
Abstract
Background and Purpose:
Renal transplant lithiasis represents a rather uncommon complication. Even rare, it can result in significant morbidity and a devastating loss of renal function if obstruction occurs. We present our experience with graft lithiasis in our series of renal transplantations and review the literature regarding the epidemiology, pathophysiology, and current therapeutic strategies in the management of renal transplant lithiasis.
Patients and Methods:
In a retrospective analysis of a consecutive series of 1525 renal transplantations that were performed between January 1983 and March 2007, 7 patients were found to have allograft lithiasis. In five cases, the calculi were localized in the renal unit, and in two cases, in the ureter. A review in the English language was also performed of the Medline and PubMed databases using the keywords renal transplant lithiasis, donor-gifted lithiasis, and urological complications after kidney transplantation. Several retrospective studies regarding the incidence, etiology, as well as predisposing factors for graft lithiasis were reviewed. Data regarding the current therapeutic strategies for graft lithiasis were also evaluated, and outcomes were compared with the results of our series.
Results:
Most studies report a renal transplant lithiasis incidence of 0.4% to 1%. In our series, incidence of graft lithiasis was 0.46% (n=7). Of the seven patients, three were treated via percutaneous nephrolithotripsy (PCNL); in three patients, shockwave lithotripsy (SWL) was performed; and in a single case, spontaneous passage of a urinary calculus was observed. All patients are currently stone free but still remain under close urologic surveillance.
Conclusion:
Renal transplant lithiasis requires vigilance, a high index of suspicion, prompt recognition, and management. Treatment protocols should mimic those for solitary kidneys. Minimally invasive techniques are available to remove graft calculi. Long-term follow-up is essential to determine the outcome, as well as to prevent recurrence.
Introduction
Urologic complications are among those concerning the graft per se and are mostly irrelative to administered regimens. Their reported incidence in large series is 2.6% to 15% and is correlated with several potential risk factors, among them patient age, the method used to restore primary urinary continuity, and the regimens of immunosuppression. 1 Urologic complications include urinary leakage and/or ureteral obstruction, ureteral stricture, ureteral necrosis, vesicoureteral reflux, and graft lithiasis. 2,3 In our series of 1525 consecutive renal transplantations over 24 years of experience, the reported incidence of urologic complications was 6.3%. 4
Renal transplant lithiasis represents a rather uncommon complication, but it can lead to significant morbidity and to a devastating loss of graft function if obstruction occurs. The management of allograft lithiasis is a challenging situation because of the medical complexity of these cases and the extra-anatomic location of the allograft kidneys.
We present our experience with patients with graft lithiasis. Data on treatment outcomes are reported and compared with similar data of other series in the literature.
Patients and Methods
Retrieved data of a consecutive series of 1525 renal transplantations that were performed between January 1983 and March 2007 were retrospectively analyzed. In seven (0.46%) patients, allograft lithiasis was found. All seven transplants were obtained from cadaveric donors. Three patients had no symptoms or sign of obstruction, and gross hematuria developed in one patient.
A systematic review in the English language was also performed of the MEDLINE and PubMed databases using the keywords renal transplant lithiasis, donor-gifted lithiasis, percutaneous nephrolithotomy (PCNL), and extracorporeal shockwave lithotripsy (SWL). All relevant articles were studied in full with particular emphasis on large series of kidney transplantation, in which graft lithiasis cases were identified and managed with current treatment modalities. The selection of these articles was based on the following key points: Large number of kidney transplantations, long-term follow-up of the transplanted patients that led to identification of the graft-lithiasis patients,treatment of these patients, and treatment outcome.
Results
Intervention and follow-up characteristics of our series are summarized in Table 1. In five cases, the calculi were localized within the renal unit, and in two cases, in the ureter. Mean time of lithiasis presentation post-transplantation was 3.2 years (2–7 years). Mean stone size was 1.45 cm (0.4–2.5 cm). All graft calculi were radiopaque. In all patients, tertiary hyperparathyroidism was found, despite cinacalcet hydrochloride administration, and therefore an increased urine calcium load was a common laboratory finding.
Died from acute pulmonary edema, not related to intervention.
After second transplantation.
SWL=shockwave lithotripsy; PCNL=percutaneous nephrolithotomy; NA=not applicable.
In three cases, where significant obstruction was observed, nephrostomy tube and antegrade Double-J-stent insertions were performed. The nephrostomy tube was removed 3 days after the antegrade insertion of the Double-J stent by the radiologist.
Intervention was decided on stone size and location. Stones >2 cm were managed by PCNL. Ureteral stones and stones smaller than 2 cm were managed by SWL, because of the difficult approach via the ureter. Of the seven patients, three were treated via PCNL; in three patients, SWL was performed; and in a single case, spontaneous passage of a urinary calculus was observed.
PCNL was performed in all three cases with the patient in the supine position. Percutaneous access was achieved by using ultrasonography and fluoroscopy (Figs. 1, 2). One patient with previous ureteropyelostomy (the recipient's own ipsilateral ureter has been used) underwent simultaneous ureterolithotripsy. Complete stone removal was achieved in all three cases. The SWL treatment was performed with the Dornier SLII lithotripter. The patients were placed in the prone position, and the stone localization and targeting was achieved by using fluoroscopy. A total of 3000 shocks were delivered in each session, and complete stone fragmentation was achieved in all cases, which was confirmed post-treatment by plain radiography (Figs. 3, 4).

Plain radiography of the kidneys, ureters, and bladder with the stone in the left side transplanted kidney.
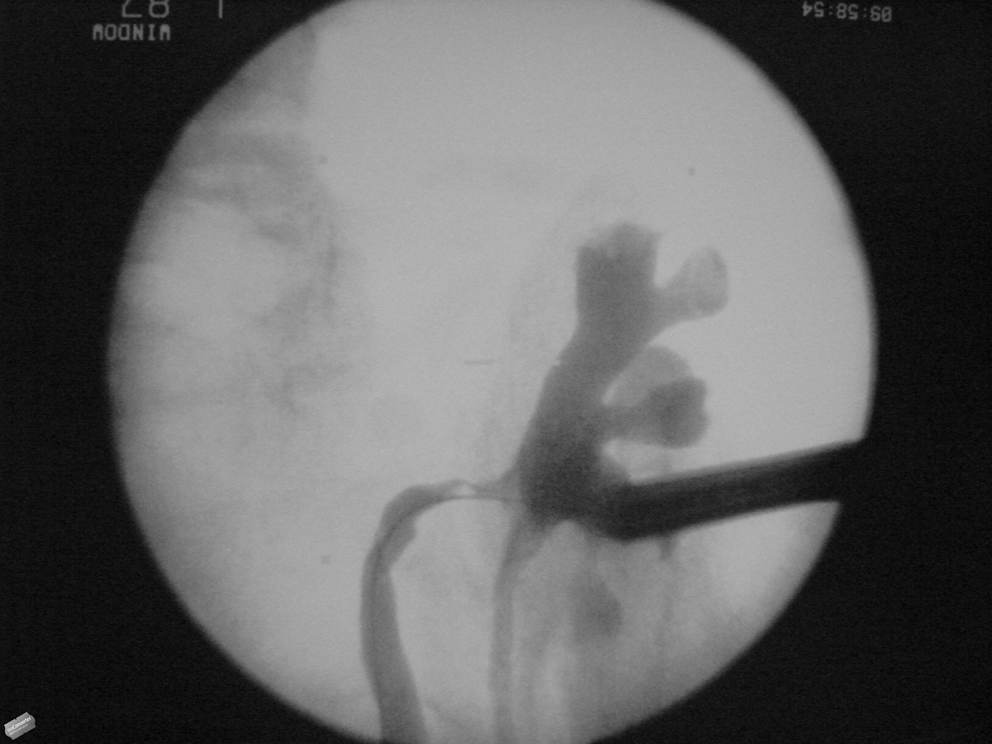
Intraoperative fluoroscopic image during percutaneous nephrolithotomy.

Plain radiography of the kidneys, ureters, and bladder: Renal graft lithiasis before shockwave lithotripsy.

Plain radiography of the kidneys, ureters, and bladder: Fragmentation of the graft stone postshockwave lithotripsy.
Two patients already had a Double-J stent in place. Close follow-up was applied to detect early obstructive disease from residual stone fragments. The patients were able to spontaneously pass the stone fragments with no intervention. No perioperative or postoperative complications were observed, and all patients are currently stone free but still remain under close urologic surveillance. Unfortunately, no stone analysis was performed, and thus no data regarding the stone composition are available.
Mean follow-up time was 8 years. Follow-up of these patients included ultrasonographic examination 3 months postintervention and every 6 months thereafter. Serum determinations of blood urea nitrogen (BUN) and creatinine levels were also provided at the same time. No dimercaptosuccinic acid (DMSA) or diethylenetriaminepentaacetic acid (DTPA) was needed, because all patients had normal BUN and creatinine values postintervention.
From the reviewed articles, no prospective studies were found. Most of the studies were retrospective, and Table 2 outlines selected series of graft lithiasis.
In these series are also patients included with stones located in the bladder.
SWL=shockwave lithotripsy; PCNL=percutaneous nephrolithotomy; URS=ureteroscopy.
Discussion
Renal transplant lithiasis has been recognized as a complication of renal transplantation since 1975, when the first case of a calculus in a kidney transplant was described by Rattiazzi and associates. 5 Renal transplant lithiasis represents a rather uncommon complication, although the incidence varies significantly among different series. Most studies report an incidence of 0.4% to 1%. 6 Abbot and colleagues 7 reported retrospective records of 42,096 renal transplant recipients, based on the United States Renal Data System, indicating an incidence of 0.11% for males and 0.15% of females. Recently, Buresley and coworkers 3 retrospectively reviewed the medical records of 646 renal transplant recipients for urologic complications. Graft lithiasis was reported with an incidence of 0.17%. Similar studies, however, bearing smaller numbers of patients, report incidence rates ranging from 0.23% to 6.3%. 8,9 In our series, incidence of graft lithiasis was 0.46% (n=7).
Etiology of graft lithiasis
Allograft stones may be already placed in situ, the so-called donor-gifted allograft lithiasis, or may be the result of new stone formation after transplantation. 10 The latter is believed to be a multifactorial phenomenon, related to both metabolic and urodynamic parameters. Thus, stone formation theories suggest that when certain physicochemical conditions are present in the urinary tract, stone formation may occur.
Several factors have been considered to predispose to graft lithiasis. 11 Urinary stasis, reflux, recurrent urinary tract infection, renal tubular acidosis, pH changes, supersaturated urine, decreased inhibitor activity, tertiary hyperparathyroidism, hypercalcemia, and hypercalciuria are present at higher rates in allograft kidneys and considered as predisposing factors for stone formation. 8,12 Tertiary hyperparathyroidism is a common finding in renal transplant patients, which can explain the increased urine calcium load. 13 Actually, tertiary hyperparathyroidism represents the inability of the parathyroid glands to restore normal function and resume normal serum calcium levels after kidney transplantation. Benoit and colleagues 14 in their series report an incidence of calculus formation up to 14% in hyperparathyroid renal transplant recipients. In our series, all patients with graft lithiasis were found to have hyperpathyroidism, and therefore an increased urine calcium load was a typical laboratory finding in all of them.
Urinary tract infections, especially with Proteus mirabilis, constitute both a causative agent and a result of renal transplant lithiasis, especially in cases of encrustaded retained ureteral stents. 15 Nonabsorbable suture material (eg, use of stapled ureteroureteral anastomosis) has also been implicated in renal stone formation, because it may act as a nidus, probably from harboring of bacteria. 1,16 Nutritional habits, such as high dietary protein intake, and medications, such as vitamin D and calcium may also be contributing factors. 17 Immunosuppresive therapy with calcineurin inhibitors, such as cyclosporine, is known to produce hyperuricosuria in 50% to 60% of patients, by decreasing renal filtration and possibly by direct tubular damage. 18 Decreased citrate excretion and increased serum and urine excretion of uric acid and calcium compared with controls seem to play a major role.
Several studies have previously been made to identify the importance of risk factors in graft lithiasis. Harper and associates 19 reported statistically significant hyperexcretion of uric acid and calcium in stone formers compared with controls (5.5 vs 3.9 mmol/24h, P=0.027 and 6.4 vs 3.9 mmol/24 h, P=0.064 respectively). In the same series, urine of stone formers was found to be also less acidic compared with controls (pH=6.4 vs 6.0, P=0.05).
These findings suggest that despite the presence of the above mentioned multifactorial predisposing factors, the risk of forming calcium-containing stone may be associated with increased water excretion and more concentrated and alkaline urine. These data would also explain the fact that most stones in renal allografts have been reported to be calcium oxalate, 20 although hyperuricemia is the most common metabolic disorder found in renal transplant recipients with lithiasis. 21 Data on uric acid lithiasis are conflicting. There are studies reporting a rate of uric acid stones of 8% to 10%, 19 while another study did not reveal an increased risk of uric acid urolithiasis and reported only a 0.2% rate in this cohort. 8
Donor-gifted allograft lithiasis
Transplant preexisting lithiasis was first described in 1985, 22 and it has yielded suggestions for routine pretransplant screening both in living and cadaveric donors. Until recently, stone-bearing kidneys in the live-donor setting have traditionally not been accepted for transplantation in most centers. In 1996, Kasiske and coworkers 23 issued guidelines on the selection of renal transplant donors. They stated that nephrolithiasis was at least a relative contraindication to donation because of the known risk of recurrence. With increasing organ shortages, however, the use of suboptimal donors was becoming more accepted. 24
In 2005, these guidelines were reviewed by Davis and Delmonico, 25 who relaxed the restrictions on potential donors and nephrolithiasis by suggesting that an asymptomatic potential donor with a current single stone may be suitable if the donor is not at high risk for recurrence and the current stone is less than 15 mm in diameter. In an effort to determine which donors are at risk for recurrence, the authors suggested that potential donors with a history of cysteine/struvite stones or systemic diseases, such as primary or enteric hyperoxaluria, distal renal tubular acidosis, sarcoidosis, inflammatory bowel diseases, or other diseases that can cause nephrocalcinosis, should not be eligible to donate.
The Amsterdam Forum on the Care of the Live Kidney Donor outlined eligibility criteria for asymptomatic potential donors with a history of a solitary stone. 26 According to these, donors must have no hypercalciuria, hyperuricemia, metabolic acidosis, cystinuria, or hyperoxaluria, no urinary tract infection, and no CT evident multiple stones or nephrocalcinosis. Moreover, Devasia and associates 27 suggested that asymptomatic stone-bearing voluntary donor kidneys detected during screening can be considered for transplantation in carefully selected and compliant cases. These data indicate that stone recurrence rates and subsequent morbidity in patients with a history of nephrolithisasis and a solitary kidney stone are essential for risk determination in renal transplant donors. 24
Donor graft lithiasis is currently estimated to be approximately 0.64%. 28 Nevertheless, if nephrolithiasis is recognized before transplantation, then the treatment can be performed via SWL in the live donor, or by bench techniques on the donor kidney. Open pyelotomy is the traditional method; however, ureteroscopic ex-vivo techniques to remove stones have also been used. Rashid and colleagues 29 reported their experience of a series of donor patients who underwent living related renal transplantation, in which the donor kidney underwent ex-vivo ureteroscopic stone treatment at transplantation, suggesting that this method is a technically feasible means of rendering a stone-bearing kidney stone free without compromising ureteral integrity or renal allograft function. Nevertheless, minor stones are left in situ or may not be perceived and are only detected after transplantation. 30
Clinical manifestations
Although rare, nephrolithiasis of the transplanted kidney can result in significant morbidity and a devastating loss of renal function if obstruction occurs. Because of renal and ureteral denervation, inherent to the transplantation procedure, the classic renal colic is absent. 22 Symptoms mimicking acute rejection may appear, or recurrent infections may cause injuries similar to those of chronic pyelonephritis. Therefore, if ongoing asymptomatic obstruction occurs, acute renal failure or a syndrome similar to acute rejection may be the first clinical signs of disease. A palpable mass from renal dilation and hydronephrosis sometimes is present, and vague abdominal discomfort in the iliac fossa, where the transplant lies, because of irritation of the overlying fascia and abdominal wall 11 might be reported. Anuria is the presentation of complete ureteral obstruction.
The reported mean time of lithiasis presentation post-transplantation in several series is 1.6 to 3.6 years. 13,31 In our series, mean time of lithiasis presentation post-transplantation was 3.2 years (2–7 years), and this finding is consistent with that of the previous series.
Management of transplant lithiasis
The management of allograft lithiasis is a challenging situation because of the medical complexity of these cases and the extra-anatomic location of the allograft kidneys. Generally, treatment protocols for calculi in the transplanted kidney should mimic those for a solitary kidney. 31 The management of renal transplant lithiasis includes observation; SWL; endourologic, percutaneous, and open approaches.
Asymptomatic graft renal stones of <4 mm in diameter, once diagnosed, can be managed conservatively, and often there is a spontaneous passage in the recipient. The patient, however, has to be counseled appropriately, and the compliance of the patient has to be very good. 8 In our series, only in a single case was a spontaneous passage of a urinary stone observed.
SWL
Currently, SWL constitutes the method of choice for small and middle-sized stones with a diameter approximating 1.5 cm. 14,31,32 Previously published series have reported successful sessions of SWL for small stones in the transplanted kidney. 8,20,33 SWL, however, may be hindered by the usual position of the allograft in the pelvis. The bony pelvis not only makes stone localization difficult, because it can preclude the use of fluoroscopic location of the stone, but also can cause shockwave attenuation, with consequently decreasing efficacy. 34 These problems can be solved by placing the patient in the prone position, so that the kidney lies next to the shockwave generator, although even then, overlying bowel may cause difficulty with shockwave delivery. 11,31
The most important concern of SWL is that of ureteral obstruction after stone fragmentation because of stone fragments that are too large to pass spontaneously through the ureteral lumen. The use of Double-J stents is controversial. 35 Thus, despite good results and less morbidity reported by several studies, the position and orientation of the transplanted ureter is responsible for the often unsuccessful attempts to gain retrograde access to the upper urinary tract, limiting the feasibility of stent insertion, as well as of an endoscopic approach. Therefore, better drainage may be achieved with a nephrostomy tube; it is relatively straightforward, because of the superficial position of the transplanted kidney. Consequently, close follow-up with serial ultrasonography is needed, because the altered pain response makes managing steinstrasse difficult. 20
PCNL
PCNL in a renal transplant was first described in 1985 by Hulbert and coworkers, 36 and since then several isolated successful descriptions have been made. More recently, some small series have been published. 31,37 –40 PCNL has the advantage of potentially removing all stone fragments at one procedure. Therefore, it can be performed for removal of stones larger than 1.5 cm in diameter, especially in cases of caliceal and pelvic stones, and it is argued to be effective in the management of a significant stone burden. 41 In a recent series, 39 PCNL was performed for stone removal with average stone size of 32 mm (20–50 mm). Stone-free rates have been reported to be 77% to 100% in these series, and low recurrence rates (<10%) have also been cited. 39,40
Several concerns regarding this procedure, however, have also been cited. As mentioned, the pelvic position of the kidney and its relatively superficial location facilitate the percutaneous approach with the patient in the supine position, but it may also predispose to adjacent organ injury—namely, the overlying bowel. Indeed, the risk of bowel perforation must be kept under consideration, because, in contrast to conventional PCNL, access to the transplanted kidney is usually gained through an anterior calix, so that during puncture, the use of ultrasonography in addition to fluoroscopy is essential. 20
In addition, after transplantation, perirenal reactive tissue in the form of a fibrous sheath usually develops, so that percutaneous tract dilation can be very difficult with consecutive increase of significant bleeding risk. Moreover, this perirenal fibrosis may limit the use of the rigid nephroscope, necessitating the use of a flexible instrument for the inspection of all parts of the kidney and ureter. 40
In a recently published small series, 42 PCNL was performed using a 16F miniature nephroscope, and the approach was considered safe and effective in the management of graft lithiasis, with complete stone removal without compromising graft function. The authors suggested that this approach is ideal for most cases of upper urinary tract stones in transplanted kidneys, other than simple and small stones in the middle and lower calix.
Nevertheless, the standard 27F rigid nephroscope can be used according to a previous series. 40 The authors in their series of 13 patients with renal transplant lithiasis treated with PCNL noted no adjacent organ injury during the percutaneous access tract creation and no difficulties with dilating the tract or inserting the rigid nephroscope. In our patients treated with PCNL, the 26F rigid nephroscope (Karl Storz GmbH, Germany) and an Amplatz sheath were used, and no problems regarding tract dilation or nephroscope insertion were noticed.
The most commonly reported complications of PCNL in renal transplant recipients include sepsis, gastrointestinal bleeding, herpes esophagitis, development of cutaneous urinary fistula, perinephric urinoma after nephrostomy tube removal, and impaired wound healing and are primarily related to patient immunosuppression. Therefore, most centers would delay PCNL in the initial period after transplantation because of the higher levels of immunosuppression. 31
Ureteroscopic management
Flexible ureteroscopy with subsequent electrohydraulic lithotripsy or holmium laser is a challenging but effective means for managing renal transplant and ureteral calculi. Del Pizzo and colleagues 43 in a series of 14 patients who underwent ureteroscopy reported success in 13 of them by using a 7.5F flexible ureteroscope for most patients with no stones and an 8F semirigid ureteroscope for those with a ureteral calculus. Ureteral stones can be managed via endoscopy, which is sometimes combined with SWL.
Ureteroscopy poses quite satisfying results if used properly, and success rates in removing ureteral stones or encrusted ureteral stents in renal transplants have been reported to be as high as 78%. 44 Because the ureteroneocystostomy may be at the dome, anterior wall, or high on the posterior wall, however, the access can be very difficult and may be often unsuccessful. It has been suggested that by introducing the ureteroscope over a guidewire, the problem can be countered, because this way can offer support to the allograft ureter, because the lack of soft tissue support of the allograft ureter makes ureteroscopy, especially rigid ureteroscopy, very risky.
Devasia and associates 27 suggest that ureteral reimplantation during transplantation of stone-bearing donor kidneys should be such that it facilitates ureteroscopy later if needed. Even so, in cases in which ureteroscopy is not possible, a combined percutaneous and flexible ureterorenoscopic approach has been reported. 15
Open surgery
Open surgery is rarely needed to treat the aforementioned cases and should be the last resort, applied only to cases in which all other means of therapy have failed, or in very rare cases of staghorn calculi, which cannot be removed with minimally invasive techniques. The main reason that contributes to the significant difficulties of open procedures is immunosuppression. Immunosuppressive drugs are known to have profibrotic and ischemic properties. Therefore perinephric, capsular, and subcapsular fibrosis as well as loss of capsular vessels are common findings in renal transplants, so that surgical reinterventions are very difficult. 39
Follow-up
Currently, there is no consensus regarding the post-treatment follow-up of graft-lithiasis patients. In several studies, a relatively short mean follow-up period of 33 months 27 and 1.91 years, 7 respectively, has been reported, whereas in another study, all patients were entered into a surveillance program with regular ultrasonography of the transplant; however, the follow-up period was not defined. 31 In our study, the mean follow-up after treatment was 8 years.
Because of lack of evidence, we recommend a follow-up period of at least 5 years. Follow-up of these patients should include ultrasonography 3 months postintervention and every 6 months thereafter. Serum determinations of BUN and creatinine levels should be provided at the same time. It should be noted, that these two parameters are not used as renal function markers, but they may assist in evaluating poor hydration of the lithiasis patients, which is extremely important.
Earlier imaging and blood work should be performed in symptomatic cases. Scintigraphy with DMSA or DTPA is not needed when patients have normal BUN and creatinine values postintervention, and it can be omitted.
Conclusion
Renal transplant lithiasis is uncommon, but it can lead to significant morbidity and to loss of graft function. Therefore, it requires vigilance, a high index of suspicion, prompt recognition, and management. Treatment protocols should mimic those for solitary kidneys in general. Multiple, less invasive techniques are available for the management of renal transplant lithiasis. Moreover, a multimodal management may further increase the rate of successful treatments. In addition, long-term follow-up is essential to determine the outcome, as well as to prevent recurrence.
Footnotes
Disclosure Statement
No competing financial interests exist.