
Abstract
Background and Purpose:
Hemostatic agents have been suggested as an adjunct for tubeless percutaneous nephrolithotomy (PCNL). We pathologically evaluated the percutaneous tracts injected with the fibrin sealant (FS) Evicel and hemostatic gelatin matrix (HGM) Surgiflo at various time intervals to determine their absorption and tract closure rates. We also evaluated whether these agents reduced urine leak rates in a porcine model.
Materials and Methods:
Percutaneous access was obtained in 19 kidneys in 10 domestic swine. The tracts were dilated to 30F using a balloon dilating catheter. Ten kidneys served as controls. Surgiflo was injected into the tract of four kidneys, and Evicel was injected into the tract of five kidneys. Intravenous urography (IVU) was performed on postoperative days (POD) 1 and 10 to 14. IVU was performed on two pigs at POD 30. The pigs were sacrificed and kidneys were harvested for pathologic evaluation.
Results:
Two (20%) control kidneys had a urine leak on IVU on POD 1. None of the kidneys treated with HGM or FS had a urine leak on POD 1. None of the kidneys had a leak on POD 10 to 14 or POD 30. On pathologic inspection, the tracts of all the control kidneys and HGM kidneys had closed completely at POD 14. Two kidneys treated with FS had fistula at POD 6 and POD 14. At POD 30, the tracts in the control kidneys and kidney treated with HGM had completely healed. Fibrin sealant remained in the tract at POD 30.
Conclusion:
Fibrin sealant should be used with caution because it can persist in the tract for up to 30 days and may inhibit wound healing. Hemostatic gelatin matrix is the preferable agent because the tract closed by POD 10 to 14, similar to the findings in the control animals. The use of hemostatic agents in a nephroscopy tract may reduce the risk of early urine leak after tubeless PCNL.
Introduction
We pathologically evaluated percutaneous tracts injected with the fibrin sealant (FS), Evicel® (Johnson and Johnson, Somerville, NJ) and the porcine gelatin matrix combined with thrombin, Surgiflo® (Johnson and Johnson, Somerville, NJ) at different time intervals to determine the absorption rates of these materials and tract closure rates in a porcine model. We also investigated the effectiveness of these hemostatic agents at preventing urinary leaks.
Material and Methods
After obtaining approval by the Institutional Animal Care and Use Committee, 10 female juvenile farm pigs with a nominal body weight of 80 lb (36.3 kg) underwent percutaneous access in 19 kidneys.
Surgical technique for percutaneous access
After induction of general anesthesia, the pig was positioned prone. A semirigid ureteroscope was used to place a 0.038 in guidewire up the ureter, followed by insertion of a 6F externalized ureteral catheter. Retrograde pyelography was performed with iodinated contrast to delineate the collecting system. After skin incision, an 18-guage needle was placed percutaneously into the collecting system under fluoroscopic guidance. A 0.038 in guidewire was placed down the ureter under fluoroscopic guidance. After placement of a second (safety) guidewire, a 30F balloon dilator (Nephromax-Boston Scientific, Marlborough, MA) was placed over the working wire and inflated with dilute iodinated contrast to a pressure of 12 atm. Fluoroscopy was used to confirm appropriate positioning of the balloon, and a 30F percutaneous access sheath was placed. A rigid nephroscope was placed through the access sheath to confirm correct placement into the collecting system. The sheath was left in place for 15 minutes.
In the kidneys that served as controls, the sheath was removed, and the skin was closed with interrupted 2-0 nylon sutures. For the kidneys that were treated with the FS Evicel or the hemostatic gelatin matrix (HGM) Surgiflo, the rigid nephroscope and the access sheath were pulled back to the visualized edge of the collecting system. The depth from the collecting system to the edge of the access sheath was determined by marking the place on the nephroscope immediately protruding from the sheath. The nephroscope was removed, and the distance from this mark to the tip was measured. This represents the distance from the outer edge of the access sheath to the edge of the collecting system.
The applicators for either the FS or the HGM were then cut to the appropriate length, approximately 2 to 3 mm less than the distance from the outer edge of the access sheath to the edge of the collecting system. The applicators were then placed through the sheath, and the FS or HGM was slowly injected while pulling both the applicator and sheath back slowly. This was done to prevent either agent from being injected into the collecting system. A total of 10 mL of each agent was used. The skin was closed with interrupted sutures.
Imaging
All pigs underwent imaging on postoperative day (POD) 1 with intravenous urography (IVU). All pigs underwent IVU between POD 10 and 14 with the exception of one pig that was euthanized on POD 6 because of sepsis. Two pigs were kept alive to POD 30 and underwent one additional IVU. One of these pigs had two control kidneys, and the other had FS injected into one tract and HGM injected in the other. Imaging was reviewed for any signs of urinary extravasation from the percutaneous site or any signs of obstruction.
Pathologic studies
All pigs were sacrificed immediately after the IVU on POD 10 to 14, with the exception of three pigs: Two pigs were sacrificed on POD 30 after an IVU; one pig was euthanized on POD 6 secondary to sepsis. The kidneys from all pigs were removed and inspected grossly. The tracts were examined to determine if they had been properly sealed and to determine grossly if there was any residual HGM or FS.
Results
Access was successfully obtained in 19 of the 20 kidneys. Ten kidneys served as controls and had no agents injected. A total of five kidneys had Evicel injected into the tract, and four kidneys had Surgiflo injected into the tract. In one kidney, percutaneous access could not be obtained, but the contralateral kidney had successful access and the tract was injected with FS. This pig was euthanized on POD 6 because of sepsis from peritonitis related to ureteral perforation during the unsuccessful access attempt. There were no other complications related to access.
Imaging
There was evidence of urine leak in 2 of 10 control kidneys (Fig. 1) and in none of the kidneys that had either FS or HGM injected into the tract on POD 1 (Table 1). There were no leaks seen on IVU in any of the kidneys beyond POD 1. There was no evidence for obstruction on any of the imaging studies.
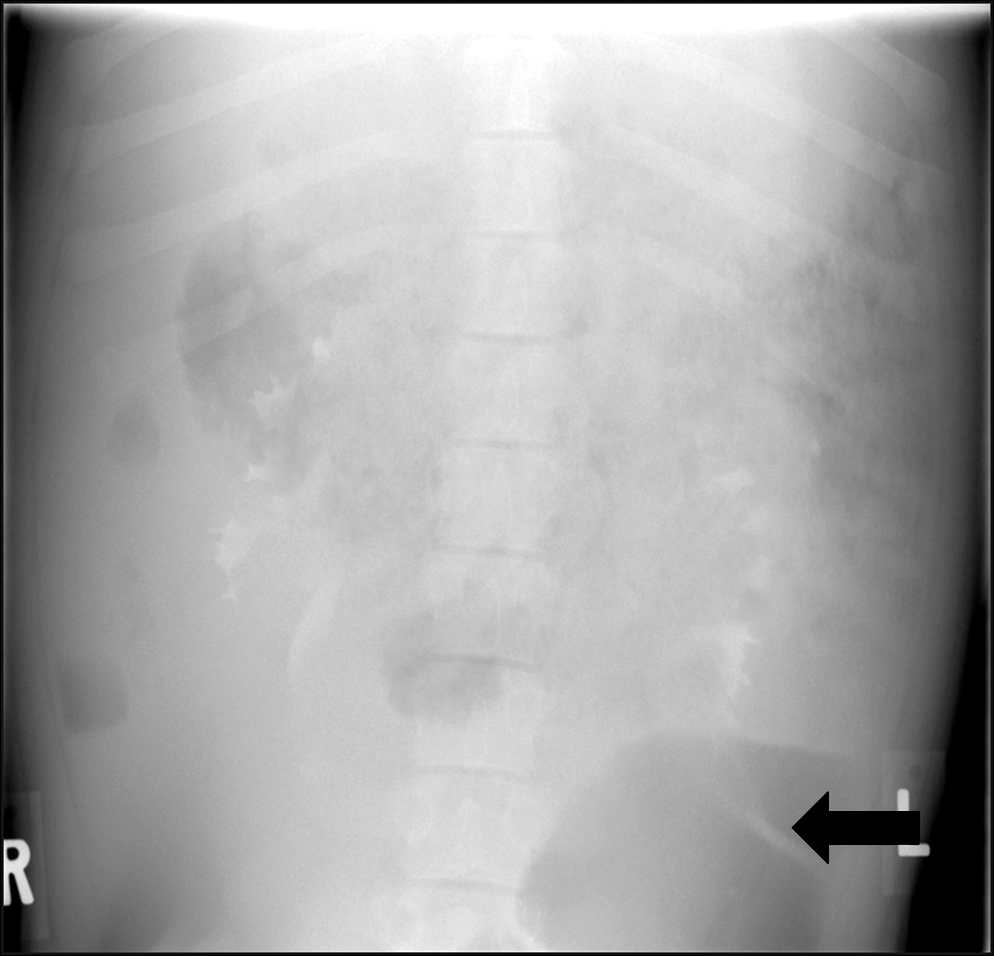
Intravenous pyelogram from a control pig on postoperative day 1 demonstrating a urine leak from the left lower pole. Arrow points to extravasated contrast.
IVU=intravenous urography; POD=postoperative day.
Pathologic analysis
Pathologic results are summarized in Table 2. At the time of harvest, the percutaneous access tracts in all the control kidneys had healed and were closed (Fig. 2a). There was a persistent fistula in one of three kidneys that were treated with FS that were harvested on POD 10 to 14. This fistula measured 3 mm in diameter and extended from the collecting system through the parenchyma to the capsule. On gross inspection, there was no evidence of residual FS in the fistula. Evicel was found in the tract of the kidney that was harvested on POD 30; however, the collecting system and capsule had healed, so there was no fistula (Fig. 2b). All of the tracts that were treated with HGM were closed at the time of harvesting, and on gross inspection, there was no evidence of HGM found in any of the tracts (Fig. 2c). There was no evidence of obstruction or residual FS or HGM within the collecting system on pathologic inspection of any of the kidneys that were treated with these agents.

Pathologic evaluation of the nephroscopy tract at postoperative day 30. Tract denoted by circle.
POD=postoperative day.
One pig had to be euthanized on POD 6 because of sepsis that was caused by a ureteral perforation. Access was obtained in the contralateral kidney, and FS was injected into the tract. On autopsy, there was a persistent fistula measuring 6 mm in diameter extending from the collecting system all the way through the capsule (Fig. 3). There was no evidence of residual FS in the tract. There was a significant amount of urine in the retroperitoneum.
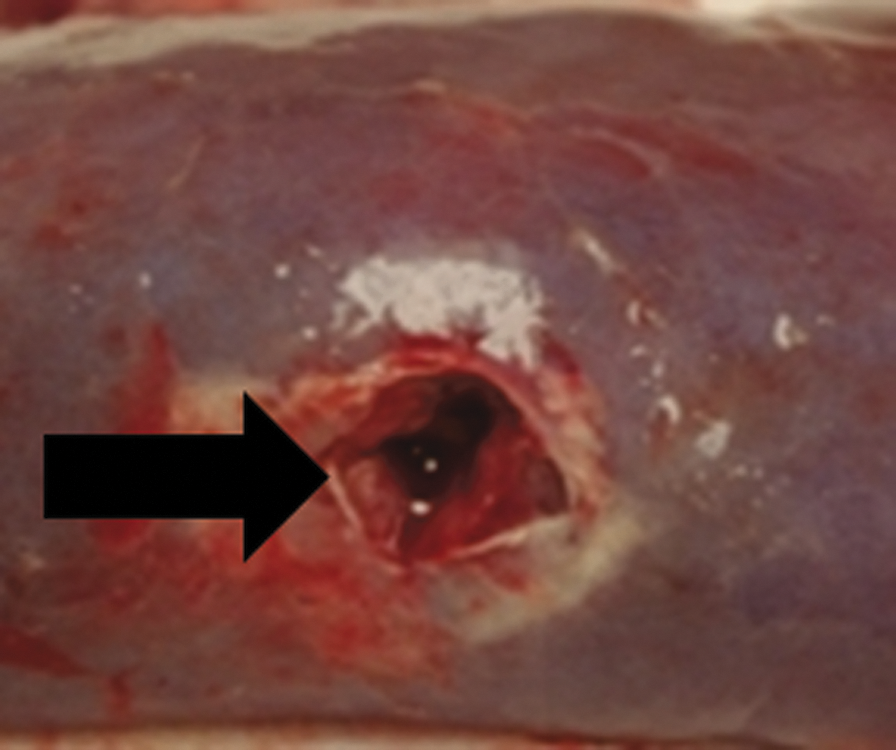
Image of the fistulous tract on pathologic evaluation of the tract injected with Evicel on postoperative day 6. Arrow points to fistula opening on the capsule of the kidney.
Discussion
Nephrostomy tube placement at the conclusion of PCNL was initially considered standard of care. The perceived advantages of nephrostomy tube placement were to allow for access to the collecting system if further percutaneous surgery is planned, to aid in hemostasis, and to prevent urinary extravasation. The major disadvantage of nephrostomy tube placement is the discomfort that is associated with the tube. Recent studies suggest that not placing a nephrostomy tube, so-called tubeless PCNL, is a safe alternative, with reduced patient discomfort and pain. 1
The safety and efficacy and reduced patient morbidity after tubeless PCNL has been confirmed in randomized trials. 2,3 In these trials, an internal ureteral stent was placed antegrade at the conclusion of the PCNL in the tubeless group. There was no difference in the change in hematocrit in either of these studies. In both of these trials, there was a longer duration of urine leakage from the nephroscopy site after nephrostomy tube removal when compared with the tubeless patients. This may be accounted for by the internal ureteral stent left in place in the tubeless group.
In addition to these randomized trials, a recent comprehensive review of tubeless PCNL concluded that tubeless PCNL has similar complication rates with decreased patient morbidity when compared with standard PCNL. 1 Despite these reports demonstrating no difference in transfusion rates or change in hemoglobin value in patients who were undergoing tubeless PCNL, a number of surgeons have reported placing hemostatic agents in the percutaneous tracts as an adjunct during tubeless PCNL. Both FS and gelatin matrix have been used in the percutaneous tract. Mikhail and associates 4 retrospectively reviewed their experience with the FS Tisseel® (Baxter Healthcare, Hayward, CA) in the percutaneous tract and compared this maneuver with a control group of patients who underwent tubeless PCNL. Patients who had Tisseel injected into the tract had a significantly shorter hospital stay; however, there was no difference in hematocrit drop, analgesic use, or complications between the two groups. On postoperative CT, they noted no significant changes along the nephrostomy tract when compared with the preoperative CT.
In a randomized study comparing tubeless PCNL with and without Tisseel, there was no significant difference in drop in hematocrit or transfusion rates between the two groups. 5 There was a significant decrease in analgesic requirement in the patients who received Tisseel. Patients were evaluated with ultrasonography at POD 1 and 1 to 2 weeks after surgery, and no urinomas were noted.
A third study examined the use of Surgicel placed in the nephroscopy tract of patients who were undergoing totally tubeless PCNL. 6 Twenty patients were randomized to undergo totally tubeless PCNL with or without Surgicel placed in the tract. The authors found no difference in the change in hematocrit value between the groups. In both groups, 20% of the patients had evidence of a urinoma on ultrasonography on POD 2.
HGM has been used in percutaneous tracts after tubeless PCNL as well. Lee and colleagues 7 reported on two patients who underwent tubeless PCNL and used the HGM Floseal® (Baxter Healthcare, Hayward, CA) injected into the percutaneous tract. They demonstrated stable postoperative hematocrits and no evidence of hematoma or obstruction on CT on POD 1.
Based on the studies comparing tubeless PCNL with and without the use of hemostatic agents, there does not appear to be a clear clinical advantage to the use of these agents. There has been no pathologic evaluation to determine what happens to these agents once they are placed in the nephroscopy tract. To our knowledge, this is the first study performed to pathologically evaluate what happens to these agents in the percutaneous tract after tubeless PCNL. On gross pathologic inspection, all of the control tracts were completely closed at POD 10 to 14. The tracts injected with Surgiflo were all closed on POD 10 to 14 with no residual HGM in the tracts. The single tract injected with HGM evaluated at POD 30 was also closed. Our studies suggest that HGM does not appear to lead to fistula formation.
In the kidneys that were treated with Evicel, 60% of the tracts remained open. These findings raise concern about injecting FS into the tract after tubeless PCNL. As FS is absorbed over time, a fistulous tract may form and lead to a delayed urine leak. There was no evidence of this finding on imaging in the present study, but there was a fistula in one of the tracts treated with FS on POD 10 to 14 on pathologic inspection. In the pig sacrificed on POD 6, there was a large fistula in the tract treated with FS, and there was a significant amount of fluid in the retroperitoneum, suggestive of urine leak. In addition, FS was still present in the tract at POD 30. Plasminogen, which normally aides in fibrinolysis, is not present in Evicel. 8 The lack of plasminogen slows down the breakdown of the fibrin plug and may explain why it persisted in the tract for up to 30 days.
On radiographic imaging with an IVU in the current animal study, there were no urine leaks in the five kidneys that were treated with FS or the four kidneys that were treated with HGM at 1 day or 2 weeks after the procedure. In the one kidney that was treated with FS and the one kidney that was treated with HGM that were evaluated on POD 30, there was no evidence of urine leak. On POD 1, 20% of the control kidneys had radiographic evidence of urine leak. This leak rate is higher than has been reported for patients undergoing tubeless PCNL. 2,3 These clinical investigations, however, did not evaluate patients with contrast studies postoperatively, and internal ureteral stents were placed in the tubeless group, which may explain their lower urine leak rates. There were no urine leaks in any of the control kidneys at POD 10 to 14 or POD 30. Although it is difficult to make a definitive conclusion based on this small sample size, it appears that the hemostatic agents are effective at preventing urine leaks immediately postoperatively, and there is no evidence for delayed leaks over time on imaging with IVU.
Urinary obstruction from hemostatic agents entering the collecting system is also a concern. Uribe and coworkers 9 demonstrated that when mixed with urine, the fibrin sealant Tisseel formed a solid clot in vitro. This study found that the HGM Floseal formed a fine colloidal suspension. After 5 days, the Tisseel had still not completely dissolved. In a follow-up study, hemostatic agents were injected directly into the porcine collecting system. 10 All the kidneys were evaluated with an IVU 24 hours after the procedure. There was evidence of obstruction in 50% of the kidneys injected with Tisseel and Floseal on IVU. The pigs were sacrificed 5 days after surgery, and there was evidence of obstruction on autopsy in 50% of the kidneys that were injected with these agents. In the current study, radiographic evaluation demonstrated no evidence of obstruction on IVU on POD 1, POD 10 to 14, or POD 30 in any of the kidneys that were injected with Evicel or Surgiflo. On pathologic evaluation, there was no evidence of residual FS or HGM within the collecting system.
There are several limitations of the present study. It is unclear if the urine leaks in the control kidneys found on IVU on POD 1 have any clinical significance. These leaks all resolved by POD 10 to 14, and there was no urine found in the retroperitoneum on pathologic inspection. The clinical significance of Evicel persisting in the tract is unknown. The small number of kidneys studied makes statistical comparisons difficult.
This is the first animal study to pathologically evaluate nephroscopy tracts treated with hemostatic agents at different time intervals. Based on the above findings, if a hemostatic agent is going to be placed in the percutaneous tract after PCNL, we recommend the use of HGM over FS. Use of HGM may reduce urine leak in patients who undergo tubeless PCNL without an internal ureteral stent. There is no evidence of delayed urine leak with HGM, and on pathologic inspection, the percutaneous tracts injected with HGM are completely closed with no evidence of residual HGM. FS, such as Evicel, should be used with caution after tubeless PCNL, because they may lead to fistula formation between the renal collecting system and the retroperitoneum. Further clinical trials are warranted to assess the safety and efficacy of hemostatic agents placed in the nephroscopy tract after tubeless PCNL.
Conclusion
The use of hemostatic agents placed in the nephrostomy tract after tubeless PCNL may reduce urine leakage. The gelatin matrix Surgiflo is completely reabsorbed with complete tract closure without evidence of delayed urine leak over time. The FS Evicel may persist in the percutaneous tract for up to 30 days, and its reabsorption in the tract may lead to a fistula and possible delayed urine leak. FS, such as Evicel, should therefore be used with caution. When placing a hemostatic agent after tubeless PCNL, HGM appears to be preferable to FS.
Footnotes
Disclosure Statement
David Albala is a speaker for Ethicon. No competing financial interests exist for any of the other authors.