
Abstract
Purpose:
The aim is to report our 1-year experience in transumbilical Laparoendoscopic single-site (LESS) radical nephrectomy (LESS-RN) and assess its learning curve.
Patients and Methods:
From September 2009 to December 2010, 18 consecutive patients with a solitary renal tumor underwent transumbilical LESS-RN. We grouped measured parameters on the basis of the first nine (group A) and last nine (group B) patients, and compared both subgroups with the control group (C), which was composed of the initial nine consecutive patients who underwent conventional laparoscopic RNs performed by the same surgeon.
Results:
There was one LESS patient converted to conventional laparoscopic surgery for intraoperative hemorrhage and transfused. The mean for measured parameters of the groups A, B, C were: age: 58.6, 57.2, and 59.2 years, respectively (P>0.05); American Society of Aneshesiologists score: 1.9, 2.0, and 2.0, respectively (P>0.05); body mass index: 25.2, 23.5, and 23.1 kg/m2, respectively (P>0.05); lesion size at CT scan: 5.0, 4.6, and 6.2 cm, respectively (P=0.039); operative skin to skin time: 191.6, 123.9, and 122.2 minutes, respectively (P=0.000); estimated blood loss: 172.2, 246.7, and 116.7 mL, respectively (P>0.05); incision length: 5.6, 5.9, and 7.4 cm, respectively (P=0.000); hospital stay: 5.8, 5.8, and 5.8 days, respectively (P>0.05). At the latest follow-up, all patients did not present any local recurrence or metastasis.
Conclusions:
In selected patients, the transumbilical LESS-RN can be safely performed with favorable outcomes. While a learning curve certainly exists, it appears to be short for an experienced laparoscopic surgeon.
Introduction
A great number of technical innovations had made possible the reduction of the size and number of ports, which was intensified with the advent of the first single-port surgery case reported by Rane and associates 3 in 2007. Later, this novel surgical style was well described as laparoendoscopic single-site (LESS) surgery in 2008. 4
Subsequent work has greatly expanded its indications into almost the whole spectrum of conventional laparoscopic surgery in urology. 5 The role of LESS in RN, however, has been fiercely debated, because the incision must be extended for intact specimen extraction. We present our series of 18 patients who underwent transumbilical LESS-RN to further accumulate clinical evidence, which may help to fully elucidate its overall benefit and clear role.
Patients and Methods
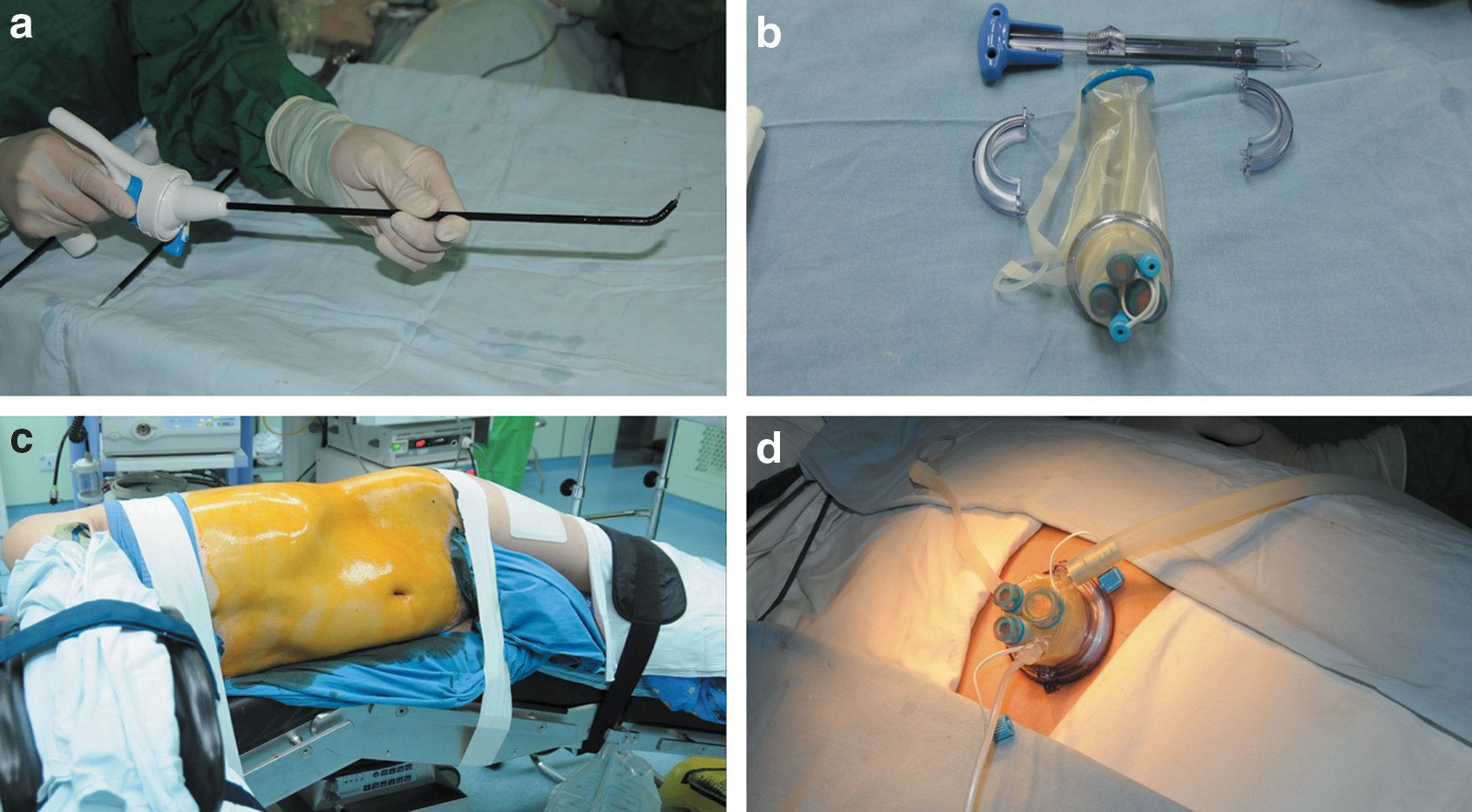
Between September 2009 and December 2010, 18 patients underwent transumbilical LESS-RN via a multichannel TriPort™ (Fig. 1b) (Advanced Surgical Concepts, Wicklow, Ireland) through a 2 to 3 cm incision by a single experienced urologist at our center. The main criteria of patient selection were patients with stage T1b tumor for whom RN was indicated, those with a lower body mass index (BMI) (≤30 kg/m2), and those with no previous abdominal surgery or renal vascular anomalies. Additional criteria were T1a tumors that were not suitable for partial nephrectomy (localized in hilum, significant involvement of pelvicaliceal system, or patients' decision to undergo radical procedure). The LESS subject group was composed of 12 male and 6 female patients. Mean age was 57.9±8.75 years and mean BMI was 24.3±2.20 kg/m2.
After counseling all the patients regarding all the surgical options, the final decision was made to proceed with the LESS-RN. All patients consented specifically in writing to the LESS-RN approach and ancillary incisions/ports or open conversion if necessary intraoperatively.
American Society Anesthesiologists score (physical status classification system) and perioperative data (Table 1) including operative time, estimated blood loss, transfusion, additional ports, or conversion to standard laparoscopy or open surgery, length of incision measured with a ruler at the end of the procedure (Fig. 2d), length of postoperative hospitalization, intraoperative and postoperative complications, pathologic results, and short to intermediate term follow-up data were prospectively recorded. Postoperative complications were classified according to the Clavien grading system. 6

LESS=laparoendoscopic single-site; CL=conventional laparoscopy; BMI=body mass index; ASA=American Society of Anesthesiologists; OT=operative time; EBL=estimated blood loss; LOS=length of stay; ss=statistically significant; all other comparisons were nonsignificant.
Patients were regularly followed up with the appropriate studies at 3, 6, and 12 months after surgery and once a year thereafter. Cancer patients were evaluated by CT scan at 6 and 12 months after surgery, and then every 12 months if there was no evidence of recurrence or metastasis.
To evaluate the difficulty of the LESS technique in RN and its learning curve, we divided all parameters on the basis of the first nine (group A) and last nine (group B) patients, and compared both subgroups with the control group (C). The control group was composed of the initial nine consecutive patients who underwent conventional laparoscopic RNs performed by the same surgeon from December 2007 to March 2008.
Statistical analysis was performed with the one-way analysis of variance, Student-Newman-Keuls-q test, and chi-square for continuous and categorical variables, respectively. Statistical significance was set at P<0.05 and all P values were two-tailed. Parameters were evaluated using SPSS v. 16.0 (SPSS, Inc, Chicago, IL).
After general anesthesia, the patient was placed in a standard lateral decubitus position (Fig. 1c). A 2 to 3 cm single longitudinal transumbilical incision was made and extended down to the level of the peritoneum. The single-port device was inserted into the abdominal cavity with a specialized introducer, and insufflation commenced with a pressure limit of 15 mm Hg (Fig. 1d). The characteristics and technique of insertion were similar to that described by Gill and colleagues 7 and Rane and Rao. 8 A 5-mm 30-degree rigid video-laparoscope (EndoEYE, Olympus Surgical, Orangeburg, NY) was placed through one of the 5-mm channels, and initial observation of cavity was without abnormal findings. The subsequent steps in the procedure were identical to those of conventional transperitoneal laparoscopic RN completed with the combination of rigid and flexible laparoscopic instruments, Autonomy Laparo-angle™ (Cambridge Endo, Framington, MA) (Fig. 1a).
An ancillary 5-mm trocar was applied to facilitate spleen retraction with a grasper during our first two procedures via a skin incision in the anterior axillary line below the 12th rib. Individual dissection of the renal artery and vein was undertaken and ligated with Hem-o-lok clips (Weck, Research Triangle Park, NC) and titanium clips (Olympus, Tokyo, Japan), doubly clipped on the body side, singly on the specimen side and transected. In two patients, the renal pedicle was controlled with EndoGIA linear staplers similarly to that performed in conventional laparoscopic RN (Fig. 2b).
The intact specimen was placed into an EndoCatch bag (Covidien, Norwalk, CT) and extracted with the TriPort synchronously. A drainage catheter was left in situ through the primary single umbilical incision, carefully sutured to avoid possible complications.
Results
The detailed perioperative data of the whole cohort are presented in Table 1. Of the 18 LESS patients, 15 cases were completed successfully. A 5-mm ancillary trocar was needed in the first two cases for retraction. Hem-o-lok clips for vascular control were used in 16 cases while vascular EndoGIA staplers were used in two cases. There was one patient whose operation was converted to conventional laparoscopic surgery for intraoperative hemorrhage from inadvertent injury of an anomalous renal artery branched from the celiac trunk and required transfusion.
Mean operative duration was 157.7 minutes (range 70–245 min) with an estimated blood loss of 209.4 mL (range 20–1100 mL). There was an obvious trend toward a decreasing operative time from case 1 to case 18 (Fig. 3). Mean length of incision was 5.7 cm (range 5–7 cm). Mean tumor size was 4.8±1.67 cm. The recovery was uneventful, and transient postoperative fever up to 38.6°C (Clavien grade I) developed on only the patient who received the transfusion. No major postoperative complications occurred. Mean stay of hospitalization was 5.8±1.40 days.

The trend of operative time with each consecutive case (except the #16 case that was converted to standard laparoscopy).
Results of one-way analysis of variance under the significant level of 0.05 indicated statistically significant differences among the groups of A, B, C on the mean tumor size, mean operative time, and mean incision length (P=0.039, 0.000, and 0.000, respectively). The difference of all the above three parameters was statistically significant between group A and group C. No statistical significance was observed, however, for any of the considered parameters between group A and group B except the variable of the mean operative skin to skin time. For group B and group C, the difference on the mean tumor size and mean operative time were statistically significant (Table 1).
Pathologic examination revealed organ-confined malignant lesions in all cases. In the LESS group, there were 17 renal-cell carcinoma (RCC) and 1 sarcomatoid carcinoma, and 6 pT1aN0 and 12 pT1bN0, respectively. The grading according to Fuhrman was 4 G1, 12 G2, and 2 G3. In the conventional laparoscopic group, all cases were RCC—seven clear-cell and two papillary—with a stage distribution of one T1a, four T1b, and four T2 tumors.
The mean follow-up time of the LESS group was 8.0±4.6 (range, 3–18 mos). All patients did not present any local recurrence or metastasis, with a single scar (Fig. 4).

Healed umbilical incision 6 months after transumbilical laparoendoscopic single-site left radical nephrectomy.
Discussion
Ever since Clayman and coworkers 9 reported the first clinical laparoscopic nephrectomy in 1991, urologists have been at the forefront of surgical innovations and technologic refinements. Many innovations regarding surgical techniques and technologies have been developed to decrease the size of incision and the number of ports needed for safe laparoscopic surgery. LESS, regarded as the latest evolution in laparoscopic surgery, is referred to as a single small skin incision approach through which all instruments and scope are introduced, enabling surgeons to perform surgery with a single scar. The milestone was the first LESS nephrectomy reported by Rane and associates 3 in 2007. Within a short span, the LESS technique has gained worldwide acceptance, and a great deal of initial experience has been described in the literature. 5
Initially, investigators remained extremely cautious and selective in applying LESS technique for oncologic indications. To date, the experience in LESS-RN is still in its infancy, with approximately 100 cases reported from different centers. 10 –17 The operative outcomes of the present study were comparable to those of previous anecdotal studies in LESS-RN (Table 2).
OT=opertive time; EBL=estimated blood loss; LOS=length of stay.
From our experience of two cases, the vascular EndoGIA stapler can be safely used during LESS-RN for hilar control. Especially with a complex renal vascular presentation, the renal artery and the renal vein can be addressed together with an EndoGIA stapling device. In those two patients, the renal veins were surrounding the renal artery in a pampiniform form, and there was little chance that the artery could be dissected free from the veins. Nevertheless, cautions must be taken in that EndoGIA misfire may occur if a dense structure (ie, fibrotic or calcified vessel, etc.) is inadvertently caught within the jaws during engagement.
Raman and colleagues 18 first reported the LESS-RN in 2007, followed thereafter by Kaouk and coworkers 19 in their initial LESS series in 2008 and a more detailed description by Stolzenburg and associates 12 in 2009. Raman and colleagues 20 reported the first case-control study comparing 11 LESS with 22 laparoscopic nephrectomies. The results revealed that there was no difference in median operative time, percent decrease from preoperative hemoglobin value, analgesic use, length of stay, or complication rate between these two approaches. The superiority of LESS over conventional laparoscopic nephrectomy was merely a nonspecifically measured or quantified cosmesis. Notably, that study was susceptible to its inclusion of patients with an enhancing mass (55%) as well as those with a nonfunctioning kidney (45%) where the extension of the incision was not needed, possibly blunting the whole results. More recently, several comparative series of LESS nephrectomy vs standard laparoscopy have become available. 21 –23 The predominant advantage, however, stays as the subjective cosmetic improvement with the additional benefits of decreased postoperative pain and shorter hospital stay to be determined.
Despite the retrospective and anecdotal nature of our study, to the best of our knowledge, it is among the largest series for such a single disease entity and the first to evaluate the learning curve of the LESS-RN. As was reported, technical difficulty was encountered during our experience. First, ambidexterity was necessary in that the instruments are often crossed at the entry point in the port. Second, loss of triangulation, instruments clashing, and limited working space is inevitable but could be partially overcome by the application of flexible instruments.
Vascular control is the most challenging step during the procedure, and bleeding is the most common complication reported. 2 We excluded patients with renal vascular anomalies. There was one patient with an anomalous renal artery branched from the celiac trunk that was not identified preoperatively. Inadvertent injury and uncontrollable hemorrhage occurred intraoperatively; the procedure eventually necessitated conversion to conventional laparoscopic surgery. In this regard, preoperative radiologic assessment is of paramount importance, and a 2-mm ancillary needlescopic port is somewhat demanded in these patients.
Although it is difficult to adapt to the articulating instruments, we do not believe there exists a steep learning curve for an experienced laparoscopic surgeon with a high volume of conventional RN. As was shown in Table 1, the operative time became shorter with each consecutive case, and it was not much different from standard laparoscopic RN after 9 cases. The postoperative length of stay for patients in both groups was relatively longer because of most patients staying in hospital until they could return to normal activities of life.
In RN, the lengthening of the single incision is always needed, which is, on one hand, a cosmetic compromise and, by itself, increases postoperative pain and the risk of related complications. Only with specimen morcellation can the maximum cosmesis be achieved, however, which will exert an adverse effect on postoperative oncologic assessment. From our viewpoint, the LESS-RN is merely a slight technical modification instead of a surgical revolution. What is more, difficulty in surgical manipulations and cost of surgical instruments greatly increases with possible subtle benefits to be determined compared with conventional laparoscopy.
Ongoing technologic advances specific for LESS, such as the magnetic anchoring and guidance system and in vivo robotics that have been put into clinical practice and purpose-built robotics on the horizon will obviate the technical limitations of LESS. 24 –26 We must take into account, however, patients who are most concerned with cosmesis and at what point does the cosmesis justify the increased expense. A large multicenter prospective comparative study of LESS over conventional RN has been undertaken in our institute to detect the subtle difference between these two approaches.
The da Vinci Surgical System provides the recognized benefits of superior ergonomics, optical magnification of the operative field, enhanced surgeon dexterity, and precision of surgical manipulation. 27 Several innovations have been made to address limitations of the current available robot, which remains bulky and not specifically designed for the LESS technique. 28,29 A reduction in the range of motion of the instruments still exists, however, and the robotic LESS surgery is in its infancy.
Natural orifice translumenal endoscopic surgery (NOTES), an approach without abdominal incision, is gaining momentum. Eight years after the first experience with NOTES (transvaginal nephrectomy in pigs) reported by Gettman and coworkers, 30 the first human pure NOTES in urology—transvaginal nephrectomy—was recently reported by Kaouk and colleagues. 31 Its successful completion with negligible blood loss and absence of perioperative complications made us aware that pure NOTES will be the final solution to the controversy in LESS-RN.
Conclusions
In selected patients, the transumbilical LESS-RN can be performed safely with favorable outcomes. While a learning curve certainly exists, it appears to be short for an experienced laparoscopic surgeon. A long-term follow-up is necessary, and a well-designed prospective comparative study is awaited for solid conclusions.
Footnotes
Acknowledgment
The study has been supported by the Military Major Project for Clinical High-tech and Innovative Technology of China (NO. 2010gxjs057) and the Municipal Hospitals' Project for Emerging and Frontier Technology of Shanghai (NO. SHDC12010115).
Disclosure Statement
No competing financial interests exist.