
Abstract
Purpose:
To describe robot-assisted complex reconstruction of the lower urinary tract in children with neurogenic bladder and sphincteric incompetence.
Patients and Methods:
Four sequential patients with spinal dysraphism, neurogenic bladder, and sphincteric incompetence based on urodynamic parameters had persistent urinary incontinence on maximal anticholinergic therapy and clean intermittent catheterization (CIC). They underwent robot-assisted Mitrofanoff appendicovesicostomy along with Leadbetter/Mitchell bladder neck reconstruction and bladder neck sling. All patients received cystography 3 weeks postoperatively. Patient demographics, medical history, perioperative parameters, and urinary continence status were collected prospectively.
Results:
Mean predicted bladder capacity was 353 mL (range 210–450 mL) while actual preoperative bladder capacity was 216 mL(range 180–275 mL). Preoperatively, one-patient demonstrated uninhibited bladder contractions; none had trabeculated bladders. Mean detrusor leak point pressure was 29 cm H20. Three of four (75%) cases were completed robotically; one necessitated conversion to open and Monti channel creation because of a marginal appendix. Mean operative time (hours:minutes) was 7:45 (range 5:56–12:18). Mean length of stay and blood loss were 85.7 hours and 117.8 mL, respectively. Postoperatively, all patients were completely dry on CIC and anticholinergics. None of the bladders demonstrated trabeculation on follow-up cystography. Unilateral de novo grade II vesicoureteral reflux developed in two patients, and anticholinergics were dose escalated.
Conclusion:
Our initial series of robot-assisted appendicovesicostomy with bladder neck reconstruction and sling placement expands the scope of complex robotic reconstruction in children. The preliminary data demonstrate the procedure to be feasible and safe. Comparison with traditional “open” series of the same procedure is necessary.
Introduction
Increasingly, complex pediatric urologic procedures are being performed with robot assistance. The feasibility of nephrectomy, pyeloplasty, ureteral reimplantation, and bladder surgery has been clearly established. 4,5 A few case reports and a small series have been published describing robot-assisted Mitrofanoff appendicovesicostomy (APV) with or without augmentation ileocystoplasty or creation of an anterograde continent enema colon tube. 6 –9 At our institution, management of neurogenic bladder with persistent urinary incontinence despite clean intermittent catheterization (CIC) and anticholinergic therapy includes creation of a Mitrofanoff APV (or Monti channel when the appendix is inadequate) and Leadbetter/Mitchell bladder neck reconstruction (BNR) along with a bladder neck sling (BNS). 10 We report our initial clinical experience with robot-assisted APV, BNR, and BNS.
Patients and Methods
Patient selection
This is a single surgeon series (PG) of four consecutive patients who received APV/BNR/BNS between April 2010 and August 2010. Institutional Review Board approval was obtained from The University of Texas Southwestern Medical Center and Children's Medical Center to maintain a prospective database regarding clinical outcomes for patients who were undergoing surgery for neurogenic bladder. Informed consent was obtained from patients' parents. All patients received a preoperative urodynamic study (UDS) once they were receiving maximal anticholinergic therapy (the greater of 0.2 mg/kg or 5 mg qid oxybutynin). UDSs were performed under physician supervision as previously described from our institution. 11 Predicted bladder capacity (mL) was estimated by the formula [volume=(age +2)× 30.] Actual bladder capacity was the volume instilled at detrusor pressure less than 40 cm H20. Patients were designated as having sphincteric incontinence and counseled to receive APV with BNR/BNS if they had detrusor leak point pressure (DLPP) <50 cm H20 or a history of stress urinary incontinence despite CIC and maximal anticholinergic therapy or intolerance of anticholinergic treatment without evidence of upper tract deterioration. All patients were preadmitted for a mechanical bowel preparation and preoperative antibiotics.
Description of technique
The patient was placed supine on a surgical bean bag positioner. All potential pressure points were meticulously padded. A 14F catheter was inserted per urethra once the patient was prepped and draped. Pneumoperitoneum was established using a Veress needle in an infraumbilical location. Given the thin nature of the abdominal wall in most pediatric patients, the working ports were secured to the patient's skin with TroGARD® (Conmed Corporation, Utica, NY). Once all ports were secured, the robot (da Vinci Surgical System, Intuitive Surgical, Inc, Sunnyvale, CA) was docked.
On the back table, two 10F subclavian line tunneling devices cut to 2.5 cm were attached with 3-0 polydioxanone (PDS) suture to a 10 cm entimeter×1 cm strip of Tutoplast cadaveric fascia (IOP, Inc, Costa Mesa, CA), which would serve to create the sling.
An inverted V-shaped incision was made at the umbilicus, ultimately serving as the future skin flap to bring to the APV, and the 12-mm robotic camera was placed after Veress needle insufflation. Under direct visualization, two 8-mm robotic ports were placed: The first in the right midclavicular line slightly superior to the camera port and the second in the left midclavicular line just inferior to the umbilical site. A 12-mm assist port was placed between the left arm and the working camera port (Fig. 1). A 12-mm trocar was used to accommodate suture needles and Lapra-Ty (Ethicon, Inc. San Angelo, TX).
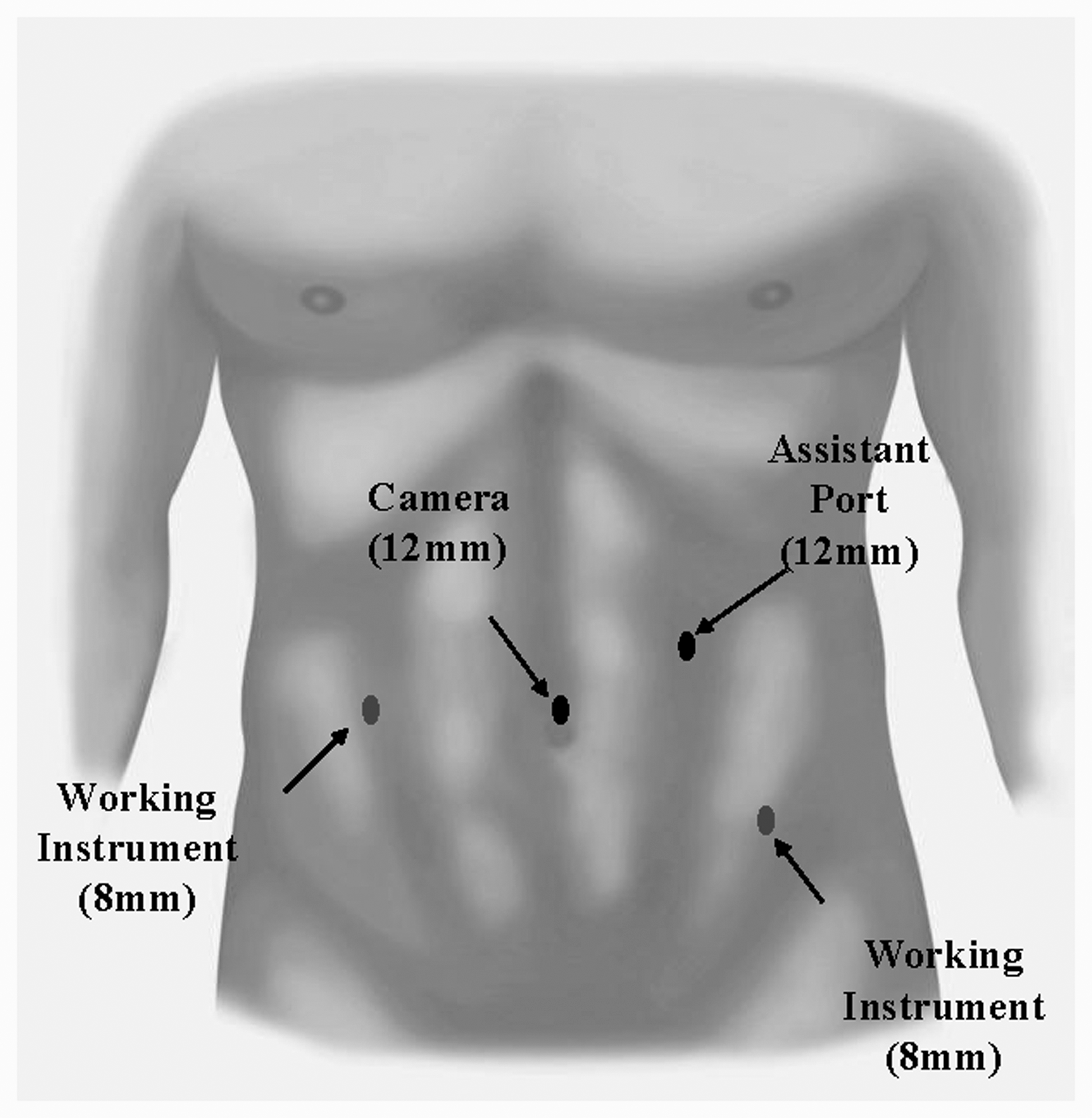
Port placement.
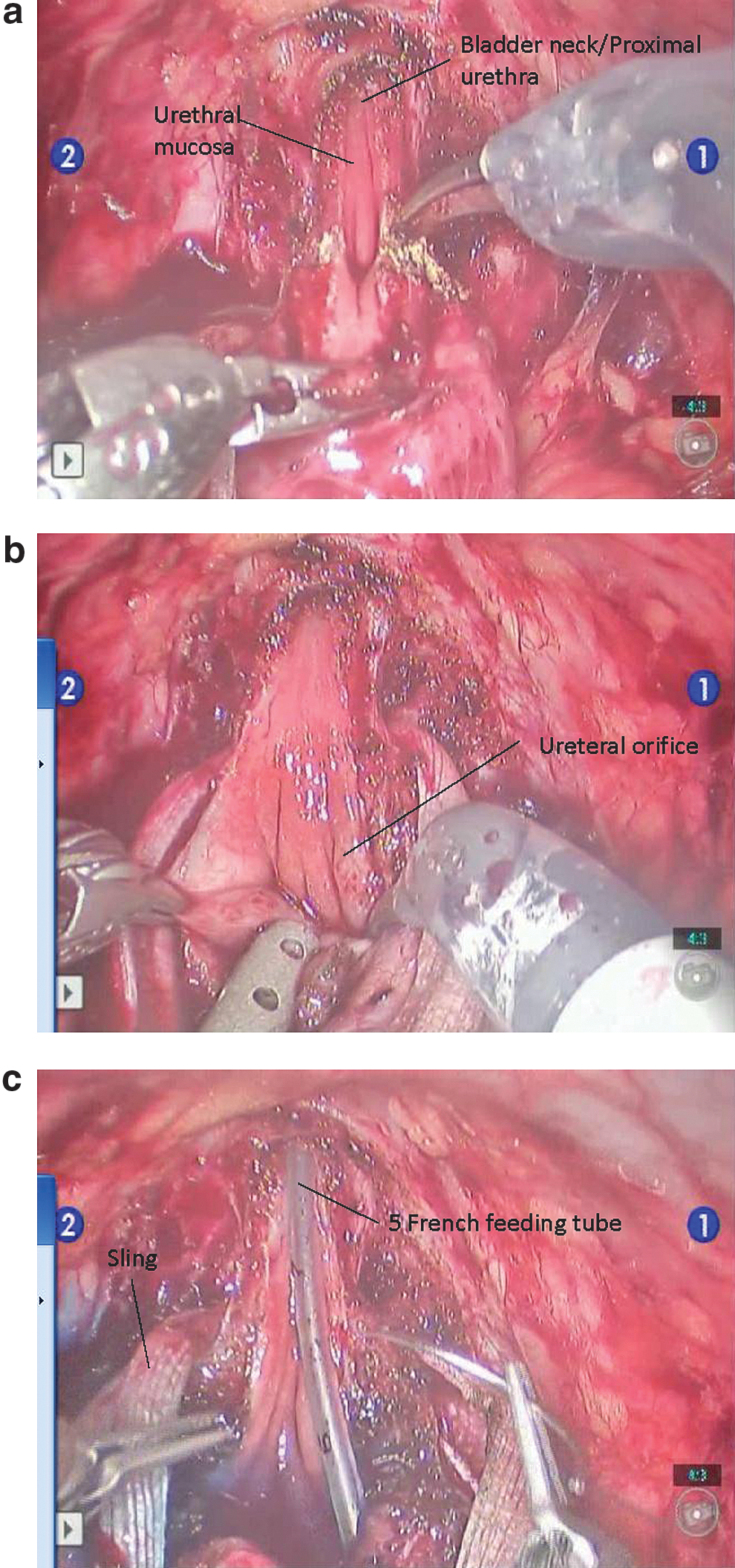
After the robot was docked, a crescent-shaped incision was made posterior to the bladder to drop the rectum in males or vagina in females. The plane for placement of the sling was developed specifically for robotic surgery with limited tactile feedback. Specifically, the peritoneum was incised and the space of Retzius was developed in both males and females. On the posterior aspect, the rectovesical space (boys) and the vesicoureterine space (girls) was developed, from which point the tunnelers were passed ventrally into the developed space of Retzius (Figs. 2a, 2b, 2c). The bladder was dropped anteriorly, and the suspensory puboprostatic ligaments were divided using monopolar cautery. A 2.0 polyglactin dorsal vein stitch was placed before cutting down to the catheter and unroofing the proximal urethra and bladder neck to the level of the interureteric ridge (Fig. 3a). The ureteral orifices were identified by having the anesthesiologist inject 5 mL of indigo carmine into the patient's intravenous line (Fig. 3b). At this point, the Foley catheter was exchanged for a 5F feeding tube, and the urethra was retubularized in two layers with a running simple suture of 5-0 PDS followed by 4-0 PDS (Fig. 3c).

Given the patients' ages and their underlying pathology (spinal dysraphism), we found it important to preserve bladder capacity in these young patients with neurogenic bladders. As such, although we could not uniformly excise a 3 to 4 cm strip of bladder, we did go to the level of the intraureteric ridge in all patients. While the ureters could be reimplanted robotically to remove a larger bladder segment, we did not find this maneuver to be necessary. Bladder integrity was ascertained by injecting the bladder with saline. After the Leadbetter/Mitchell BNR, the tunneling devices were identified by dissecting lateral to the urethra. The sling was tightly wrapped 360 degrees and attached to the pubic bone using six screws from a hernia tacker (Fig. 4).
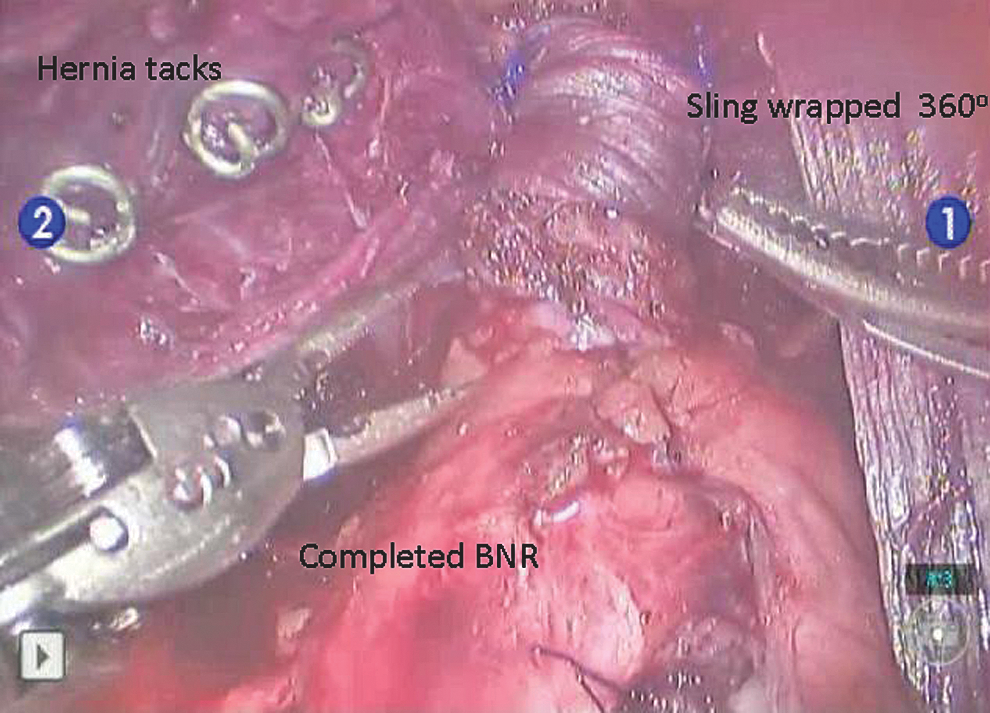
Fascial sling is wrapped 360 degrees and tacked to pubic bone.
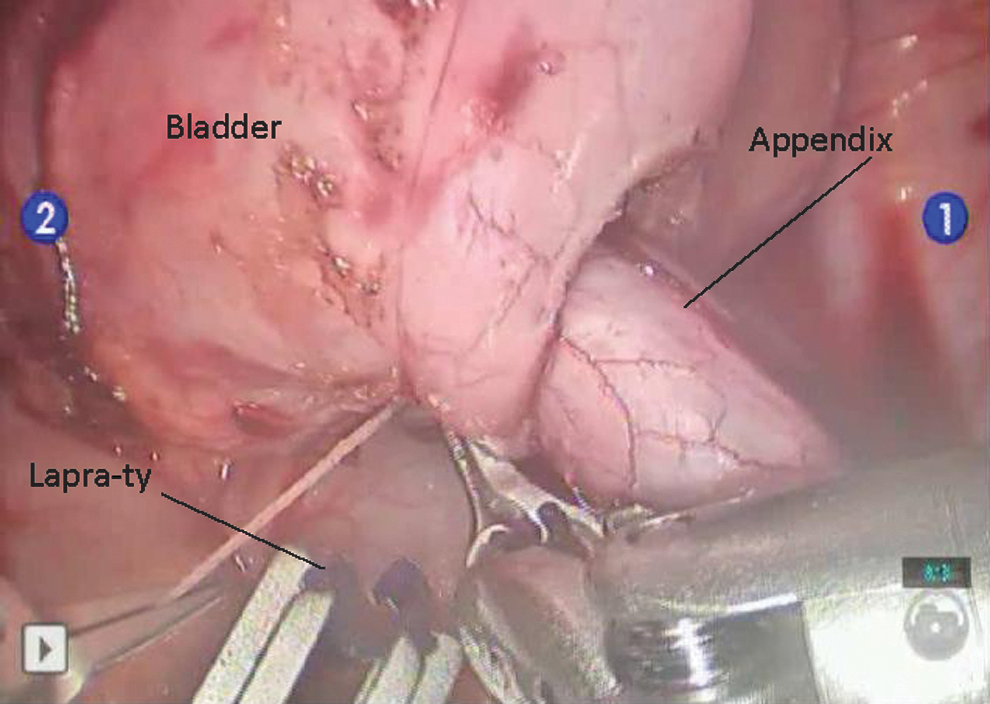
Attention was then directed toward creation of the APV. The bladder was hitched to the anterior abdominal wall with 2-0 PDS to provide a tension-free APV. With careful preservation of the mesoappendix, the appendix was harvested from its stump. The cecotomy was closed with a zero chromic tie, which was subsequently inverted with a 3-0 silk purse-string suture. The liberated appendix was intubated with a 10-cm, 10F feeding tube that was secured to the proximal appendix with a 2-0 PDS suture, and the distal 0.5 cm was removed. Detrusorrhaphy using monopolar electrocautery was performed to create a 3 to 5 cm tunnel. All detrusor tunnels were created on the posterior bladder wall. Before incision of the mucosa at the distal end of the tunnel, a 5-0 polyglactin suture was placed at the apex to prevent mucosal retraction; the anastomosis was completed with interrupted 5-0 polyglactin suture (Fig. 5). The appendix was placed within the detrusor trough, and the tunnel was closed with figure-of-eight sutures of 3-0 polyglactin cut at 10 cm and secured with Lapra-Ty (Fig. 6).
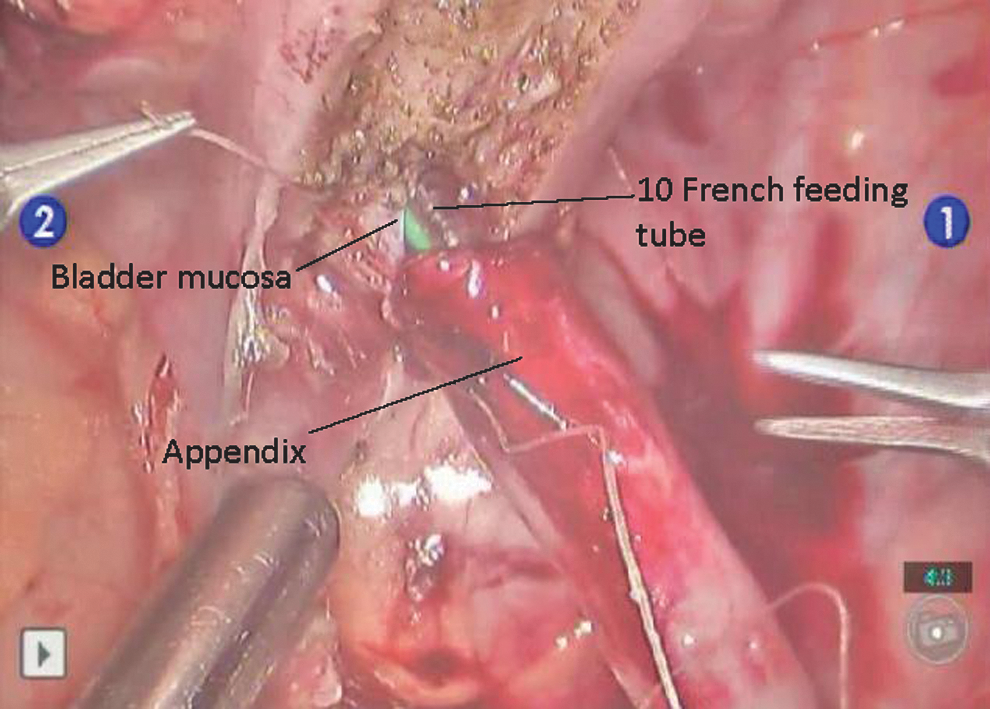
Securing appendix to bladder mucosa.
Closure of detrusor tunnel.
The proximal end of the appendix was delivered through the umbilical incision under direct visualization. The appendix was then matured into the umbilicus as previously described. 8 Briefly, the appendix was spatulated and then secured to the fascia followed by the skin. The feeding tube was exchanged for a 14F Mentor catheter that was secured to the skin. The urethral 5F feeding tube was secured to the foreskin or labia. Seventy-five percent of the actual bladder capacity was instilled into the bladder to ensure integrity. All patients were discharged on anticholinergic therapy unless intolerant and underwent cystography 3 weeks postoperatively.
Outcomes
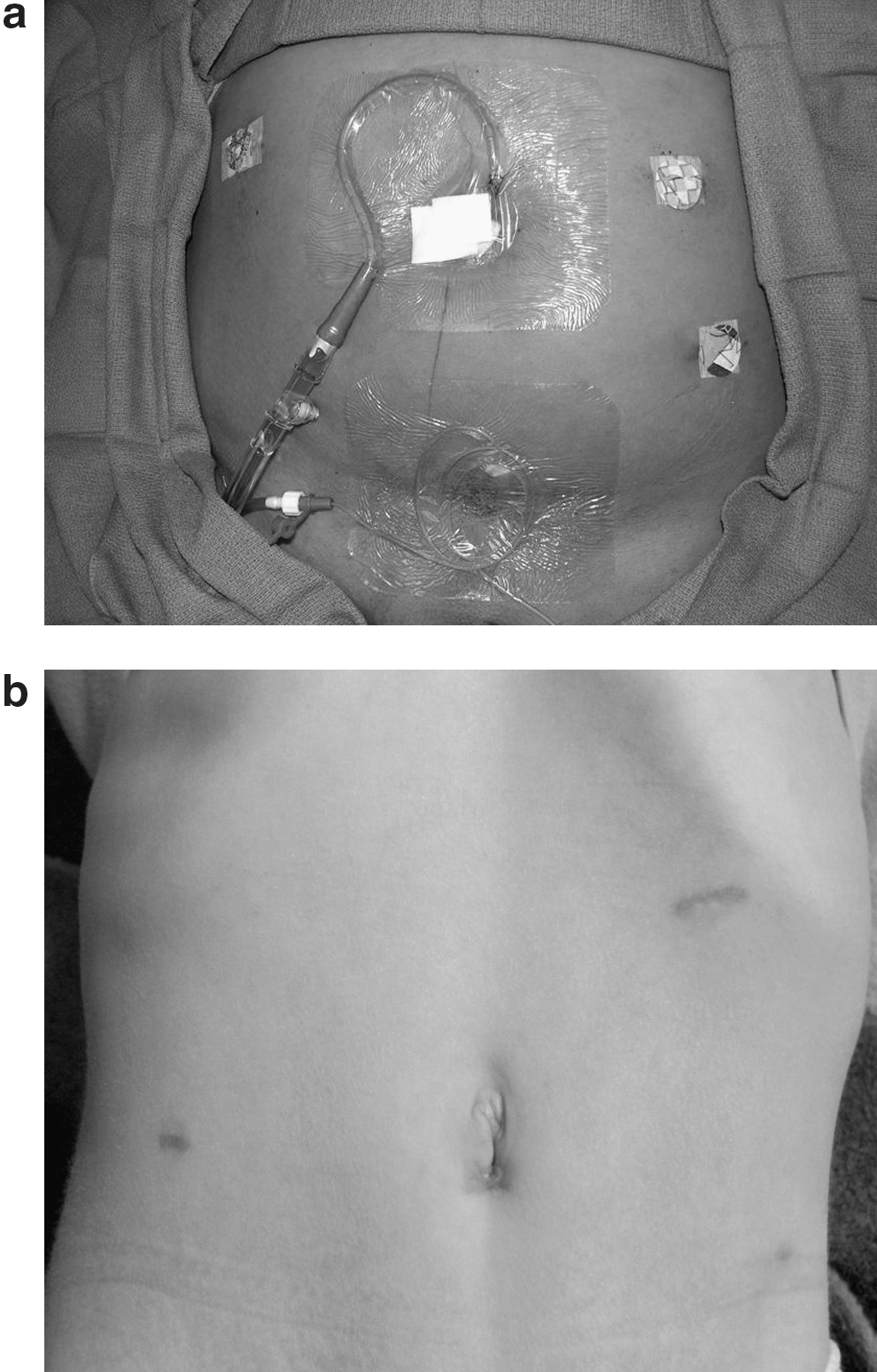
Demographic information, type of spinal dysraphism, medications, and preinterventional urodynamic parameters on maximal therapy were accessioned before surgery (Table 1). Perioperative data included total and categorized operative times, length of stay (LOS), estimated blood loss (EBL), the occurrence of complications, and procedure success, defined as an easily catheterizable APV and complete dryness (Table 2). Representative immediate and 6-week follow-up results are demonstrated in Figures 7a and 7b.
BMI=body mass index; shunt=ventriculoperitoneal shunt; BC=bladder capacity; UIC=uninhibited contractions; DLPP=detrusor leak point pressure.
EBL=estimated blood loss; LOS=length of stay; VUR=vesicoureteral reflux.
Results
Results are summarized in Tables 1 and 2. Underlying pathology was myelomeningocele in three patients and lipomeningocele in one. Three patients were female. Mean age was 9.8 years (range 5–13 y) and mean body mass index was 24.3 kg/m2 (range 16.7–29 kg/m2). Mean predicted bladder capacity was 353 mL (range 210–450 mL) while actual preoperative bladder capacity was 216 mL (range 180–275) mL. Before surgery, one patient demonstrated one uninhibited bladder contraction during cystometrography. No patients had trabeculated bladders or preoperative reflux. Three patients had DLPP less than 50 cm H20. One patient had DLPP of 53 cm H20 with no evidence of reflux or upper tract damage, including normal renal ultrasonography and serum creatinine level.
Three of four (75%) of the cases were completed successfully. One patient (case 2) needed conversion to an open procedure. The patient needing conversion had very severe scarring from multiple ventriculoperitoneal shunt revisions and her appendix was retrocecal, necessitating extensive dissection to liberate the appendix. In this patient, after the appendicovesical anastomosis was completed and the detrusorrhaphy closed, the appendix was noted to be dusky, although the mesentery appeared to be intact. The appendix was matured to the skin, but a catheter would not pass easily. The APV was taken down, and we converted to the open creation of a Monti conduit. Mean operative time (hours:minutes) was 7:45 (range 5:56–12:18); excluding the case necessitating conversion, mean was 6:14.
Subdivided times are listed in Table 2. Mean LOS was 85.7 hours, or 44.8 hours if case 2 were excluded. Similarly, EBL was 117.8 mL vs 40.3 mL. The patient needing conversion to an open procedure remained intubated and was admitted to the intensive care unit for resuscitation, given low urine output and blood pressure. She responded well to fluids and aggressive pulmonary toilet. She also had breakthrough seizures, a postoperative ileus, and a urinary tract infection. No complications were observed in the other three patients.
Postoperatively, none of the patients were leaking urethrally or from their conduit. None of the bladders demonstrated trabeculation on follow-up cystography. Asymptomatic unilateral de novo grade II vesicoureteral reflux developed in two patients, and were dose escalated on anticholinergics.
Discussion
Paul Mitrofanoff's APV procedure, first described in 1980, is an integral component of the treatment of patients with neurogenic bladder when urethral catheterization is no longer possible. 12,13 Incontinence rates are low (<5%), and postoperative complications—including stomal stenosis (10%), cystolithiasis, urinary tract infection, wound dehiscence, bowel obstruction, and development of peristomal hernia are also infrequent after APV. 12,14 Given the variability and spectrum of bladder structure, function, and compliance (small capacity, hyperreflexic to myogenic failure/acontractile with increased capacity) and also in bladder neck/external sphincter physiology (hypertonic to extremely low detrusor and stress leak point pressures), patients may need bladder neck procedures to obtain urinary continence. 15,16
Options include injection of bulking agents around the bladder neck, placement of artificial urinary sphincter (AUS), BNR, and fascial sling procedures. 17 At our institution, bladder neck surgery is performed for DLPP <50 cm H20 or a history of stress urinary incontinence despite CIC and maximal anticholinergic therapy.
Several studies from the 1980s called to attention deleterious effects of increasing bladder outlet resistance in patients with neurogenic bladder, suggesting that the increased resistance leads to detrusor hyperreflexia and decreased compliance. In turn, elevated detrusor pressures were implicated in causing hydronephrosis, vesicoureteral reflux, renal damage, and incontinence. 18 –20 These initial reports of upper tract damage after bladder outlet procedures were in patients who received AUS.
Slings, however, may not occlude the bladder neck as completely as AUS, alleviating the high intravesical pressures. Consequently, augmentation cystoplasty is commonly performed at the time time of bladder neck procedures. 21,22 For instance, Perez and colleagues 23 performed augmentation cystoplasty in 87% of their sling procedures. Augmentation cystoplasty is not without potential complications, including rupture, malignancy, and infectious complications ranging from 20% to5 0%. 22,24 Snodgrass and associates 11 reported successful outcomes in patients receiving BNS and APV without augmentation, with only 1/30 (3.3%) patients ultimately needing enteroplasty for symptomatic hyperreflexia and compliance loss. Further, the same authors demonstrated that at a mean of 39 months, urodynamic patterns remained stable or improved in comparison with preoperative UDSs for patients receiving sling/APV without augmentation. No new cases of hydronephrosis, bladder trabeculation, or reflux were identified in that cohort. 25
In efforts to enhance continence rates, Snodgrass and coworkers 10 began performing Leadbetter/Mitchell bladder neck procedure in addition to fascial sling. The cohort receiving BNR plus sling had a 94% complete continence rate compared with 46% who underwent sling alone. Preservation of the upper tracts is likely in part because the bladder outlet controlled only with a sling allows for a pop-off mechanism in the event of high intravesical pressures.
We report our experience with robotic APV with Leadbetter/Mitchell BNR followed by fascial sling. To our knowledge, this is the first robotic series of extensive BNR and sling placement in addition to APV. Similar to Nguyen and colleagues, 8 conversion to open surgery was necessary for a marginal appendix in one case. Excluding the case that was converted, our mean operative time of 6 hours is comparable to those reported for APV with or without augment or creation of anterograde continent enema. 6 –8 The patient who needed open conversion had numerous risk factors that made her surgery and postoperative course substantially more complex, including a ventriculoperitoneal shunt with dense adhesions, a retrocecal appendix, and an American Society of Anesthesiologist score of 3. The patient who needed conversion to an open procedure had a history of a ventriculoperitoneal shunt necessitating two previous revisions. The resultant inflammation and subsequent fibrosis made the dissection substantially more difficult and may be a reason to preclude this type of advanced robot-assisted surgery.
Several technical modifications were made over the course of this series that facilitated successful surgery. Using a dorsal venous suture before bladder neck reduction significantly increased visibility. Second, we found that once one subclavian dilator was identified in the space of Retzius, it was often easier to pass the same dilator from anterior to posterior on the contralateral side for sling creation. All detrusor tunnels were created on the posterior bladder wall because decreased stone formation, urinary tract infection, and increased mucus removal are cited with posterior placement. 26 Maneuvers for improving the operation will surely continue to come to light.
The benefits of robot-assisted surgery were evident in the majority of our patients. Three of four patients were discharged on postoperative day 2. Unilateral low-grade reflux did develop in two patients; it has responded to increased anticholinergic dose. The patients in whom de novo reflux developed will be followed by semiannual creatinine check, renal ultrasonography, and dimercaptosuccinic acid scan. As long as no parameters worsen, the interval for evaluation will be extended. The patient with the protracted hospital course is doing well and back to her preoperative baseline. All four are completely dry and able to catheterize their APV easily. In addition to potential for decreased postoperative pain, rapid convalescence, and improved cosmesis, RALS surgery has immense potential with respect to meticulous dissection when operating in the deep pelvis in children—one of the main reasons this technology has taken a strong foothold in urologic and gynecologic surgery.
Conclusion
Our initial series of robotic APV with BNR and sling placement expands the scope of robot-assisted surgery in children. Although the length of follow-up is a limitation, the preliminary data demonstrate the procedure to be feasible and safe. Comparison with open APV with BNR is needed as is a cost analysis.
Footnotes
Disclosure Statement
No competing financial interests exist.