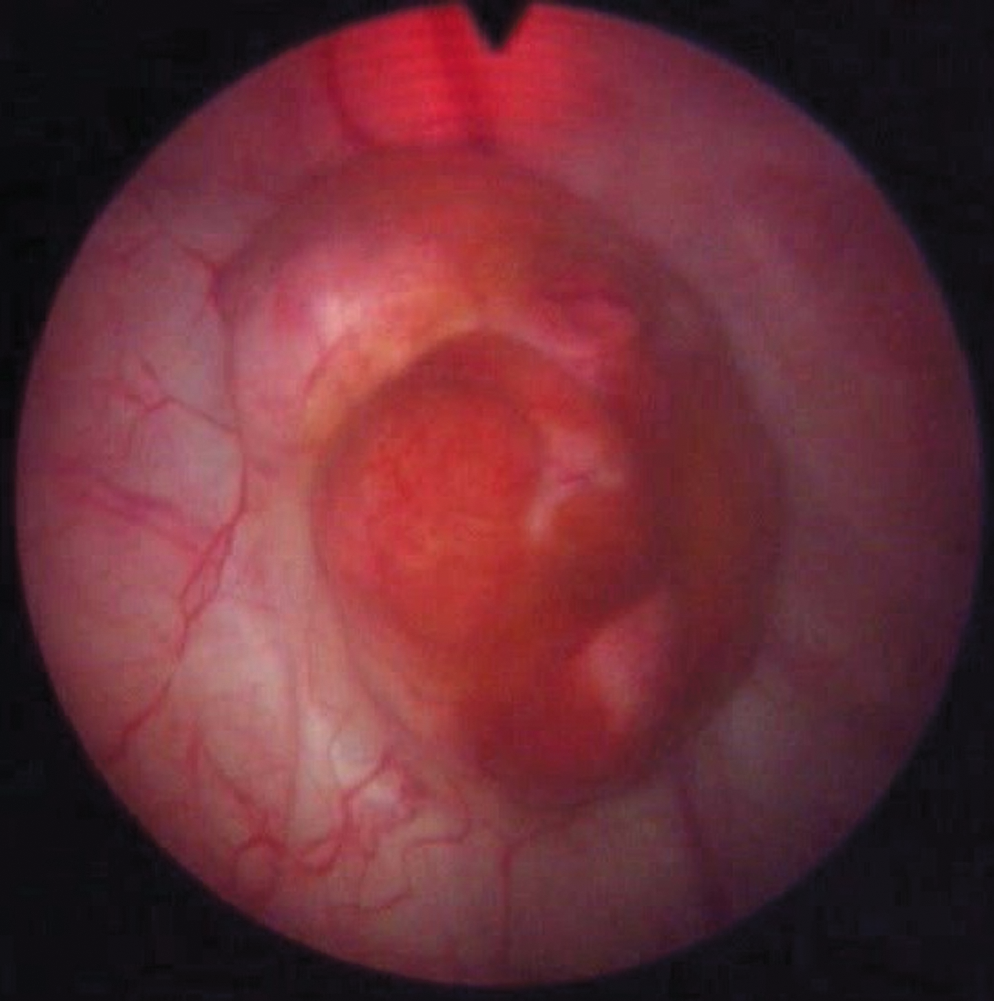
The tumor was completely covered by mucous membrane, with a smooth surface and some enlarged veins.
The third lesion was located in the inferoanterior wall. Because the fiber probe was not flexible, we could not incise a full circle around the tumor, so the whole bladder wall was vaporized and incised around approximately 75% of a circle, to reduce the lesion's blood circulation. Then the tumor was incised piece by piece, and the base bladder wall was vaporized down to the fibrous connective tissues in the outer bladder layer.
The intact tumor specimens and their basal layers were obtained with an extractor. There was a craterlike change in the bladder wall at the tumor excision site, and the incision margin was smooth (Fig. 4). At the end of laser resection of the bladder lesion, and after irrigation and drainage, the bladder mucosa appeared well approximated. The urinary catheter remained indwelling for 7 to 9 days postoperatively, and no bladder irrigation was needed.

Shell-hole-like change in the bladder wall at the tumor excision site, and the incisal margin smooth.
Results
All operations were successful, and all patients tolerated the surgery well under general anesthesia. Mean operative time was 25 to 32 minutes (mean time was 30 min) per patient. Perioperative blood loss was minimal. No patient experienced obturator nerve reflection or postoperative hemorrhage.
As Table 2 and Figure 5 show, at the beginning of the operation, blood pressure was lowered in all three patients to prevent sharp fluctuations. Blood pressure was generally stable in case 1 and case 2 during the operation, but in case 3, blood pressure fluctuated while the tumor was being peeled (peeling in each case took 10–20 min). In case 3, when the entire tumor and the full-thickness bladder wall at the base were freed, blood pressure reverted to stability.

Intraoperative blood pressure change.
The preoperative values of 24-hour urine CA and VMA of two patients decreased significantly, with CA values decreasing from 429 nmol and 241.5 nmol to 205.2 nmol and 173.1 nmol, respectively; VMA values decreased from 64 μmol and 69.1 μmol to 31.3 μmol and 51.1 μmol, respectively. For the third patient, the preoperative normal values of 24-hour urine CA and VMA were still within normal limits postoperatively (Table 1).
We can obtain complete tumor specimens after this partial cystectomy surgery, and the edge of the tumor base can be distinguished clearly. Edges were carbonized, but the base was still fresh because of the blunt dissection. Pathologic examination of the specimens revealed benign pheochromocytoma. The mean diameter of tumor was 1.5 cm. Immunohistochemistry inspection showed chomogranin A(+), synaptophysin(+), CD56(+++), Ki-67(+< 2%), creatine kinase (−). Patients were followed up for 7 to 9 months.
Discussion
The 2013 nm thulium continuous wave laser working pattern is vaporization plus resection. In clinical practice, it is effective for hemostasis, smoothing the injured area, and removing tissue and has few complications. 10 The 2013 nm thulium laser can completely excise the whole detrusor muscle layer of the bladder and precisely strip the muscle layer from the outer layer of connective tissue. Surgery was uneventful. After the tumor and the whole muscle layer at its base were completely peeled off, we clearly saw off-white outer layer connective tissue. Because blunt stripping was the primary method to treat the whole muscle layer, with laser vaporization and incision used only in auxiliary fashion during the operation, it was performed in a clear operative field. There was minimal hemorrhage perioperatively, the histologic structure was clear, the range of excision was precise, and the operation was easy to control. 11
Vaporesection with the 2013 nm thulium continuous wave laser has already been used successfully as a minimally invasive treatment for patients with bladder tumor. Because of its characteristics of simultaneous precise vaporization, as well as resection and bladder wall anatomic characteristics, we applied the 2013 nm thulium laser for endourologic management of bladder pheochromocytoma.
These patients were treated by transurethral partial cystectomy with 2013 nm thulium laser, which is minimally invasive but with results similar to those of open surgery. For the two lesions located in the posterior vesical wall, the full thickness bladder wall was vaporized and incised to the outer bladder layer about 1.0 cm circularly with the 2013 nm thulium laser. It blocked the arteries and veins before the fiber head touched the tumors. In this way, even if the tumors were stimulated in the subsequent steps, blood pressure remained stable in a safe range. Then, blunt stripping was performed with the laser resectoscope tip along the loose spaces between the detrusor muscle and outer connective tissue layers until the entire tumor and the full-thickness bladder wall at the base were freed. Tumors prominent in the bladder or hidden in the bladder muscle layer could be resected completely.
For the third tumor, which was located in the anterior wall, incision of the full-thickness bladder wall around the tumor circularly could not be accomplished because of the limitations of the optical fiber. Consequently, after the bladder wall was vaporized and incised about three-quarters circle, the tumor was resected piece by piece with laser. In this situation, the patient's blood pressure increased significantly to 160/105 mm Hg. When the tumor was resected completely and the full-thickness bladder wall at the base was vaporized to the outer connective tissue layers, blood pressure returned to normal. After that, when the tumor bases were stimulated again, no blood pressure fluctuation was noticeable.
In these procedures, we can see that it is important to block the tumor's blood circulation early in the operation. Circular incision of the bladder wall around the tumor by transurethral partial cystectomy with 2013 nm thulium laser can achieve this goal.
Because the 2013 nm yhulium laser has no field effect, it is perfect for excising tumors in the lateral bladder wall. There was no obturator nerve reflex in the operations on tumors in the lateral bladder wall. Thus, the safety of the operation was enhanced. 12
Cystoscopy is a common method for accomplishing pheochromocytoma diagnosis and transurethral resection. It can not only locate a tumor, but also can determine its qualities by biopsy. It can inspect tumor size, shape, and location, which is important for surgical decisions. Bladder pheochromocytomas are usually solitary and attached to the bladder wall with a broad base. They are located in the bladder dome and the triangular region.
Cystoscopy shows an exophytic tumor in 84% of pheochromocytomas; otherwise, the mass is included in the bladder wall. The tumor is usually covered by mucosa, which may appear normal, hypervascular, or superficially ulcerated. Because of the possibility of false negatives, bleeding, hypertension, headache, and dizziness, etc, in cystoscopic biopsy, however, some physicians do not advocate it.
The bladder filling provocation test used in the diagnosis of bladder pheochromocytoma should be avoided in patients who are undergoing transurethral surgery, because without previous preparation, it may have deadly consequences 13 —ie, hypertensive crisis. It is important to control the volume of fluid in the bladder to reduce the risks of blood pressure fluctuation. In our surgery group, intravesical liquids were controlled at 150 to 200 mL to help ensure stable blood pressure in the initial stage of the operation.
Extra-adrenal pheochromocytomas often have multiple lesions, so urinary CA and VMA levels need to be checked 1 week after surgery. This can show whether all pheochromocytomas are completely removed. We reviewed 24-hour urine CA and VMA for our patients after the surgical procedure, and the results showed normal. Because follow-up was short, however, the long-term curative effects and complications have not yet been observed.
Analyzing the surgical procedure for our patients, we believe that resection of the tumor directly would have created much higher risk. Using the 2013 nm thulium laser partial cystectomy enhanced the safety of the surgery. According to indications in the treatment of bladder cancer, we propose that tumors less than 3 cm in diameter can be treated with this procedure. For tumors in the anterior and roof walls of bladder, however, there are still some difficulties in the operation.
Conclusions
Using 2013 nm thulium laser partial cystectomy to treat patients with bladder pheochromocytoma is a new endeavor in our clinical practice. As evidenced by this surgical experience, we believe that this minimally invasive treatment is applicable to some bladder pheochromocytomas and provides a viable option for the management of small-volume bladder pheochromocytoma.
Footnotes
Disclosure Statement
No competing financial interests exist.