
Abstract
Purpose:
The study compared characteristics and outcomes in patients with staghorn or nonstaghorn stones who were treated with percutaneous nephrolithotomy (PCNL) within the Clinical Research Office of the Endourological Society (CROES) PCNL Global Study.
Patients and Methods:
Data over a 1-year period from consecutively treated patients from 96 centers worldwide were collated. The following variables in patients with staghorn or nonstaghorn stones were compared: National prevalence, patient characteristics, access method, puncture frequency and outcomes, including bleeding rates, operative time, and duration of hospital stay.
Results:
Data from 5335 eligible patients were collated; 1466 (27.5%) with staghorn and 3869 (72.5%) with nonstaghorn stones. Staghorn stone presentation varied between centers from 67% in Thailand to 13% in Argentina. The frequencies of previous procedures were similar between groups, but shockwave lithotripsy was less frequent in patients with staghorn stones compared with nonstaghorn (16.8% vs 22.6%) and positive preoperative urine cultures were more frequent in patients with staghorn than nonstaghorn stones (23.4% vs 13.1%). Patients with staghorn stones underwent multiple punctures more frequently than those with nonstaghorn stones (16.9% vs 5.0%). Postoperative fever, bleeding, and the need for blood transfusion were more frequent, the median operative time and duration of hospital stay were longer, while the proportion of patients remaining stone free was lower (56.9% vs 82.5%) in patients with staghorn than nonstaghorn stones.
Conclusions:
The proportion of patients with staghorn stones varies widely between centers. Stone-free rates were lower, complications more frequent, and operative time and hospital stay were longer in patients with staghorn stones.
Introduction
Although in use for 30 years, recent refinements to the technique of percutaneous nephrolithotomy (PCNL) currently make it the preferred first-line therapy for renal stones that are not amendable to extracorporeal shockwave lithotripsy (SWL), such as large volume and staghorn calculi. 8 Nevertheless, the management of staghorn calculi with PCNL remains challenging. Compared with the management of nonstaghorn stones, a number of investigators have reported that the use of PCNL in the management of staghorn calculi is associated with increased risks, such as increased renal hemorrhage and blood transfusion requirement. 3,8,9 Large studies that assess the actual level of risk in the management of staghorn calculi by PCNL, however, have not been undertaken, and debate continues over whether stone-free rates with this technique are adequate when compared with other interventions.
The PCNL Global Study was instigated by the Clinical Research Office of the Endourological Society (CROES) to generate a global database on the utility of the technique as assessed primarily by stone-free rate 30-days post-PCNL and secondarily through assessment of morbidity and other factors influencing outcomes. 10,11 Previous publications from the study have focused on complication rates 12 and tract dilation methods. 13,14 The current analysis examines outcomes in patients who presented with staghorn or nonstaghorn stones.
Patients and Methods
The CROES PNCL Global Study is a prospective observational study for which the study organization and methods have been described in detail previously. 12 In brief, 96 centers worldwide participated in the study, and each submitted data from consecutively treated patients for a 1-year period. Patients who were eligible for the study were those who had PCNL either for primary or secondary treatment for nephrolithiasis during the study period. There were no specific exclusion criteria. A stone was classified as staghorn when located in the renal pelvis and was in at least two of the calices. PCNL procedures were performed according to local guidelines and practices.
Ultrasonography and/or radiography in combination with fluoroscopy guided access to the upper tract. Once access was achieved, following proper caliceal puncture of the collecting system, a guidewire was inserted and maneuvered toward the ureter. Thereafter, dilation of the tract was achieved either with balloon, telescopic, or serial dilators to allow positioning of an Amplatz sheath and passage of a rigid nephroscope. After nephroscopic inspection, lithotripsy by laser, ultrasound, or ballistic means was performed, and various stone graspers were used to remove stone fragments; if indicated, flexible nephroscopy was also performed. The patient was considered stone free when all removable stones had been taken out and he or she was stone free by 30 days post-treatment. Bleeding severity was based on the judgment of the treating physician and blood transfusion given according to local practice guidelines.
Data analysis
Patients were classified into two main groups: Those with staghorn stones and those with nonstaghorn stones. The data were analyzed to compare differences between the two groups. In terms of preoperative, intraoperative, and postoperative parameters, the variables of interest were: The global distribution and demography of the presence of staghorn stones, patient characteristics, access method, puncture frequency and outcomes, including bleeding rates, operative time, and duration of hospital stay.
SPSS version 16.0 was used to analyze the data. All data are descriptive and based on frequencies. Continuous variable were analyzed using parametric tests (independent Student t test) and nonparametric tests (Mann-Whitney U test). Categorical variables were compared using the Pearson chi-square test. Statistical significance was set at P<0.05.
Results
A total of 5803 patients were included in the database after treatment during the study period November 2007 and December 2009. Of these, 468 patients were excluded from the analysis because information on their staghorn stone status was unavailable. Of the remaining 5335 patients, 1466 (27.5%) had staghorn stones and 3869 (72.5%) had nonstaghorn stones.
Study center variation
The level of staghorn stones varied between continents. In the study centers in Asia, Australia, and Europe, 29.5%, 22.2%, and 25.5% of patients presented with staghorn stones, respectively. In North American centers (average of United States, Canada, and Mexico), 38.8% of patients presented with staghorn stones, while in South America, the proportion of patients with staghorn stones was 12.7%. Figure 1 illustrates the relative proportions of patients presenting with staghorn stones in each of the participating countries. The center in Thailand had the highest proportion of patients with nephrolithiasis who presented with staghorn stones at approximately 67%. The centers in Portugal, China, The Netherlands, Israel, and United States reported that >40% of patients had staghorn stones. The lowest proportion of staghorn stones reported was in Argentina at 13%.
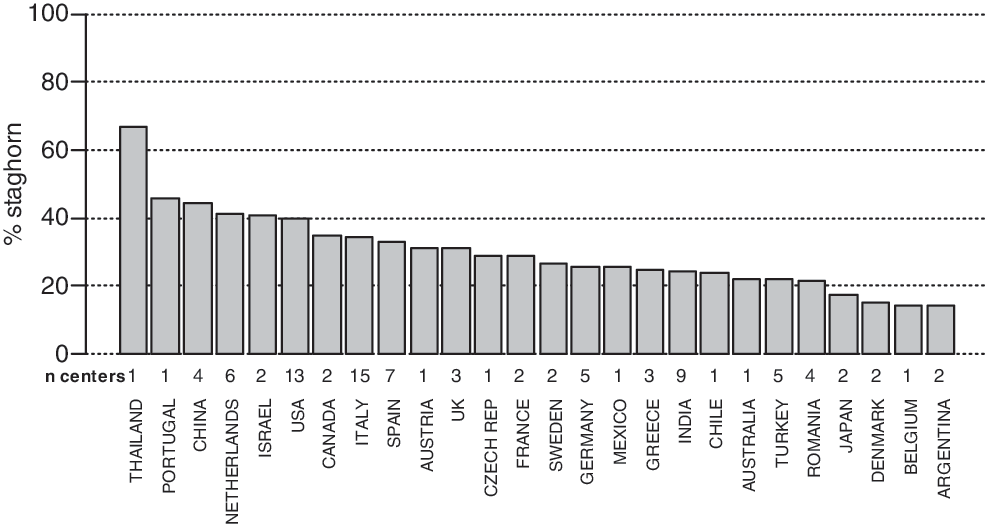
Proportions of patients who presented with staghorn stones in participating countries.
Patient characteristics
Preoperative patient characteristics presented in relation to staghorn stone status are shown in Table 1. The median age in both groups was similar, and a significantly greater proportion of women had staghorn stones (P<0.0001). Regarding history of procedures, these were broadly similar between groups. A slightly higher proportion of patients with staghorn stones than with nonstaghorn stones had undergone previous PCNL and nephrostomy insertion while slightly fewer had previous pyelolithotomy or ureteroscopy. Of patients with staghorn stones, however, 16.8% had undergone SWL compared with 22.6% of nonstaghorn patients, and preoperative urine cultures were positive in a greater proportion of patients with staghorn than nonstaghorn stones (23.4% vs 13.1%).
SWL=shockwave lithotripsy; PCNL=percutaneous nephrolithotomy; URS=ureteroscopy.
Access method and puncture frequency
The access methods used and the proportion of punctures at various renal sites are shown in Table 2. The ratio of balloon to metallic (telescopic/serial) dilation was 46.1:53.9 in patients with staghorn stones compared with 39.3:60.7 in those with nonstaghorn stones. Generally, patients in both groups had a greater proportion of lower than middle or upper kidney punctures; however, 16.9% of patients with staghorn stones underwent multiple punctures to attain stone removal compared with 5.0% of patients with nonstaghorn stones (P<0.0001). There was also a significant difference between puncture sites in patients with and without staghorn stones (P<0.0001), suggesting that the presence of staghorn stones may have an influence on the position of renal puncture in PCNL.
Outcomes
The postoperative outcome variables of main interest are shown in Table 3. Complications such as postoperative fever, bleeding and the need for blood transfusion, and perforation were more common in patients with staghorn compared with nonstaghorn stones. More patients in the staghorn group needed postoperative nephrostomy insertion, and median operative time and duration of hospital stay were also longer in the staghorn group. During follow-up, a significantly smaller proportion of patients with staghorn stones were stone free compared with nonstaghorn patients (56.9% vs 82.5%; P<0.0001). Similar results were reported for the two groups of patients with regard to percentage of failed procedures and the occurrence of hydrothorax.
Discussion
Over the course of 1 year, a total of 5803 patients were entered into the CROES PCNL database. As part of an ongoing series of CROES PCNL Global Study analyses, herein the outcomes in patients undergoing PCNL for the removal of staghorn and nonstaghorn stones are compared. A calculus is considered a staghorn stone when present in two or more calices. To confirm if this definition was applied by all participating centers, (selected) images should have been centrally reviewed. The absence of the central radiologic confirmation of staghorn calculi can be considered one of the limitations of the study. Because the study sites were eligible to participate in the study if they were considered by the Steering Committee to have high expertise in this medical field, however, we may safely assume that the proper definition of a staghorn stone was applied in the vast majority of patients treated.
An overall staghorn stone frequency of 27.5% was reported. North America, however, reported a rate of 39%, well in excess of this overall frequency. One possible reason for this may be the existence in the United States of centers that are dedicated to treatment of small stones using SWL monotherapy. Therefore, as sites only performing PCNL alone or in combination with SWL were recruited to this study, this could account for the observation. At the other extreme, in South America, where the proportion of staghorn stones was 13%, the underlying rationale for this observation remains unknown. When considering the proportion of staghorn stones by country, however, Argentina contributed largely to the South American population recruited to the study, and the low level of staghorn stones seen may be a feature of this population rather than of the population of South America as a whole.
The center in Thailand reported the highest prevalence of staghorn calculi. Interestingly, a publication on the incidence of kidney stones in South Korea reported that just 1.6% of patients audited had staghorn calculi. 15 Intriguingly, a report that indicated an incidence of staghorn calculi of 24% in Hmong people from the highlands of Laos who migrated to Minnesota 16 suggests that within Southeast Asia, there may be a great variation in the incidence of staghorn stones. Of note, in both Southeast Asia reports, a common shared feature was stone composition; the staghorn stones were uric acid stones. 15,16
A significantly smaller proportion of patients with staghorn stones (56.9%) were classed as stone free compared with nonstaghorn patients (82.5%) in the present study. The determination of stone-free status was made by individual institutions and, as such, we cannot eliminate the possibility of variance in the criteria applied. Nevertheless, this should not have affected the ratio between stone-free rates in staghorn vs nonstaghorn patients within an individual institution.
In terms of previous procedures, patient characteristics were broadly similar between the staghorn and nonstaghorn groups. As expected, fewer patients with staghorn stones had undergone SWL before PCNL. SWL monotherapy currently has a limited role in the treatment of patients with complex renal calculi. 17 PCNL in patients with staghorn calculi is recommended as the first-line therapy, which may be followed-up with SWL and further PCNL to ensure complete stone removal. 17,18 Of late, the final PCNL procedure appears to have been abandoned in favor of spontaneous passage of stone fragments, which may explain the suboptimal stone-free rates seen in some series. 17 Previous SWL in CROES patients with staghorn and nonstaghorn stones may have been undertaken in an attempt to clear kidneys before stones enlarged, and certainly indicates a possible symptomatic history of nephrolithiasis.
A greater proportion of patients with than without staghorn stones had bacteriologically positive preoperative urine cultures. Staghorn renal calculi are commonly, though not always, infection induced. While the role of nonurease bacteria in the pathogenesis of other types of stones is unclear, it is known that 75% of staghorn stones are composed of struvite and are induced and infected by urease-producing bacteria. 7 Infected staghorn calculi can grow rapidly, and patients often present with recurrent symptoms of cystitis. 19
Of the 96 centers recruited to the CROES PCNL Global Study, 28 used balloon dilators only and 25 centers used only metallic (telescopic/serial dilators); the remaining centers (predominantly European) used both types of dilator. 13 Overall, telescopic/serial dilation was the predominant method used in Asia (1271/1342; 94.7%) and South America (337/344; 98%), and balloon dilation was the most popular method in North America (650/787; 82.6%). Thus, it appears that North America, which contributed 580 patients to the overall study and which reported a 39% rate of staghorn stones, used mainly balloon dilation, which may influence the access ratios. In addition, in South America, which reported some of the lowest proportions of staghorn stones, telescopic/serial dilation was almost exclusively used, which may also influence the access ratio.
The comparison of puncture sites in staghorn and nonstaghorn patients was similar between groups, with lower pole puncture being more commonly used in both groups. For staghorn stones, upper pole entry with the patient in the prone position usually provides access to the majority of the collecting system and can facilitate complete stone removal. 17 While the advantages of PCNL in the supine and modified supine positions have been supported by clinical findings, however, upper pole caliceal puncture becomes more challenging if undertaken with the patient in the supine rather than the prone position. 20 –22 Therefore, most punctures are performed in the lower pole and interpolar calices with supine patients and may explain the observations of this study. 22 Positioning the patient supine does have some limitations, and although it is not yet clear which operating procedure is optimal, use of a modified supine position with or without simultaneous ureteroscopy may be the procedure of choice used in the future. 20,22
Although feasible, access to all renal calices through one percutaneous tract remains difficult because of the peculiarities of the renal collecting system. 2 Single tract approaches are also hampered by reduced vision caused by bleeding, making the use of flexile instruments challenging. 23 The fact that multiple punctures were noted more frequently in staghorn patients than nonstaghorn patients in this study was not unexpected. The argument for multiple rather than single tract PCNL (with or without flexible instrumentation) for the complete clearance of renal stones is ongoing, however. 24 One argument against use of a multitract approach is the potential for increased bleeding as demonstrated in a study by Akman and associates 23 but contradicted in other studies. 8,24 In general, however, PCNL necessitating multiple tracts appears effective and should be used in place of excessive levels of manipulation through a single tract. 23 –25 As flexibile nephroscopy becomes more widely used, together with improvements in techniques that debulk the stone, the need for additional tracts may be alleviated in future. 17
The higher rate of postoperative fever seen in staghorn patients than in nonstaghorn patients may reflect the higher rate of preoperative positive culture also noted in this group and discussed previously. Antibacterial prophylaxis is routinely administered in urologic procedures, although it has been reported that there is little evidence of its affording benefit. 26 Marriappan and colleagues, 27 however, reported the successful use of extended preoperative prophylaxis in PCNL patients with dilated pelvicaliceal systems. 27 Increasingly, physicians are using extended prophylaxis in such “at risk” patients, a practice that may be reflected to some extent in this study.
Bleeding during and after PCNL continues to be a cause of patient morbidity. In the current study, bleeding and the necessity for blood transfusion was seen to a greater extent in patients with staghorn than nonstaghorn stones. Surgical bleeding is the main cause of blood loss in PCNL and can be minimized by optimizing renal access, tract dilation, and renal manipulation while minimizing technical error—practices that apply to PCNL in both staghorn and nonstaghorn patients. 28 That staghorn stones are generally larger and more awkwardly sited than nonstaghorn stones makes placement of the dilator and stone manipulation and removal more difficult, possibly contributing to the increased bleeding noted in this study. Removing large stones through the working sheath can damage it, and its subsequent removal can cause profuse bleeding. 29 Awareness of stone size during extraction, minimal nephroscope angulation, and the exertion of minimal torque forces on the kidney during PCNL can all aid in reducing bleeding and, thus, the need for transfusion. 28 The increased perforation of the collecting system rate noted in the staghorn patients would also contribute to the greater bleeding and transfusion reported in this group.
Two retrospective studies identified risk factors for post-PCNL hemorrhage. Stone size significantly predicted the occurrence of bleeding in patients undergoing PCNL for symptomatic stone disease in the first study; upper caliceal puncture, solitary kidney, multiple punctures, staghorn stones, and inexperienced surgeon were the risk factors for hemorrhage post-PCNL in the second. 30,31 As PNCL is the most complicated stone treatment to teach, with urologists needing to perform at least 100 procedures to be considered excellent, 32 the importance of the risk associated with the inexperienced surgeon in PCNL is further acknowledged.
Given that in the current study the median operative time and hospital stay were longer in staghorn than nonstaghorn patients while the stone-free rate was lower, physicians may wonder whether the treatment practices used in the management of staghorn calices are optimal. Although open surgery maintains a mandatory role in selected cases, the advantages of PCNL, including shorter hospital stay, lower morbidity, and shorter operative time, 33 outweigh any small benefit in stone-free rate gained through open surgery, such as reduced cost, 34 leaving it the technique of choice in staghorn stone removal. 35
In the future, it is anticipated that further developments in at least three major areas where PCNL has undergone recent changes in technique—patient positioning, improved intracorporal lithotripsy, and postoperative nephrostomy tube management—will increase stone-free outcomes and reduce postoperative complications and perioperative patient morbidity, thereby making PCNL an even more effective first-choice therapy in the management of staghorn nephrolithiasis. 20
Footnotes
Acknowledgment
The Global CROES PNCL study was supported by an unrestricted educational grant from Olympus.
Disclosure Statement
No competing financial interests exist.