
Abstract
Background and Purpose:
The application of a water-jet dissector for mucosal elevation was shown to improve resection of lesions of the gastrointestinal tract. We present the first prospective clinical trial on the application of a combined water-jet dissector and needle-knife (HybridKnife) in transurethral dissection (TUD) of urothelial carcinoma of the bladder (UCB).
Patients and Methods:
Thirty separate urothelial tumors of the bladder in 17 unselected patients were elevated and dissected with the HybridKnife. The goal was to determine the safety, effectiveness of resection, and overall applicability of the HybridKnife.
Results:
No perforation or other complication was seen. All tumors could be dissected from the bladder wall en bloc. TUD of UCB by using the HybridKnife is technically feasible and safe in the resection of papillary and solid tumors.
Conclusion:
The application of the HybridKnife in TUD of UCB appears to be a feasibly safe and applicable for en-bloc dissection technique potentially following principles of oncologic surgery in transurethral removal of UCB. It seems to facilitate histopathologic assessment. A possibly improved oncologic outcome has to be addressed in further studies.
Introduction
One reason for the high recurrence rates that are associated with conventional TURB is that its technique is diametrically opposed to the fundamental oncologic surgical principle of removing a tumor en bloc by dissecting surrounding normal tissue. According to the 2010 European Association of Urology guidelines, only tumors less than 1 cm can be dissected en bloc, while larger tumors have to be resected separately in fractions. 4 Thus, UCB is usually fragmentized during TURB and tumor cells spilled within the bladder, potentially being implanted into the bladder wall spurring recurrence. 5 –7
This issue could be overcome with a dissection technique adopted from gastroenterology using a water-jet dissector. Removal of colorectal tumor lesions showed favorable long-term outcomes, and it has been postulated that it may largely replace colectomy for node-negative colorectal cancer. 8 The present study reports the first prospective clinical evaluation of transurethral water-jet dissection of UCB.
Patients and Methods
Study design
This is a prospective evaluation of both the applicability and safety of the HybridKnife® (ERBE, Tübingen, Germany) in transurethral removal of UCB. The study was approved by Institutional Ethical Review Board.
HybridKnife: Technical aspects
The HybridKnife (I-Type, Ø2.3 mm, length 1.9 m, No. 20150-061) is a multifunctional probe combining water-jet and electrosurgical surgery technology. The water jet (ERBEJet® 2) is applied through a stainless steel tube incorporating a microcapillary lumen with a diameter of 120 μm (Fig. 1), which is connected with a radiofrequency generator (VIO 300D; mode Forced Coag E2, 50W for cutting and hemostasis). The HybridKnife is fixed in a custom-produced CE-certified resection slide (27042HL, STORZ, Tuttlingen, Germany) allowing axial movement, inserted in an ordinary 26F resection shaft (27040SL, STORZ, Tuttlingen, Germany).

HybridKnife.
Preclinical studies
Preclinical studies on ex-vivo pig bladders were performed (Samed Resection, Typ LS 20-2, SAMED GmbH, Dresden, Germany). The water-jet applicator was placed directly on the bladder wall, and the optimal pressure for mucosal elevation was evaluated. At a pressure of 30 bar, a vigorous elevation of the bladder mucosa and submucosa by hydrodistention of superficial fibers of the detrusor muscle was reliably observed, which we dubbed “bleb-effect” (Fig. 2). Thirteen different mucosal and submucosal areas with a mean diameter of 2 cm were elevated by a fluid cushion and resected in the level of the superficial detrusor with the HybridKnife. The bladders were dissected and examined macroscopically by the surgeon. No perforation was seen. The specimens, assessed by an uropathologist, showed a selectively created fluid cushion within the upper muscular layers (Fig. 3). The resected specimens contained sufficient muscle for valid histopathologic evaluation. 9

Application of HybridKnife: Creation of bleb effect and dissection.
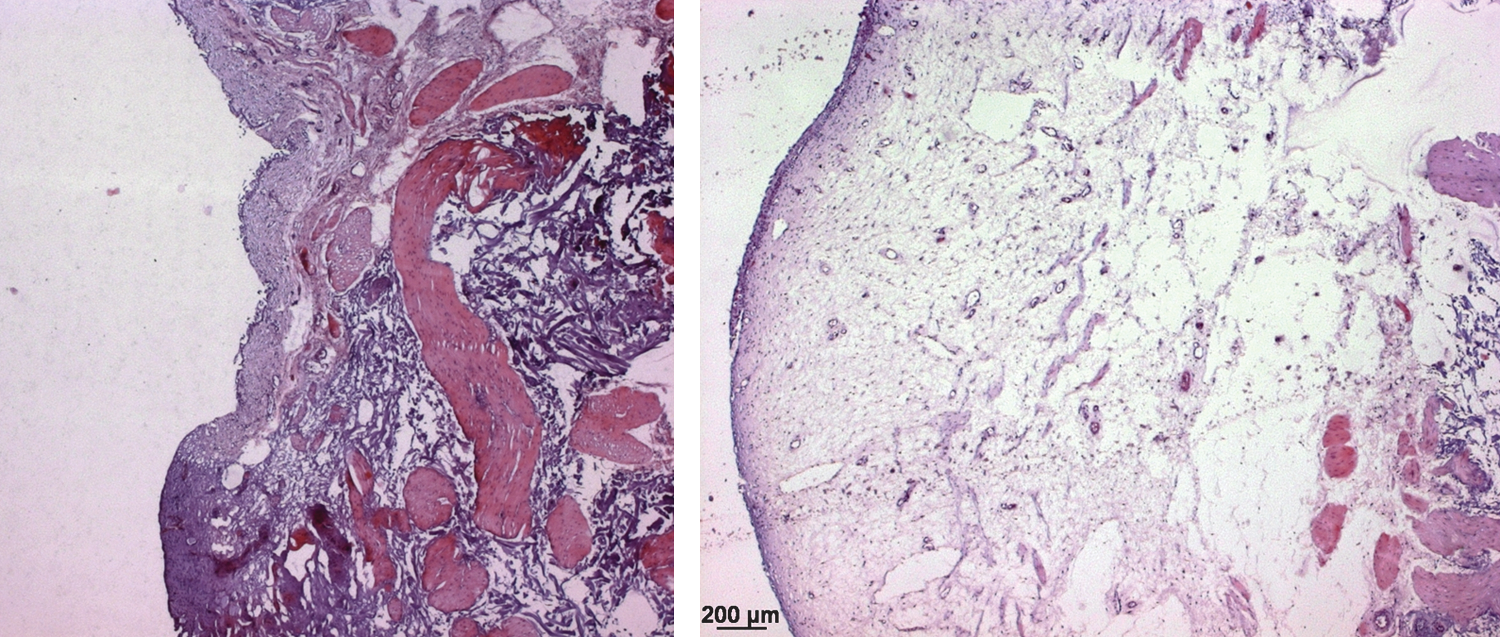
Normal urothelium before and after application of water jet.
Patient selection
Patients with cystoscopically suspicious primary lesions within the urinary bladder were consecutively included, regardless of flat, papillary, or solid tumor appearance or size. Informed consent was obtained. The singular exclusion criterion was a tumor highly suspicious of muscle invasion (ie, large tumor with solid aspect). The intention was to distinguish tumors appropriate for water-jet dissection from those that were not.
Resection technique
Photodynamic diagnostic was applied in every patient to clearly define tumor margins. The water-jet applicator of the HybridKnife (diameter 120 μm) was directly placed on normal mucosa surrounding the tumor and the water jet was activated with a pressure of 30 bar for the needleless injection of saline that was colored with indigo carmine. The HybridKnife was used for mucosal incision, further dissection, and for repeated saline injection when needed, without having to exchange the instruments. Hemostasis was accomplished by use of the electrosurgical function of the HybridKnife (VIO300, ERBE: Forced Coag E2, 50W; EndoCut Q 2-4-1). Whenever considered necessary by the investigator, muscular tissue was to be resected by common TURB after transurethral dissection (TUD).
The tumors were extracted with an endo-bag (Multi-Bag standard-bag retrieval bag, 70×35 mm, 20 mm bag depth 2.5 mm–230 cm or Roth standard-basket 25 mm oval, 1.8 mm–120 cm, both EndoTechnik, Solingen, Germany) (Fig. 4), commonly used in gastroenterology, preserving the structure of the tumor and thus helping to avoid tumor cell spillage and saving optimal prerequisites for histopathologic evaluation.
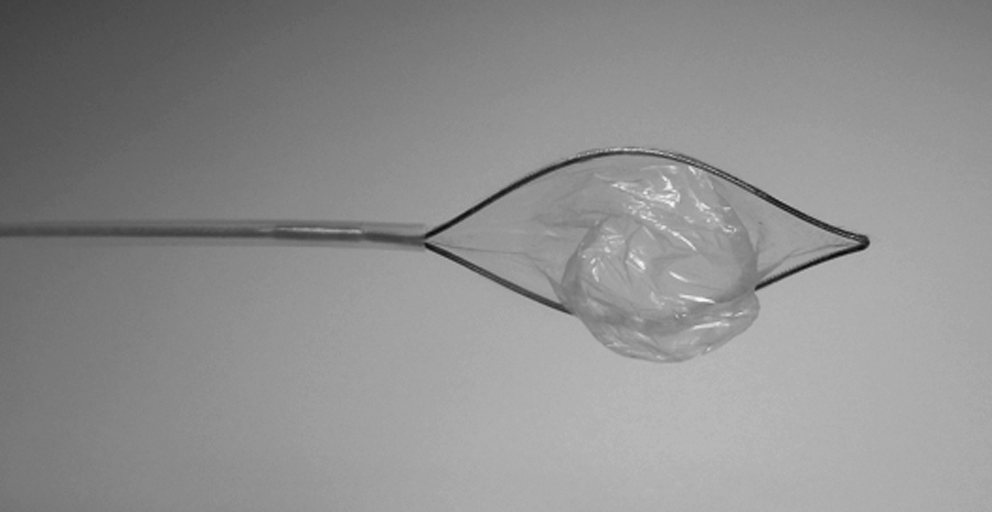
Roth standard-basket 25 mm oval, 1.8 mm–120 cm.
An indwelling transurethral catheter was placed and remained as long as judged necessary by the investigator. Ultrasonoraphy of the lower abdomen and kidneys was performed 1 day after TUD.
Measurements
The surgeon judged the applicability and handling of the HybridKnife. Detailed operative time was not measured. Any perforation or bleeding that could not be managed with the HybridKnife was defined as a complication. The histopathology of the specimens was assessed by a uropathologist. Resection margins were inked with dye (Fig. 5).

Hematoxylin and eosin-stained urothelial carcinoma of the bladder stage pTaG3; dye-inked resection margin on left side.
Results
Thirty separate tumors were resected in 17 patients (Table 1). No perforations or other complications were seen. The transurethral en-bloc dissection of UCB by the HybridKnife was technically feasible and safe in the dissection of papillary and solid tumors. The time taken to use the HybridKnife in papillary and solid tumors was judged comparable to that of conventional TURB, with a steep learning curve. In contrast, the removal of larger flat lesions was time consuming and not judged advantageous compared with conventional TURB by the investigators. Achievement of hemostasis was facilitated through the buildup of mucosal pressure by the water jet.
Hg=high grade; CIS=carcinoma in situ; lg=low grade; MMC=mitomycin-C.
The largest resected tumor had a diameter of 7.5 cm and weighed 46 g. The largest tumor able to be extracted smoothly en bloc via the urethra had a diameter of 1.6 cm.
The depth of dissection was controllable. Muscle was present in all TUD samples, which is an important indicator of surgical quality in TURB. 10 Only one case was judged to need conventional resection of detrusor muscle after TUD by the investigator. All indwelling catheters were removed 2 and 3 days after TUD, respectively. Ultrasonography on day 1 revealed no abnormalities.
One patient showed muscle-invasive tumor stage. Consecutive radical cystectomy was performed, and histology revealed pT0. Two patients with stage pT1 underwent control TURB technique within 10 weeks of the TUD, showing no residual tumor. Oncologic outcome was not the subject of the present study.
Histopathologic evaluation showed sufficient depth of dissection for valid judgment in all specimens. In the solid tumors that could be harbored en bloc, the surgical margin was inked, finally allowing the pathologist to establish the tumor stage as R0. In one case of a stage pT1 tumor, a clear lymphovascular invasion (LVI) of the tumor was diagnosed.
Discussion
The goal of the presented study was to gain first clinical experience with TUD of UCB using a water-jet dissector with regard to safety and effectiveness of resection and overall applicability. The HybridKnife proved easy to handle with a steep learning curve. There were no complications. Water-jet–aided dissection is predicted to become the mainstay of therapy for node-negative colorectal cancer. 8 The TUD of UCB is even safer compared with colonic resection, because the muscularis propria in the urinary bladder is by far thicker compared with the colon.
Lodde and associates 11 published a small series of tumors with a diameter of up to 2.5 cm that were resected en bloc using a flat loop. The present study is the first to describe a technique enabling a transurethral en-bloc dissection of even larger UCB with a diameter of up to 7.5 cm. The only exclusion criterion in the present trial was tumor that was highly suspicious of muscle invasion. Two types of tumor seem not to profit, however. For one, in smaller tumors (<0.8 cm), there is no real benefit compared with TURB that could also be dissected en bloc by the common resection loops. Second, TUD of large flat lesions was not judged advantageous compared with conventional TURB by the investigator. In flat lesions that are suspicious of carcinoma in situ (CIS), no complete en-bloc removal rather than accurate sampling has to be achieved, because specific therapy for CIS consists of adjuvant treatment with bacilli Calmette-Guérin. Because sufficient depth of resection cannot be reliably assessed during the procedure, seemingly nonmuscle-invasive UCB would appear to be the only feasible subject for TUD.
TUD of UCB provides an obvious facilitation of histopathologic assessment, potentially resulting in a more valid tumor staging and risk assessment and thus improved planning of further therapy. It not only avoids fragmentation of tumor, but also reduces fulguration artifacts, enabling the pathologist to describe depth of infiltration, resection margin, and LVI more precisely. In particular, LVI in TURB specimen has great potential to become a reliable factor in the judgment of early-invasive T1 UCB concerning further treatment needs. 12 The present study, however, can but suggest such an effect, lacking comparison with standard resection. Because the histopathologic assessment was not clearly addressed, further studies including defined histopathologic criteria are warranted. While a reduced spillage of tumor cells from TUD may be suggested when compared with TURB, no statement can be made with regard to a respective potential effect. In addition, the handling of TUD was judged by the investigator without a standardized assessment tool; while handling seemed feasibly simple in the present series, no insight on the comparability with standard TURB can be derived.
What is the perspective of TUD of bladder tumors? The present study, with a straight consecutive series of patients consenting to the water-jet dissection of their tumor, allows the definition of the following inclusion criteria for further studies: Early invasive or possibly even early muscle-invasive UCB up to a size determined by the diameter of the urethra. Recently, holmium laser TURB or plasmakinetic TURB have been shown not to be advantageous with regard to rate of recurrence when compared with a conventional TURB. 13 Clearly, there is a need to evaluate potential oncologic benefits of TUD, which the present study does not address. This supports the notion that further examinations of this technique are needed, this method adhering to ubiquitous oncologic principles not followed by the conventional TURB procedure.
Conclusion
We conclude that water-jet–aided TUD of UCB appears to be a feasibly safe and applicable en-bloc resection technique following oncologic principles. It appears to facilitate histopathologic assessment. Potential benefits for the oncologic outcome have to be assessed in further studies that address recurrence and progression rates.
Footnotes
Acknowledgments
We thank Patrick Goldsworthy for his excellent assistance.
Financial support for trial material was granted by ERBE, Tübingen, Germany.
Disclosure Statement
The authors have no conflicting financial intrests.