
Abstract
Purpose:
To investigate the clinical effect of minimally invasive percutaneous nephrolithotomy (MPCNL) using a patented irrigation and clearance system.
Patients and Methods:
From August 2008 to August 2009, 60 patients with renal stones ≥2.0 cm were randomly assigned to two groups. Group 1 included 30 patients who were treated by MPCNL through a patented 16F sheath with the aid of a patented irrigation and clearance system combined with a high power holmium laser. Group 2 included 30 patients who were treated by a third generation EMS ultrasound/ballistic trajectory lithotripsy and clearance system through a standard 24F sheath. The differences in (1) average time needed for stone clearance; (2) percentage of cases in which one surgery resulted in freedom from stones; (3) mean renal pelvic pressure; and (4) mean amount of intraoperative bleeding were compared.
Results:
Compared with the EMS ballistic trajectory/ultrasound lithotripsy and clearance system, the MPCNL irrigation and clearance system had a significantly higher percentage of stone-free outcomes after one surgery and a lower amount of introperative bleeding (P<0.05). There was no difference in mean stone-clearance time and mean renal pelvic pressure (P>0.05). When comparing the cases with one percutaneous tract in the patented system group with the cases with one percutaneous tract in the EMS system group, the findings were similar.
Conclusion:
The patented MPCNL irrigation and clearance system is safe and highly efficient in managing renal stones.
Introduction
Since some scholars first proposed a Chinese minimally invasive percutaneous nephrolithotomy (MPCNL) to remove stones, 3 –8 Chinese MPCNL has gradually been accepted by many patients and urologists in China as a significant improvement over standard PCNL and has become one of the most important ways to manage urinary tract stones in China. 3 –8
More than one kind of sheath has been used in MPCNL, and the peel-away sheath is the best known. Application of MPCNL using a peel-away sheath is an effective way to manage upper urinary tract calculi. The tract is small, less traumatic, and combined with the high-power holmium laser (or ballistic trajectory), has the advantages of breaking stones more effectively and producing less bleeding. 3 –8 This technique clears stones away mainly through high-pressure perfusion or the use of pliers to remove stones manually. This procedure, however, can lead to fever from high pressure-induced bacterial endotoxin absorbance in the renal pelvis. 6 If hydronephrosis is pronounced, high-pressure perfusion makes it difficult to remove the rubble completely, because it moves around inside the renal pelvis; in addition, a considerable amount of fluid can be absorbed by the body, resulting in “water-absorption syndrome,” or in pleural or peritoneal effusions. 9
The major disadvantage of a typical Chinese MPCNL is that it lengthens the duration of the surgery. 9,10
Recently, EMS Company from Switzerland introduced a third-generation ultrasonic pneumatic lithotripsy stone clearance system, with the function of breaking and aspirating stones. This can remove stones immediately after they are broken, reduce or avoid the use of high-pressure water or pliers to take out debris and rubble, and shorten operative time. PCNL dilation to 24F or 30F, however, may have increased risk of renal parenchyma artery vascular injury, 3,5,10 –12 and it is more difficult for a larger endoscope to enter the narrow calices. 4,5,10 Larger devices are also hard to use in a small space, such as when removing pediatric kidney stones or multiple dispersed kidney stones. 4,5,10 Frequently, multiple working tracts are needed.
One of the main causes of residual stones after PCNL is that the endoscope cannot enter the calices where stones reside. 4,5,13 For multiple, staghorn calculi, PCNL using the EMS system through the standard percutaneous tract has a lower rate of one-time stone clearance. 5
We designed a patented lithotripsy and suctioning/clearance system to solve the problems mentioned above. From August 2008 to August 2009, we treated 30 patients with renal stones by using Chinese MPCNL through a patented 16F sheath (hereafter referred to as the patented system), and treated another 30 patients with renal stones by using a third-generation EMS ultrasound/ballistic trajectory lithotripsy and clearance system through a standard 24F sheath (hereafter referred to as the EMS system). We compared the results for these two groups, and the outcome is reported.
Patients and Methods
Clinical data
There were 60 patients with renal stones—38 men, 22 women. Ages ranged from 23 to 66 years with a mean age of 42. There were five cases of renal stones that were complicated by pyonephrosis. In nine cases, shockwave lithotripsy (SWL) treatment had failed. In 12 cases, there was a history of stone removal by open surgery. These 60 patients were randomly divided into two groups who were treated with the patented system and the EMS system, respectively. Stone size was ≥2.0 cm. The stone burden (cm2) was measured by multiplying the length and the width of the stone in the kidneys, ureters, and bladder. The average stone burden in the patented system group was 8.57±2.25 cm2 (2.25 ∼ 31.7 cm2), and the average stone burden in the EMS system group was 8.65±2.03 cm2 (2.20 ∼ 32.1 cm2). There was no statistical difference in stone burden between the two groups (P=0.44).
Patients and Methods
Surgery took place under continued epidural anesthesia or general anesthesia. The patient was first placed in a lithotomy position. A 5F ureteral catheter (Shanghai Medical University Kangge Medical Instrument Co, Ltd, Shanghai, China) was then inserted retrogradely into the renal pelvis through cystoscopy or ureteroscopy, and continuous infusion of saline was used to produce artificial hydronephrosis. After this, a Foley catheter was inserted; the patient was then changed to the prone position. The abdomen was not boosted in the patented system group.
Ultrasonography-guided percutaneous punctures were made with an 18-gauge coaxial needle (Create Medic Co, Ltd, Dalian, China) into the targeted calix (middle/lower kidney calices). The puncture point was in the 11th intercostal space or the 12th subcostal margin, between the posterior axillary line and scapula line. The puncture was judged successful if there was urine overflow or if it touched a stone. Zebra guidewire (Create Medic Co, Ltd, Dalian, China) was inserted and fixed. The puncture needle was then taken out. After a 0.5–0.7 cm skin incision, the dilation of the percutaneous tract was performed serially over the guidewire with a fascial dilator (Create Medic Co, Ltd, Dalian, China) to 16F.
A 16F patented sheath (Fig. 1) was placed at the percutaneous access port and was connected to a vacuum aspiration machine. Intraoperatively, irrigation volume was set at 600∼800 mL/min, irrigation pressure was set at 250∼300 mm Hg, suction pressure was set at 100∼250 mm Hg. Subsequently, a small diameter nephroscope (Lixun Nephroscope, Richard Wolf, Knittlingen, Germany) was inserted through the sheath to observe stones. A holmium laser (3.5∼4.0J×15 HZ) was used to break the stones, and a vacuum suctioning device was used to clear gravel.

Lithotripsy with the aid of a vacuum device.
For patients in the EMS system group, dilation of the percutaneous tract was performed serially over the guidewire with a fascial dilator (Create Medic Co, Ltd, Dalian, China) to 16F. Then a telescopic dilator was used to dilate to 22F. A 24F sheath was placed as the percutaneous access port and was connected to a vacuum aspiration machine. Subsequently, a 24F standard nephroscope was inserted through the sheath to observe stones. An EMS system ultrasound or ballistic trajectory combined with ultrasound was used to break the stones, and a vacuum suctioning device was used to clear gravel. After all stones were removed, zebra guidewire was inserted into the ureter. At the end of the surgery, a 5F Double-J stent (Freda Medical Instrument Co, Ltd, Shandong, China) was inserted in the ureter under guidance of the ureteral catheter, and a nephrostomy tube of the same caliber (16F) was left in place.
Intraoperatively, the outside end of the 5F ureteral catheter that had been previously inserted was connected to an invasive blood pressure monitor and fixed at the level of the renal pelvis. For each patient, the manometry system was set at zero, the renal pelvis pressure measured, and any changes recorded. Stone clearance time was recorded (from the beginning of stone clearance to the end of the nephrostomy tube indwelling). Routine blood tests were repeated immediately after surgery. The amount of intraoperative bleeding was calculated using a hydrogenated high iron hemoglobin method to measure the hemoglobin concentration in the suctioned fluid by the following formula: Volume of blood loss (mL)=[hemoglobin concentration in the suctioned fluid sample (g/L)×total volume of suctioned fluid (mL)]/preoperative hemoglobin concentration (g/L). 14
Abdominal plain radiography was performed 3 to 5 days after surgery, and a CT was performed for cases with uric acid stones, to check for residual stones. If no residual stones >4 mm were present, the nephrostomy tube was removed, and no further treatment was pursued. Otherwise, a second-stage PCNL or SWL treatment was performed. Specifically, we gave SWL first consideration if there was only a single residual stone <2 cm. We used second-stage PCNL for cases with large residual stone >2 cm or multiple residual stones or those cases for which there were contraindications to the use of SWL. Stone clearance time, renal pelvis pressure, presence or absence of residual stones, number of percutaneous tracts used, mean amount of bleeding, and presence or absence of postoperative fever were recorded as data.
Statistics
All data were analyzed using SPSS11.5. A Student t test was used for quantitative variables, and a chi-square test was used for qualitative variables. P<0.05 was used to indicate statistical significance.
Results
In all 30 patients who underwent MPCNL with the aid of the patented irrigation clearance system, percutaneous renal access for stone removal was successfully established. Among these, 28 cases were treated using a single percutaneous tract, 2 cases using two tracts. The average stone clearance time was 39±10 minutes. In 27 cases, stones were removed completely in one operation. One surgery stone-free rate was 90%. Two patients needed two PCNLs to remove stones completely. One patient needed SWL after the surgery. The average renal pelvic pressure was 4.1±1.8 mm Hg. The average amount of bleeding was 90±33.1 mL. A nephrostomy tube was indwelling in all cases. No organ damage or pleural or peritoneal effusions occurred. Three days after surgery, body temperature was ≥38.5°C in three cases.
The other 30 patients with renal stones were treated with PCNL with the aid of the EMS system after establishing a standard percutaneous tract. Among these, 19 cases were treated using a single percutaneous tract, 9 cases using two tracts, and 2 cases using three tracts. The average stone clearance time was 42±8 minutes. In 22 cases, stones were removed completely in one operation. One surgery stone-free rate was 73.3%. Five patients needed PCNLs to remove stones completely. Three patients needed SWL after the surgery. The average renal pelvic pressure was 4.5±1.6 mm Hg. The average amount of bleeding was 110.9±35.2 mL. A nephrostomy tube was indwelling in all cases. No organ damage or pleural or peritoneal effusions occurred. Three days after surgery, body temperature was ≥38.5°C in four cases.
Compared with the EMS ultrasound/ballistic trajectory lithotripsy and clearance system, the patented irrigation and clearance system had a significantly higher percentage of stone-free outcomes after one surgery (P<0.05) and a lower amount of intraoperative bleeding (P<0.05). There was no difference in mean stone-clearance time and mean renal pelvic pressure (P>0.05). There was a significantly higher percentage of cases in which only one percutaneous tract was needed for stone removal (93.3% vs 63.3%, P<0.05) (Table 1).
SWL=shockwave lithotripsy; PCNL=percutaneous nephrolithotomy.
When comparing the cases with one percutaneous tract in the patented system group with the cases with one percutaneous tract in the EMS system group, the findings were similar. There was no significant difference in stone clearance time (38.6 min vs 40.1 min). There was a significantly higher stone clearance rate (89.29% vs 57.89%) in the patented system group (P<0.05). There was also significantly less intraoperative bleeding (83.30 mL vs 96.74 mL) in the patented system group (P<0.05) (Table 2).
Discussion
Our patented lithotripsy and suctioning/clearance system comprises a patented sheath, a small diameter (12F) nephroscope, and an irrigation and suctioning system (Fig. 2). The material of this sheath is hard and not easily deformed, maximizing access. The distal portion of the sheath leads into a funnel-shaped internal cavity. This prevents rubble from blocking the aspiration passage.
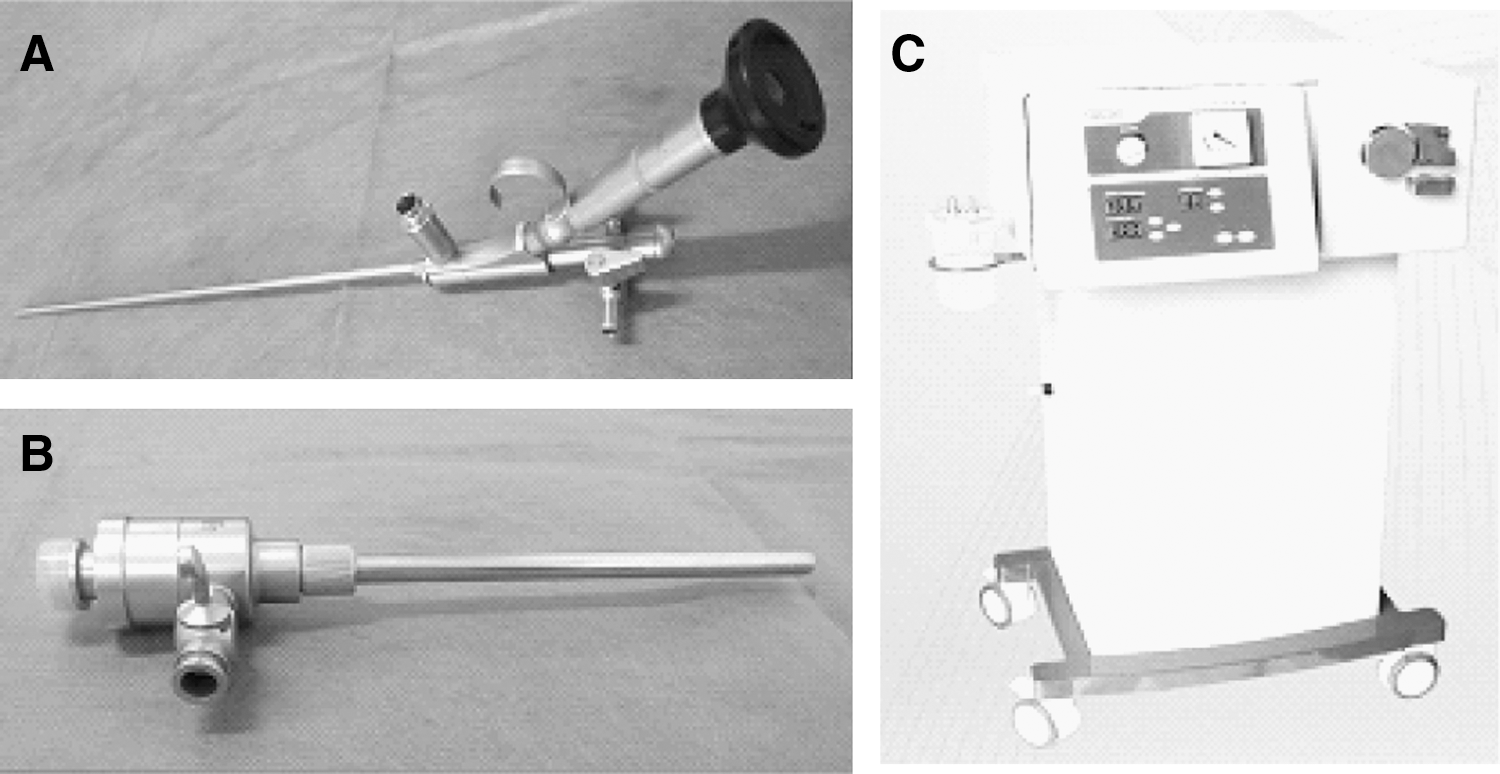
Lithotripsy and suctioning/clearance system.
One side of the cavity is connected to a vacuum aspiration tube with a diameter larger than the diameter of the lumen of the sheath, which allows the rubble to be aspirated out. The funnel-shaped cavity with its movable sealing lid allows the renoscope to move in and out conveniently while preventing extremely high or low pressure. When it is continuously infused with saline during the operation, vacuum aspiration is regulated to keep the collecting system in a state of negative pressure. This means that the breaking and suctioning of stones can go on at the same time. The side gate valve is adjusted to keep a low positive pressure state inside the collecting system, allowing the sheath and scopes to explore every group of calixes. The lateral hole in the anterior part of the sheath makes the visual field clearer during suctioning (Fig. 3).
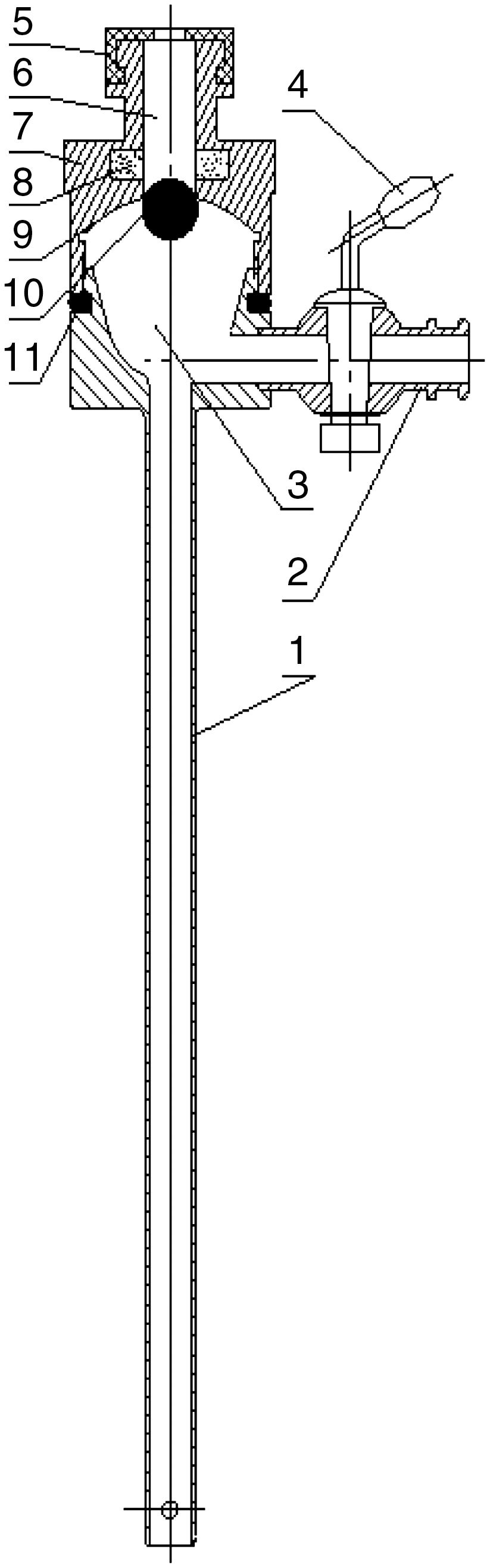
Parts of the patented sheath. (1) Metal sheath; (2) side suction tube; (3) funnel-shaped internal cavity; (4) valve of side suction tube; (5) sealed cap; (6) sealed working passage; (7) sealed lid; (8) permanent magnetic ring: (9) hemisphere surface; (10) magnetic steel ball; (11) sealing soft ring.
This study indicated that the patented system group had a significantly higher percentage of stone-free outcomes after one surgery and significantly less intraoperative bleeding compared with the EMS system group. When comparing the cases with one percutaneous tract in the patented system group with the cases with one percutaneous tract in the EMS system group, the findings were similar.
Intraoperative bleeding will significantly increase with more percutaneous tracts, larger tract diameter, and longer operative time. 10,15,16 Our findings regarding use of suction-assisted MPCNL and the small diameter patented sheath in 30 cases of patients with upper urinary tract calculi suggest that this method has significantly less need for blood transfusion compared with PCNL using the standard percutaneous tract. The skin-kidney tract is only extended to 16F, reducing the risk of renal cortex avulsion and intraoperative bleeding, speeding up the rate at which stones can be actively removed, and minimizing surgical injury. Because the rigid structure applies pressure to the tissues of the percutaneous tract, this helps reduce bleeding. In contrast, if the diameter of the percutaneous tract is bigger, there is a more frequent need for multiple tracts. There was significantly lower intraoperative bleeding compared with the EMS group.
The rigid design of the sheath ensures that the percutaneous tract is not deformed and is maximized so that stones can be sucked out once they are broken into several large pieces; stones rarely block the suction system, and the efficiency of stone removal is improved. The simultaneous application of high-power holmium laser lithotripsy allows stones to be quickly crumbled into powder, with the resulting diameter of debris generally <5 mm. 17 This makes it possible to avoid both the manual use of pliers to take out stones and high-pressure irrigation, shortens the operative time, and improves operation efficiency. Stones <2 mm in diameter were aspirated directly through the sheath. Those between 2 mm and 5 mm were aspirated out after the scope was withdrawn to the funnel-shaped portion of the sheath under the surveillance of the monitor. To make the surgical field clearer, we used high-volume irrigation to decrease the powdered gravel sedimentation caused by high powered holmium lithotripsy. The irrigation also helped to avoid heat injury from the holmium lithotripsy. Using the minimally invasive percutaneous tract with the patented system has a stone-clearance time similar to that of the EMS system using a standard percutaneous tract, and has a significantly higher stone-clearance rate.
For each surgery in the patented system group, we did not booster the abdomen to immobilize the kidney. The increased ability of the kidney and ureter to move facilitates the hard sheath's access to all target locations, making it easier to break all stones. Because the patented sheath is small and its range of movement is increased, it can easily access most of the renal calices and the upper ureter to explore and remove stones under direct vision, reducing the number of percutanous tracts needed for multiple or staghorn kidney stones, thereby reducing kidney damage (Figs. 1, 4).

Single-channel litholipsy with preoperative and postoperative radiography of the kidneys, ureters, and bladder.
Intraoperative infusion can lead to washing solution extravasations 18 and fever from high pressure-induced bacterial endotoxin absorbance in the renal pelvis. 19,20 Switches in the patented sheath allow the pressure in the collecting system to be either positive or negative as needed. Our study indicated that there was negative pressure in the renal pelvis in both the patented system group and the EMS system group. Thus, kidney reperfusion injury, extravasations of perinephric fluid, pleural effusion, peritoneal effusion, water and electrolyte imbalance, heart failure, and surrounding organ infection are avoided that are caused by continuous irrigation with water from an infusion pump. The bacteremia and toxemia can be avoided that result when high intraoperative renal pelvis perfusion pressure causes bacteria or toxins to enter the bloodstream. This increases the safety of surgery in cases of urinary stones complicated with infection or infective stones.
Using the approach reported in this article, there were no cases of pleural effusion or peritoneal infusion. In turn, the proportion of cases with postoperative fever was significantly lower than when other approaches were used. 21 Indeed, we performed MPCNL surgeries in five cases of kidney stones that were complicated with obstruction and empyema, with good results, and without sepsis, thus broadening the MPCNL surgical indications.
Conclusion
This study showed that application of the patented system to MPCNL is a new, safe, simple, more efficient MPCNL that does a better job of removing stones and reduces surgical and postoperative complications, even though some of the differences between the two groups are likely related to differences in the operating technique (MPCNL vs standard PCNL) and have less to do with the intracorporeal lithotripsy device chosen. Given that the necessary investment in equipment is small and its clinical application easy to implement, this represents an important clinical advance.
Footnotes
Acknowledgment
This work was supported by major scientific and technological project funds of Jiangxi Provincial Health Department, Jiangxi, China (20094015) to L.M.S.
Disclosure Statement
No competing financial interests exist.