
Abstract
Purpose:
To evaluate the outcomes of robot-assisted radical prostatectomy (RARP) in patients with previous renal transplantation.
Patients and Methods:
We retrospectively identified all patients who had undergone RARP for localized prostate cancer between 2005 and 2008 at a single institution (N=228). Of these, three patients were renal transplant recipients. A four-arm robotic configuration was used in all patients. Port placement was modified in two of the three renal transplant recipients to avoid trauma to the renal allograft. Preoperative demographics, perioperative parameters, and postoperative outcomes were reviewed.
Results:
RARP was completed successfully in all three renal transplant recipients. As expected, the American Society of Anesthesiologists score (3.3 vs 2.4) and Charlson weighted index of comorbidity (4.7 vs 2.4) were greater in previous transplant patients. There were no major differences in mean age, Gleason score, body mass index, estimated blood loss, operative time, complications, or oncologic outcomes between the two groups. Each of the patients with renal allografts had an undetectable prostate-specific antigen level and was continent (needing no pads) at 13 months of follow-up.
Conclusions:
RARP is feasible in patients with a previous renal transplant. Although technically more challenging, RARP can be performed in previous transplant patients with acceptable morbidity and oncologic outcomes similar to those of other prostate cancer patients.
Introduction
Thomas and associates 3 reported a series of three laparoscopic radical prostatectomies (LRP) in patients who had received a previous renal allograft. 3 There are limited data in the literature, however, regarding the use of robot-assisted radical prostatectomy (RARP) in a renal transplant recipient. While Jhaveri and colleagues 4 reported a single case of RARP in a renal transplant recipient, 4 there has been no previous study reporting a series of patients undergoing RARP after transplant. Similarly, there has been no study comparing the outcomes of RARP in previous transplant patients against a control group of patients without previous transplant.
The purpose of this study is to evaluate the feasibility of performing RARP in patients who have previously received a renal allograft and to compare their outcomes with those of patients without a history of renal transplantation.
Patients and Methods
After Institutional Review Board approval, a retrospective review was performed of 228 consecutive patients undergoing RARP for localized CaP at a single institution between February 2005 and December 2008. Of the 228 patients, 3 patients had renal allografts in the pelvis at the time of surgery. Preoperative demographics, perioperative parameters, and postoperative outcomes were collected for all patients. Operative time was defined as the time from the skin incision until the final dressing was applied. Continence was assessed by the self-reported number of urinary pads the patient wore per day. Statistical analysis was performed using chi-square and a two-tailed unpaired Student's t-test to compare the transplant group with the nontransplant control group with significance at 0.05.
In the patients with no previous transplant, selected medical clearances were obtained in high-risk patients. A surgical four-arm robotic platform (da Vinci,® Intuitive, Sunnyvale, CA) was used in all patients with a bedside assistant and a 6-port transperitoneal approach (Fig. 1a).
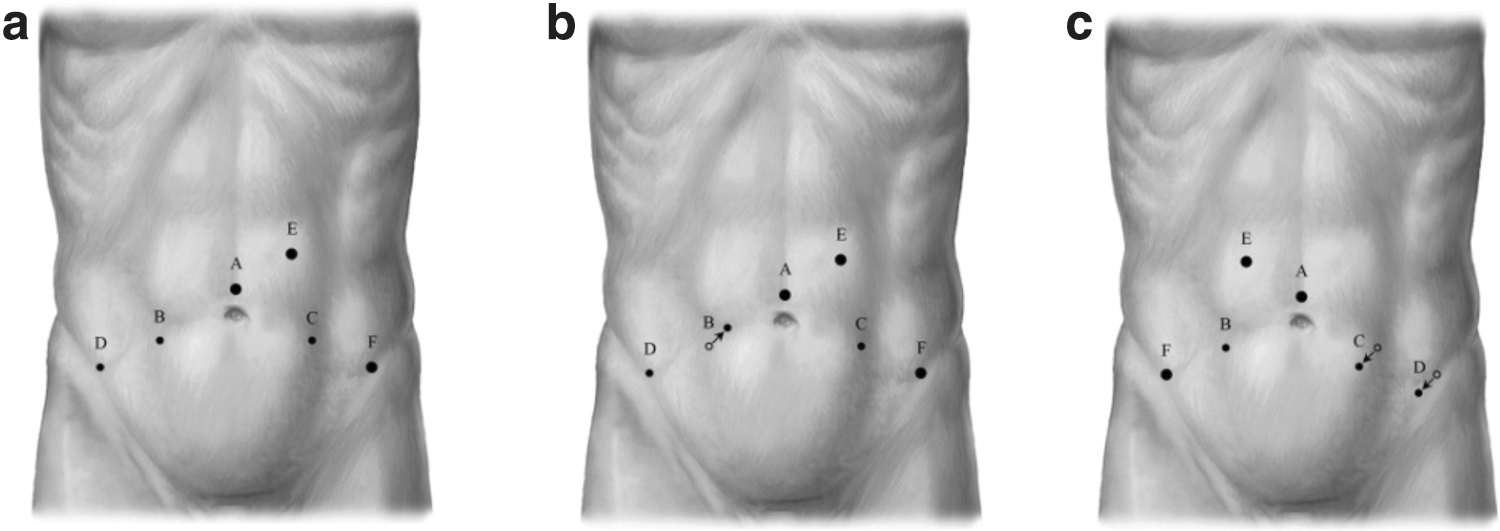
Port placements.
All surgeries on patients with renal allografts were performed by the same surgical team (PDL and DDB). Additional preoperative preparation was performed in the three transplant patients, including an extensive preoperative cardiac evaluation and consultations with the renal transplant service. The immunosuppressive regimen was adjusted in the preoperative period with assistance from the transplant team. A preoperative steroid bolus and postoperative taper were administered. In preparation for surgery, all patients underwent a mechanical bowel preparation.
One previous renal transplant patient had undergone bilateral renal transplantation with subsequent removal of a renal allograft from the left side, with his recent allograft harbored on the right. Robotic port placement in this patient was modified from the conventional port placement to optimize exposure to the pelvis while avoiding trauma to the allograft (Fig. 1b). The right arm was moved cephalad and medial, and the other ports remained in their standard locations.
The second patient, who was previously on peritoneal dialysis, underwent an open Hasson technique to establish pneumoperitoneum after unsuccessful Veress needle placement. After extensive lysis of adhesions and inspection of the pelvic anatomy, the assistant was moved to the contralateral (right) side because of the medial location of the left allograft and the narrow pelvis (Fig. 1c). The two left robotic arms, including the left and fourth arms, were moved medially and caudally to improve the angle of access to the prostate over the transplanted kidney.
The third previous transplant patient had a 10-cm allograft on the left after receiving a left lower quadrant transplant 22 years ago. Standard port placement (Fig. 1a) was maintained despite the challenging dissection because of the large size of the renal allograft and its medial position in the pelvis, which almost completely obscured the left endopelvic fascia and the left side of the prostate (Fig. 2). Arm adjustments were used to improve angles during the procedure.

Intraoperative picture displaying medially placed large left renal transplant obscuring access into the ipsilateral pelvis.
In all previous transplant patients, a meticulous technique with minimal use of electrocautery in the region of the ureter was used to prevent ischemic injury of the ureter. In these patients, the graft ureter and kidney were surrounded by a moderate to severe amount of fibrosis and induration. Caution was used not to dissect too closely to this area of scarring to avoid injury to the ureter. In addition, care was also taken to avoid traction on the transplant ureter and periureteral tissues during exposure of the ipsilateral endopelvic fascia.
In all patients, the dorsal vein was routinely sutured or stapled using a bariatric automatic stapling device, depending on surgeon preference. Nerve-sparing and pelvic lymph node dissections were performed as appropriate based on patient pretreatment parameters.
Results
RARP was completed successfully in all three patients with previous renal transplantation. Operative time was comparable between the renal transplant group and the control group (322 vs 300 min, respectively; P=0.65). Graft rejection or changes in creatinine were not observed in these patients. Similarly, there were no infectious complications in renal transplant recipients despite immunosuppression. No medical or surgical complications in the transplant group were noted. Similarly, all other perioperative and postoperative variables of the renal transplant group were comparable to those of the control group (Table 1). The prostate-specific antigen (PSA) level was undetectable in all three renal transplant patients using an ultrasensitive PSA assay (<0.03 ng/mL) at a mean of 13 months. In addition, all transplant patients were continent at short-term follow-up, needing no urinary pads.
ASA=American Society of Anesthesiologists; TNM=tumor-node-metastasis; EBL=estimated blood loss.
Discussion
Renal transplantation has become the treatment of choice for paients with end-stage renal disease. 5 As immunosuppression regimens have improved, so have survival rates after renal transplantation. 2 Unfortunately, there is an increased risk of cancer development in renal transplant patients compared with the general population because of their immunocompromised status. 1 The cumulative incidence of CaP is 3.1% at 3 years, which follows only skin cancer 1 and lymphoma. 6
With improving graft survival, treating patients with localized CaP using radical prostatectomy remains appropriate, because these patients have a life expectancy of more than 10 years. In addition, renal transplant recipients in whom end-stage renal disease develops secondary to graft failure will not be considered candidates for retransplantation at most centers with untreated prostate cancer. Inability to qualify for retransplantation can jeopardize patient survival, because patients who are receiving hemodialysis while awaiting transplant have a 5-year survival rate of 16% compared with a 70% 5-year survival in patients who receive a transplant. 7 Therefore, treatment for CaP in this population may be beneficial and lifesaving. 8
Open radical prostatectomy has been reported in patients with previous renal transplantation, including the open retropubic approach 9 –13 and the perineal approach. 14,15 The perineal approach may reduce iatrogenic graft injury by avoiding the transplant operative field but does not allow a lymph node dissection without a separate incision. In addition, the perineal incision in an immunocompromised patient is a potential source of wound infection. Finally, the general lack of familiarity with this technique also may explain the limited use of this approach. 14,15 In contrast, the open retropubic surgical approach is familiar to urologists but may be made more complicated because of obliteration of the retropubic space by the previous transplantation and a high sepsis rate because of a larger incision combined with poor wound healing. 16
Radiation has also been applied in the treatment of CaP in renal transplant patients. Mouzin and colleagues 17 applied 70 Gy to the prostate in eight previous kidney transplant patients using conformal radiation. PSA recurrence developed in 25% of patients, however, at a mean follow-up of 28 months, and transplant ureteral anastomotic strictures developed in 25% of patients. 17 With half of patients experiencing poor outcomes at relatively short follow-up, the early experience with radiation therapy in this population appears to be suboptimal.
There are some conflicting reports regarding the success of laparoscopic radical prostatectomy in previous renal transplant patients. 3,6,18 Thomas and associates 3 reported that three previous renal transplant patients who were treated laparoscopically had surgical challenges that were no greater than those in standard patients. In contrast, Robert and coworkers 6 reported their experience with nine renal transplant recipients undergoing LRP through an extraperitoneal approach and compared them with a control group. They reported a single transplant patient with positive surgical margins and none with biochemical recurrence at 12 months. They did note a much higher incidence of rectal injury in the transplant group compared with the control group (22% vs 1.8%; P=0.022), suggesting greater surgical complexity in these patients.
Both studies concluded that LRP is a feasible surgery in carefully selected patients with a previous transplant, but that the technique requires advanced laparoscopic skills. Certainly the use of straight laparoscopic instruments that do not flex over the renal transplant may increase the complexity of this procedure and might have played a role in the high rate of rectal injury reported in the latter study.
With the advent of the da Vinci robotic platform, the use of minimally invasive surgery to treat patients with CaP has been increasing, because RARP is now the most common surgical approach for CaP in the United States. 19 There are potential advantages of the robotic platform compared with a standard laparoscopic approach for radical prostatectomy in previous transplant patients. The advantages of RARP include wristed instruments that allow for easier suturing particularly working over the graft and the enhanced visualization of the magnified, high-definition picture to aid in identification of the transplant ureter and other important surgical anatomy. Development of the planes behind the prostate may be easier with instruments that can flex over the graft to create a better angle of dissection, which also allows for easier access to the ipsilateral pelvis for dissection. Compared with the perineal approach, the robotic approach allows a simultaneous lymph node dissection and avoids the increased infectious risks of operating through the perineum.
Jhaveri and associates 4 reported the first RARP in a patient with a previous renal transplant. They concluded that this procedure was feasible but needed technical modifications from a standard approach. These modifications included using an extended length bariatric port to bypass the allograft site and deliver the ipsilateral robotic instrument directly into the pelvis. They also developed the retropubic space from the contralateral side.
Our findings also support the feasibility of RARP in this patient population. In performing these surgeries, we identified key components that should be undertaken in patients with previous transplant. The previous extraperitoneal surgical dissection of the kidney transplantation may significantly obliterate the ipsilateral retropubic space, and this scarring combined with the space occupying renal graft may present a unique challenge to the surgeon because of increased adhesions and distorted anatomy.
Preoperative review of the operative notes for the transplant procedure is important to clarify relevant graft anatomy. In all three patients, an end to side anastomosis of both the renal artery and vein into the external iliac artery and vein, respectively, was used. Initially, the surgeon must anticipate intra-abdominal adhesions even in patients with no previous intra-abdominal surgeries. In all three patients, omental adhesions to the area of the transplant were identified. The intra-abdominal adhesions may be greatest in patients with previous periteoneal dialysis and, in particular, with previous episodes of peritonitis.
A bowel injury in an immunocompromised patient is a dangerous and potentially life-threatening complication, and the surgeon should be prepared for an open Hasson technique if initial Veress insufflation fails. After abdominal entry and lysis of adhesions, the surgeon should assess the pelvic anatomy to determine the optimal locations for additional port placement. Factors that increase the complexity of the surgery are a narrow pelvis, medial location of the graft, extensive scar tissue around the graft, which makes it fixed in location, and anterior insertion of the ureter into the bladder.
In all three of our patients, the ureter was anastomosed directly to the bladder. The more distal (toward the prostate) and anterior the implantation of the ureter into the bladder was, the more difficult the exposure became. Adjusting the ports medial and caudal on the side ipsilateral to the graft will improve orientation into the pelvis. In addition, the robotic ports with their articulations allow easier access into the pelvis over the graft. The majority of the dissection in the pelvis must be performed from the contralateral side. In these patients, the approach angles into the plane behind the prostate are difficult, so this dissection must be performed cautiously to avoid inadvertent rectal injury.
Constant surveillance of the allograft and ureter to ensure that undue tension is not being applied will protect these structures. In our series, a 0-degree lens, similar to the lens in conventional patients, was used during the majority of the procedure. If visualization over the graft into the ipsilateral pelvis is difficult, a 30-degree down lens may be used, and a 30-degree up lens may help in taking the rectum off the prostate. Our technique of posterior reconstruction and the modified Van Velthoven urethrovesical anastomosis were identical to that in conventional patients.
We feel that the transperitoneal approach was optimal, because it avoided the obliterated retropubic space. Normal surgical planes can still be encountered with this approach, making the dissection less cumbersome. Cystoscopy with stent placement to identify the ureter location is an option, although we did not feel this was necessary. Certainly, any injury to the graft or ureter could significantly decrease the transplant patient's long-term survival, because a damaged allograft decreases life expectancy more than untreated prostate cancer. On the other hand, patients with renal failure who need clearance for another life-saving transplant may not be considered if they have a detectable PSA level, so the stakes are very high for this procedure.
Using immunosuppression adjustments, careful surgical technique, and meticulous postoperative care, all transplant patients were free of wound complications, urinary tract infections, and sepsis. In our experience, we found that RARP in renal transplant recipients was significantly more difficult than RARP in patients without a prior transplant. Although this procedure could be performed in any high-volume center, performance in a transplantation center facilitates communication with the transplantation team both in the preoperative and perioperative period. We feel strongly that an integrated team approach in the care of these complicated patients will improve postoperative outcomes.
Nerve-sparing techniques and pelvic lymph node dissections were performed as appropriate in the entire population. Because of the low risk of metastatic disease, we did not perform a lymph node dissection in the three transplant patients. Certainly, an ipsilateral node dissection would be difficult with the graft in place, and the potential risk to the graft blood supply may not be justified. Furthermore, contralateral node dissection may result in greater difficulty in the event of a future transplant. In addition, we feel that nerve-sparing techniques should be applied cautiously in this population to ensure a negative margin and undetectable PSA level. A wide resection was performed in all three patients, resulting in an undetectable PSA level with no evidence of clinical or biochemical recurrence at 12 months of follow-up.
Our study also compared renal transplant recipients who were undergoing RARP with patients without previous renal transplantation. We noted similar outcomes between the groups despite the challenging surgical features of the transplant patients. Although our study reported good oncologic outcomes at short follow-up, the small size of the series necessitates a larger experience with longer follow-up to fully understand the long-term efficacy of RARP in patients with renal allografts. Another limitation of our study is the bias associated with a retrospective analysis. Although a randomized comparison would be ideal, this comparison would be difficult to perform because of the rarity of patients who present with both CaP and a history of renal transplantation. Despite these limitations, our study demonstrates that excellent outcomes after RARP are achievable in previous renal transplant recipients.
Conclusions
RARP is feasible in patients with both CaP and a previous renal transplant. Having a history of renal transplant surgery provides challenges to the robotic procedure. These can be overcome, however, with careful preparation and modifications to standard robotic technique, allowing the patient to benefit from the reduced morbidity and excellent oncologic outcomes of RARP.
Footnotes
Disclosure Statement
D. Duane Baldwin serves on the scientific advisory board for Onset Medical Corp. No competing financial interests exist for all other authors.