
Abstract
Ureteral avulsion during ureteroscopic stone management is extremely rare. To date, many publications reporting avulsion have been associated with “blind basket extraction” under fluoroscopy and the use of the Dormia stone basket. Fortunately, despite the significant rise in the numbers of ureteroscopic cases being performed, the rate of ureteral avulsion remains low. This is likely in part because of improvements in ureteroscope technology and stone manipulation devices. We present three recent cases of ureteral avulsion referred to our center for further management. To our knowledge, these cases represent the first published description of avulsion where the ureteroscope became wedged in the intramural ureter, resulting in full-length avulsion of the ureter. The avulsion occurs both proximally and distally with a resultant length of ureter left attached to the ureteroscope. We dub this mechanism the “scabbard” avulsion. We describe the most likely mechanism of this injury, with suggestions on how to prevent it and how to release the ureteroscope should it become wedged in the intramural ureter.
Introduction
Technologic advances over the past 30 years have resulted in smaller and more flexible semirigid endoscopes, which have made ureteroscopy a more effective, safer, and less morbid procedure. Major complications after ureteroscopic stone management, particularly in experienced hands, are rare at 0% to 2%. 8 –10 The most feared complication is avulsion of the ureter, which often results in a complicated postoperative course for the patient and possible loss of the renal unit involved. Surgical options in this situation include ureteral reimplantation with or without Boari flap or psoas hitch, ileal ureter, autotransplantation, or nephrectomy. Unfortunately, ureteral reimplantation is rarely possible, because the ureter is usually avulsed from the ureteropelvic junction (UPJ), with loss of its blood supply.
Before the modern era of ureteroscopic stone management, cases of ureteral avulsion in the literature tended to center around the use of the Dormia basket to extract stones in a blind fashion. 11 To our knowledge, this is the first report of ureteral avulsion occurring in which the ureteroscope became wedged in the intramural ureter, resulting in full-length avulsion of the ureter. This report highlights three cases referred to our center for management after what we describe as two-point or “scabbard” ureteral avulsion. They involve proximal and distal discontinuity of the ureter, with a resultant scabbard, as the ureter is withdrawn as a sheath on the ureteroscope (Fig. 1).
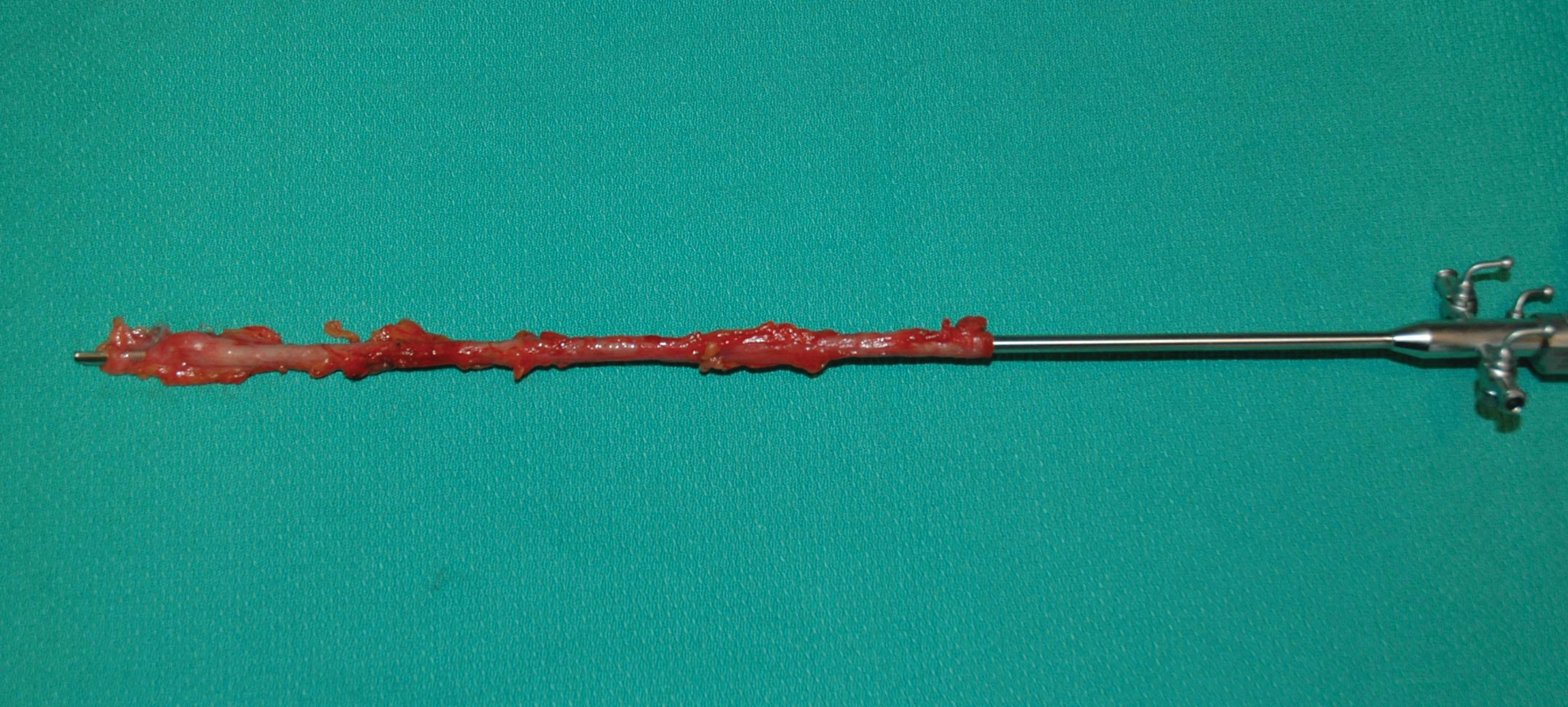
“Scabbard” of ureter on the withdrawn semirigid ureteroscope, with ureteral orifice intact.
Case 1
A 44-year-old man underwent ureteroscopic management of an 8-mm proximal ureteral stone using a 34-cm 27411K Storz semirigid ureteroscope. Details of the operative procedure were obtained from the referring urologist. The ureteroscope measured 8F at the tip and increased in diameter to 9.5F along the proximal shaft. The scope was advanced over a guidewire without dilation of the orifice. There was no safety guidewire. The ureteral lumen was reportedly visualized the entire time. The scope felt “tight” in the ureter, and some pressure was needed to advance the final few centimeters to the stone.
Once identified, the stone was entrapped in a 3F N-circle stone basket and treated with a 365 μ holmium laser fiber placed through the same working channel until a fragment approximately 3 to 4 mm was left remaining. At this point, withdrawal of the ureteroscope was attempted, but the scope appeared to be “stuck” in the ureter. A twisting motion was applied, combined with traction, and a sudden feeling of “give” was experienced, after which the scope was able to be withdrawn easily. The stone was noted to be passing freely over the urothelium, indicating to the treating urologist that the stone fragment was being withdrawn without obstruction. A second point of restriction was then felt, although the stone was still moving freely in the ureter. With further traction on the scope, a “popping” sensation was felt.
At this point, the ureteroscope was withdrawn from the urethra, and a scabbard of the entire ureter was present along the length of the ureteroscope. The ureteral orifice was intact, and the intramural ureter was noted to be tightly attached to the ureteroscope, making it difficult to remove it from the wide 9.5F proximal end of the scope.
After referral to our center, we staged the injury and attempted to control urinary leakage into the retroperitoneum with placement of a nephrostomy tube with the use of intravenous contrast and fluoroscopy. Figure 2 shows the resultant pyelogram, revealing an intrarenal pelvis and no definite proximal ureter. A nephrostomy tube could not be placed because of a collapsed collecting system from extravasation. After discussion with the patient, presenting the options of attempted reconstruction or nephrectomy, the patient elected to undergo an urgent simple laparoscopic nephrectomy. Figure 3 demonstrates the proximal nature of the avulsion at the UPJ, leaving only a small intrarenal pelvis. The patient convalesced well and was discharged home on the third postoperative day with a normal serum creatinine level.
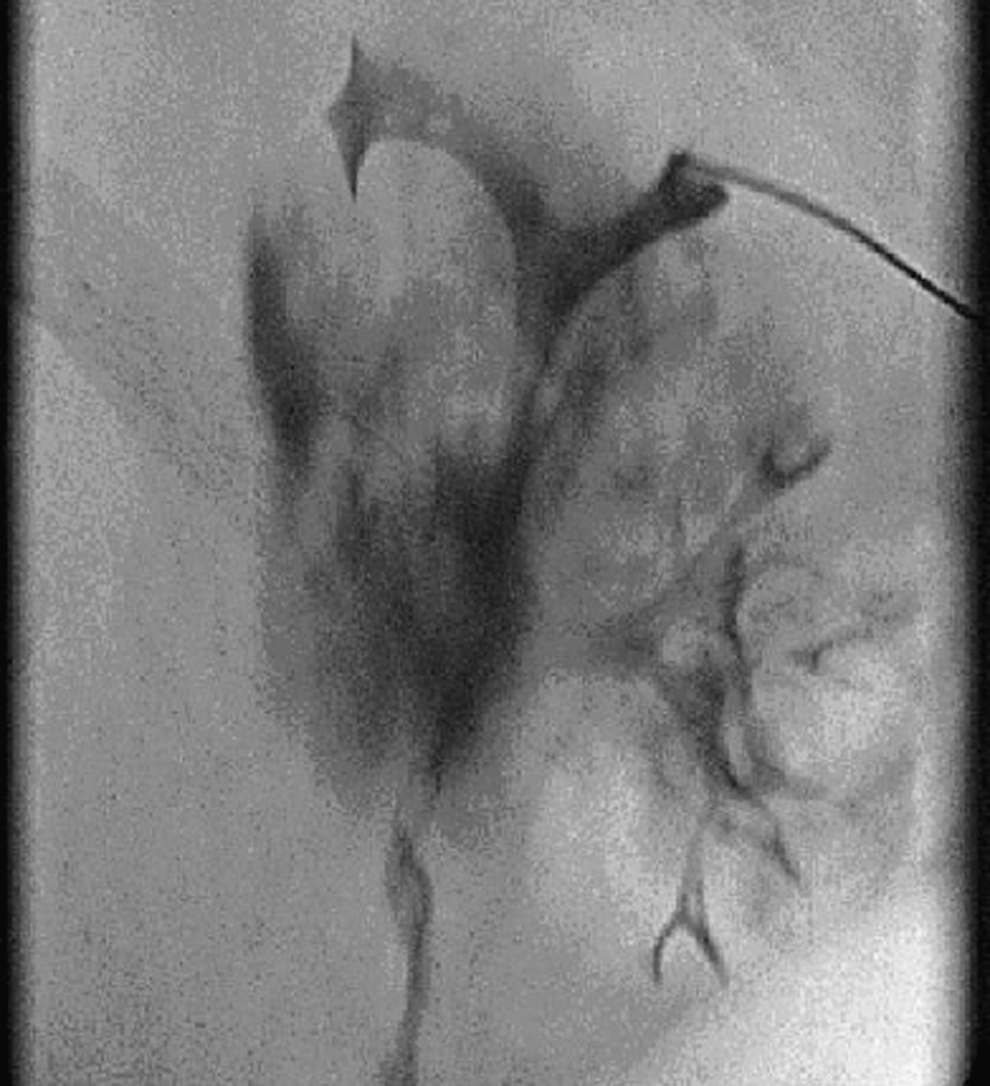
Nephrostogram at the time of attempted percutaneous nephrostomy tube insertion. Note the extravasation of contrast from the region of the ureteropelvic junction, passing down the periureteral sheath of tissue left by the avulsion.
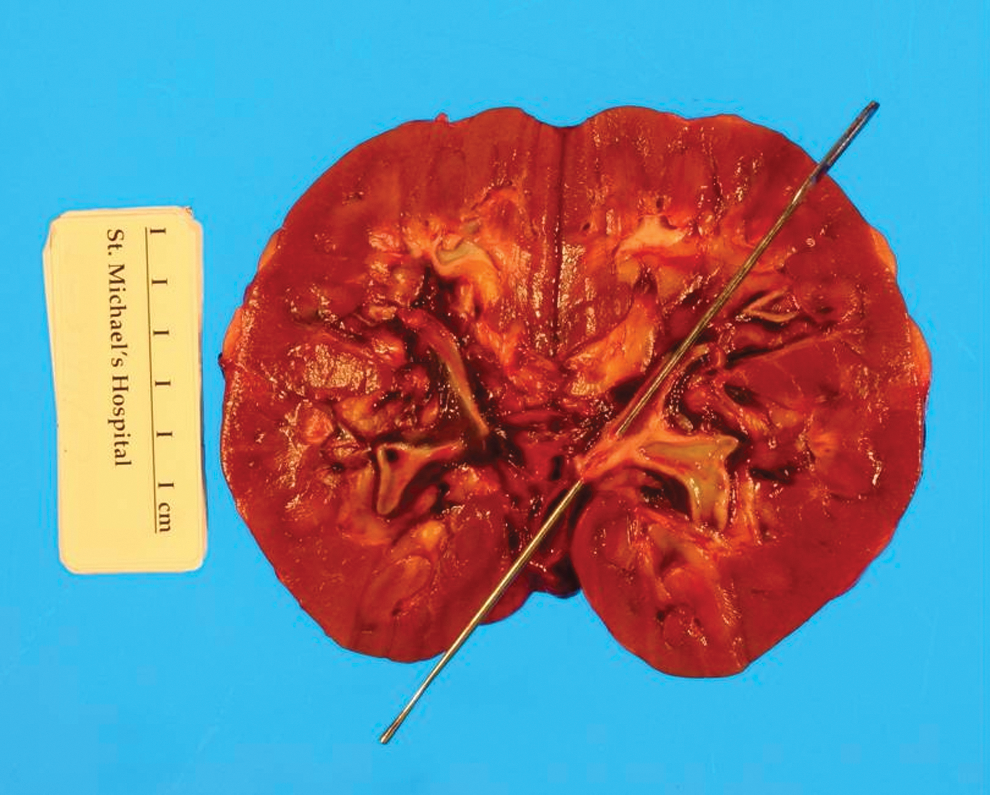
Pathologic specimen reveals complete avulsion of the ureter at the level of the ureteropelvic junction. Note the small intrarenal pelvis.
Case 2
A 51-year-old woman was referred to our unit after a left ureteral avulsion that occurred during ureteroscopy and stone manipulation with a Wolf semirigid ureteroscope. This scope measured 8F at the tip with a more proximal diameter of 9F. In this case, the stone was completely fragmented, and difficulty was experienced removing the ureteroscope at the end of the case. The avulsion of the ureter occurred with a similar resultant “sheath” of ureter left on the scope. Again, the ureterovesical junction (UVJ) was tightly adherent to the proximal end of the scope. In this case, a nephrostomy was placed before referral and the resultant nephrostogram revealed 1.5 to 2 cm of intact proximal ureter. Again, after a discussion of the management options with the patient, she elected to undergo a laparoscopic nephrectomy.
Case 3
A 67-year-old woman was found to have retroperitoneal adenopathy and a left pelvic mass. Biopsy of the nodal mass demonstrated the presence of poorly differentiated carcinoma that was thought to be either genitourinary or gynecologic in origin. At the referring center, she underwent cystoscopy and bilateral retrograde pyelography to rule out upper tract urothelial carcinoma. The left retrograde pyelogram revealed an unusual filling defect at the UPJ, leading to semirigid ureteroscopy for further evaluation. During ureteroscopy, a stricture was encountered within the distal ureter that was dilated to 10F diameter with graduated ureteral dilators. After dilation, the semirigid ureteroscope could be passed up to the UPJ, where a stricture was identified that was consistent with the filling defect previously seen on retrograde pyelography. No tumor was identified.
With an attempt to remove the ureteroscope, it became clear that there was little movement of the ureteral wall in relationship with the tip of the ureteroscope, and the ureteral wall appeared to be moving with the ureteroscope. More force was needed to remove the ureteroscope, and as the scope was removed from the bladder, the ureter could be seen forming a sheath on the ureteroscope and intussuscepting out through the urethra. At this time, a decision was made to loosen the ureter from the ureteroscope and pass the scope back into the bladder. The scope was navigated along the guidewire and up the intussuscepted ureter, ultimately manipulating the scope up to where it became obvious that it was within the retroperitoneal space. The ureteroscope was removed again leaving the avulsed ureter in the retroperitoneum. A Foley catheter was placed and the safety guidewire, which was still in place, was left protruding from the urethra.
The patient was awoken from anesthesia. After discussing the complication and previously diagnosed malignancy with the patient and her spouse, a decision was made to proceed with an immediate emergency laparotomy at the referring center. At the time of the laparotomy, the left pelvic mass and adnexal structures were removed and sent for pathologic examination. Exploration of the retroperitoneum revealed that the ureter had been completely avulsed proximally at the UPJ and distally at the UVJ. The completely detached ureter was removed with the previously placed guidewire running through it. Mobilization and dissection of the left kidney revealed significant hilar adenopathy. An intraoperative decision was made not to perform a nephrectomy to maximize renal function for systemic therapy for the metastatic carcinoma. The UPJ was identified and ligated. A left percutaneous nephrostomy tube was then placed postoperatively. She was subsequently diagnosed with ovarian cancer and completed a course of carboplatinum with a good response before referral to our center.
At the time of her referral to our unit, her serum creatinine level was normal at 95 μmol/L, and a renal scan showed her differential function to be 59% on the right and 41% on the left. Neither reconstruction with an ileal ureter nor autotransplantation was considered to be a reasonable management option in this patient with her potential reduced life expectancy related to her metastatic ovarian cancer and the previous finding of renal hilar adenopathy. A simple nephrectomy was accepted by the patient as the quickest way to optimize her quality of life.
Discussion
The incidence of ureteral avulsion during ureteroscopic stone management has been reported in 0% to 2% of series 8 –10 and fortunately does not seem to be increasing, despite an increase in the number of ureteroscopic cases being performed worldwide. The cases presented here are complicated by both upper and lower ureteral disruptions, creating the most challenging circumstance for reconstruction, because little or no ureter remains. In neither of the stone cases had predilation of the ureteral orifice been undertaken, but it has been shown that ureteroscopy without routine balloon dilation is effective with minimal complications. 12
It is alarming to consider that the proximal shafts of the semirigid ureteroscope used in the first two cases were 9F and 9.5F, respectively, well below the outer diameter of many commonly used ureteral access sheaths that are typically in the 12F to 14F range. The difference probably lies in the fact that the sheaths have a hydrophilic coating or are generously lubricated before passage. Also and more importantly, even with an extrastiff or superstiff guidewire, only a limited amount of force can be applied before the sheath buckles and cannot be advanced further.
Conversely, in the cases with the ureteroscope already up the ureter, there is no limit to the amount of force that may be applied. The degree of force applied is limited only by the sense and experience of the operator. In the cases described, it is clearly the excessive force applied to reach the very proximal ureter that wedged the largest diameter portion of the scope in the tight intramural ureter.
Between the fourth and sixth week of fetal development, extrophy of the mesonephric ducts into the posterior wall of the developing bladder brings the ureteral bud openings into the bladder wall. 13 This separate developmental origin of the intramural ureter and the bladder wall results in a cleavage plane between the two. Excessive force on a ureteroscope, tightly impacted in the intramural ureter, could result in a complete avulsion of the intramural ureter from the bladder wall. Because the ureter is freely mobile and elastic within the retroperitoneum, further traction on the ureteroscope would allow free withdrawal until the ureter is taut, tethered to the kidney by the UPJ. Any further force could result in disruption of the UPJ, leaving the ureter ensheathing the ureteroscope as if it were a scabbard on a sword.
It has been stated that “ureteral avulsion should never occur,” 14 and before the presentation of these three cases to our center, this was our teaching. Classic ureteral avulsion involves the use of excess force to extract a stone that is too large to come out through the lower ureter. In the modern era of holmium laser lithotripsy, it is possible to pass a laser fiber through the working channel alongside a basket and fragment the stone, or disengage the stone from the basket, because such avulsion from attempting to extract a stone that is too large should not occur. In the stone cases described above, however, sound ureteroscopic principles with regard to stone fragmentation and extraction were used; unfortunately, in these cases, the avulsion was likely related to the excessive degree of force used to advance and remove the scope.
While we are not cautioning against the use of semirigid ureteroscopy above the iliac vessels, one must be aware that with the use of graduated ureteroscopes with a larger proximal diameter, the larger proximal end can be tightly wedged in the distal ureter and even become impacted. Any attempt to use further force to reach a more proximal stone must be avoided.
Although this is purely speculative, two stone cases reported above did not use a safety guidewire. Perhaps the presence of a guidewire between the shaft of the ureteroscope and the ureteral wall would prevent such tight impaction.
We would like to suggest other techniques that may be used in an attempt to avoid this unusual type of avulsion. First, if a stone cannot be easily reached with a shorter graduated semirigid ureteroscope, one can always change to a longer semirigid scope or abandon in favor of a flexible approach. Second, while lubricating jelly is often applied only to the first few centimeters of the semirigid ureteroscope, in cases of more proximal calculi, lubricant should be applied along the entire length of the shaft.
Third, if the urologist finds it difficult to advance the ureteroscope despite full visualization of the lumen and senses that the scope feels tight in the ureter (likely at the UVJ in these cases), the scope should be withdrawn immediately and either replaced with a smaller caliber scope, reinserted after ureteral dilation, or ureteroscopy should be repeated on a later occasion after placement of a ureteral stent to allow ureteral dilation.
Finally, what should one do if faced with a semirigid ureteroscope wedged within the intramural ureter? It is our suggestion, although not previously attempted, that a second semirigid ureteroscope is passed into the bladder beside the first and the situation evaluated. If traction on the first ureteroscope results in intussusception of the orifice into the bladder, one has the situation described in the previous cases. We would suggest that a holmium laser is then used via the second ureteroscope to perform a ureteral meatotomy on the medial aspect, extending as far proximally as is necessary to release the impacted ureteroscope. If there is no safety guidewire present, this must be placed through the first ureteroscope, before its removal, for subsequent placement of a stent.
Conclusion
Ureteral avulsion is extremely uncommon in the present era of smaller ureteroscopes and holmium laser lithotripsy. We have reported on three cases of complete scabbard avulsion, where the ureter forms a sheath on the ureteroscope. Techniques to avoid this complication are suggested, and a procedure to free up the impacted ureteroscope should this occur is described.
Ureteroscopic stone management results in successful, uncomplicated outcomes in the majority of cases. Given that major complications are rare, it is important to be aware of various mechanisms by which they may occur in order to prevent them. Patients should be counseled that, while renal loss secondary to avulsion might occur during ureteroscopy, it is exceedingly rare.
Footnotes
Disclosure Statement
No competing financial interests exist.