
Abstract
Purpose:
To design a training phantom to allow trainees to demonstrate and practice the key steps of a laparoscopic nephrectomy, while demonstrating the anatomical landmarks, together with correct instrumentation and safe ergonomic layout.
Materials and Methods:
Calves, prepared according to the strict standards of the meat industry, were purchased from a local abattoir. The skinned torso of a 30-kg calf was prepared by opening the abdomen and removing most of the ribs and the pelvis to create a larger working space. The small intestine and the majority of the large intestine were removed, leaving 30 cm of ascending colon, the liver, and spleen as internal landmarks and placed inside a standard laparoscopic abdominal trainer. This model was then used as part of a structured training course.
Results:
From April 2005 to April 2010, 104 urologists have worked on this phantom. Evaluation forms were completed by these participants, and analysis of the feedback shows all attendees found the model to be very realistic in terms of anatomical conditions, tissue color and consistency, and organ tactility, compared with human nephrectomy (average score of 4.8 on a Likert scale of 1 (unrealistic/poor) to 5 (realistic/useful)). Participants found the model useful for developing dissection techniques, electrosurgery, coagulation, and suturing skills.
Conclusion:
This model can be easily established and is valuable as part of a multimodal training program for laparoscopy.
Introduction
These findings, combined with increased patient demand, have encouraged the development of laparoscopic surgery within urology. As well as laparoscopic radical nephrectomy for RCC, laparoscopic nephroureterectomy for upper-tract Urothelial-cell carcinoma and laparoscopic simple nephrectomy for nonfunctioning kidneys are becoming commonplace. A long and steep learning curve, however, is recognized as a limiting factor in the incorporation of laparoscopy into practice. 12
Laparoscopic surgery is technically demanding, not without inherent risk of complication for the patient. 13 Laparoscopy is an evolving practice, without the tactile and three-dimensional feedback of open surgery. Also, within urologic practice, there is a lack of simple laparoscopic procedures, such as appendicectomy and cholecystectomy in general surgery, which may hinder the stepwise development of training. Furthermore, the European Working Time Regulations 14 have resulted in decreased access to theatre and time available for training. 15
Compounding all of these factors is the ethical responsibility to decrease medical errors. As a result, unaugmented standard surgical apprenticeship is felt to be insufficient in the development of laparoscopic skills, and other training techniques are needed.
Some trainees feel there is limited access to laparoscopic training. 12 A training pathway for the development of laparoscopic skills has been proposed. 16 This would commence with basic skills courses, followed by simulator training and then assisting in procedures. Thereafter, recommended training includes attendance at an advanced skills course, training in animal models, and then mentored cases progressing to independent practice. Despite this suggestion, it is accepted that training throughout Europe is varied. Nonetheless, it is felt that each method of training has an important role in the development of laparoscopic competency. 12
Despite the accepted importance of structured training in a laboratory environment, creation of a realistic training exercise for laparoscopic nephrectomy is a significant challenge. A model currently used in training of laparoscopic nephrectomy is the (25–30 kg) porcine model. This is used in live animal laboratory courses abroad and, as such, was initially adapted for our dry laboratory course. Although the porcine kidney is accessible with similar vasculature, it is shorter with a thinner ureter 17 and has reduced perinephric fat compared with the human kidney. It was therefore thought that a porcine nephrectomy was very simple and did not provide the sufficient degree of difficulty to allow skill development and practice of laparoscopic nephrectomy. We therefore aimed to find an alternative model, using accessible animal tissue.
This study describes the design of a training phantom that allows trainees to demonstrate and practice the key steps of a laparoscopic nephrectomy. In addition, this model allows the demonstration of the anatomic landmarks for this procedure together with correct instrumentation and safe ergonomic layout. This model is currently used in a structured urologic laparoscopy training course.
Materials and Methods
Design of the program and delivery of the course
Since 2005, in close collaboration with the British Association of Urological Surgeons (BAUS) and endorsed by BAUS, the BAUS Section of Endourology laparoscopic training course has been developed and run. The course consists of didactic and practical sessions with emphasis on hands-on practice using simulated models in a well-established training laboratory. Faculties are drawn from a pool of senior urological consultant surgeons who are experts in laparoscopic surgery. There are 20 delegates, with a ratio of participants to tutors of 4:1. The aim of the course is to develop key laparoscopic skills and prepare the trainee for progression onto structured, mentored training within the theater setting.
The course is held for 2 days and is divided into three major teaching modules. Day 1 is for rehearsal and acquisition of key skills in laparoscopic surgery. Module 1 contains essential laparoscopic skills including the introduction to laparoscopic equipment and instruments, access techniques, insufflation, camera exercises, ergonomics in minimal access surgery (MAS), tissue dissection and approximation techniques, electrosurgical devices, and tissue extraction. Laparoscopic suturing skills are introduced and practiced.
Day 2 begins with a practical session to reiterate the skills practiced the previous day. Thereafter, Module 2 covers the theoretical basis of laparoscopic nephrectomy, with discussion of the pathophysiology of disease, diagnosis, indication and contraindications for surgery, and the principles of preoperative and postoperative care. The prevention and treatment of complications and relative advantages and disadvantages of both open and MAS techniques are also reviewed. This discussion is augmented by a video demonstration of laparoscopic nephrectomy performed by the expert surgeons.
Module 3, which is the majority of the second day, consists of the introduction of the calf model and essential steps involved in the laparoscopic nephrectomy. Each participant has the opportunity to perform either a right or left laparoscopic nephrectomy using the model, which is mounted inside the laparoscopic trainer, for the necessary time. The two trainees spend approximately 6 hours in total working with the laparoscopic bovine model. Close supervision is provided by the expert surgeon tutor during the course, and immediate feedback and guidance are provided.
Design and construction of the bovine model
With the purpose of identifying a better model for trainees to rehearse this commonly performed laparoscopic procedure, a calf was dissected and assessed by a consultant urologic surgeon who had experience of using the porcine model for training of laparoscopic nephrectomy. As a result, taking into consideration the anatomical proportions of the calf and the size of the laparoscopic box trainer, a 30-kg calf was used to construct the model.
A supply of calves was secured from the local abattoir. These are the calves that would normally be used for human consumption, and as such are strictly inspected to ensure disease control before culling. The abattoir is fully registered under the standard regulations stipulated by the meat industry and follows strict ethical guidelines. These calves are purchased at the current market value, within the meat industry, of £80 ($130) each.
A technician, trained by the pioneering surgeon, prepared the skinned torso (diaphragm to pelvis) of a 30-kg calf by opening the abdomen and removing most of the ribs to create a larger working space. The small intestine was removed as carefully as possible without damaging the remaining peritoneum. The liver and spleen were left in situ, providing landmarks for orientation inside the trainer. The majority of the large intestine was also removed, leaving 30 cm of ascending colon, which was used as a third internal landmark. The pelvis was removed to allow the specimen to fit inside a standard laparoscopic abdominal trainer (Fig. 1). The phantom is placed inside the box, tilted, and secured with the left edge uppermost for the left nephrectomy. For a right nephrectomy, the angle of mounting the specimen is adapted to provide the right edge uppermost.
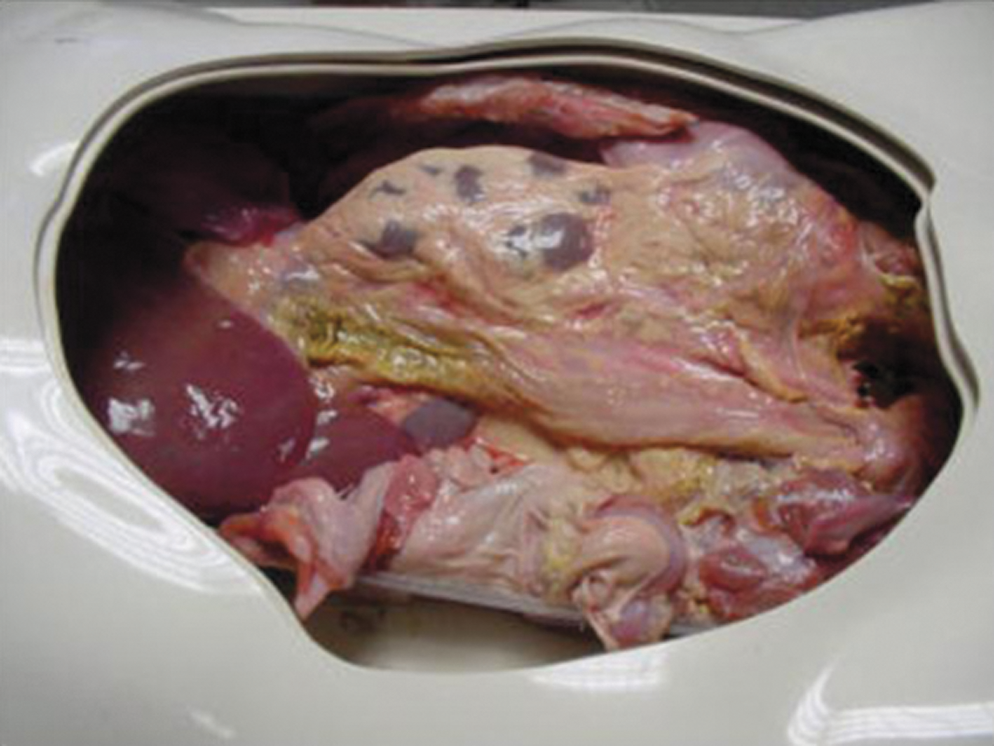
Phantom shown inside laparoscopic trainer.
Rehearsal of laparoscopic nephrectomy on the calf model
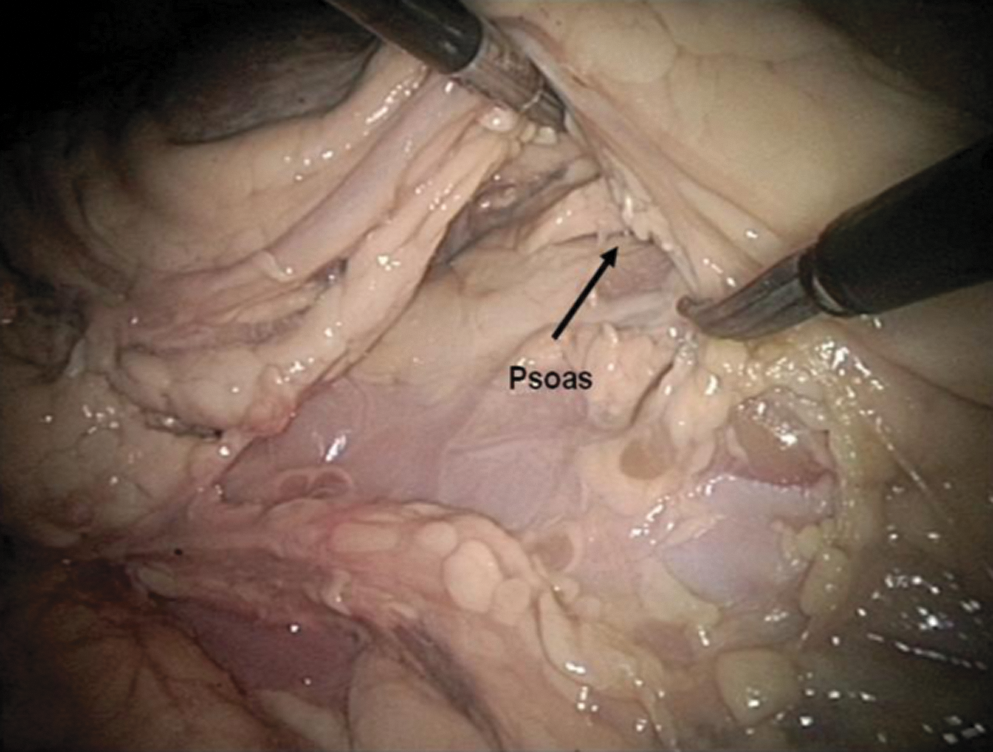
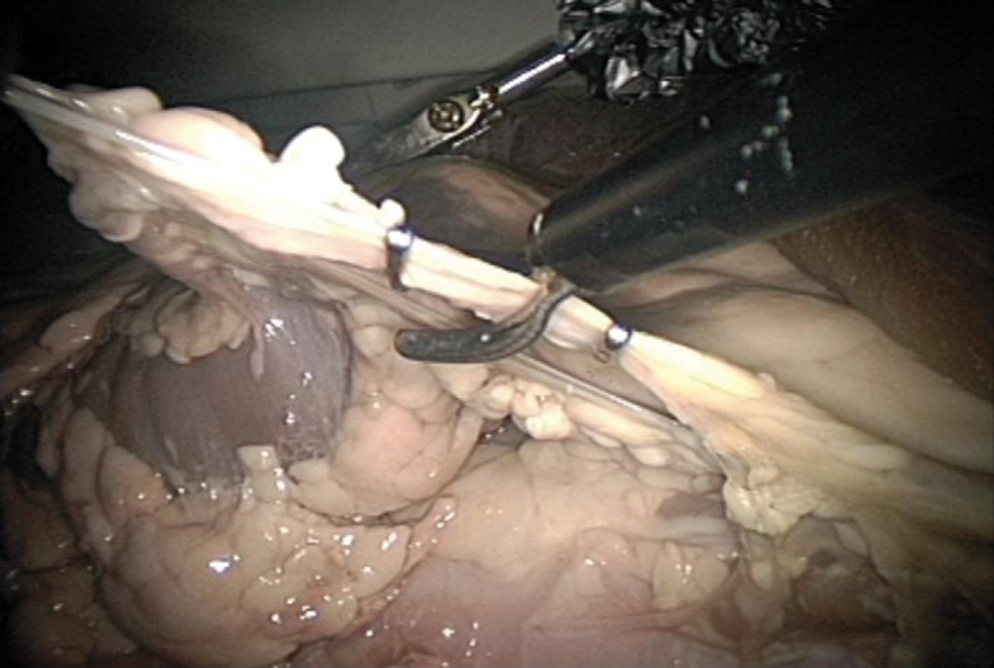
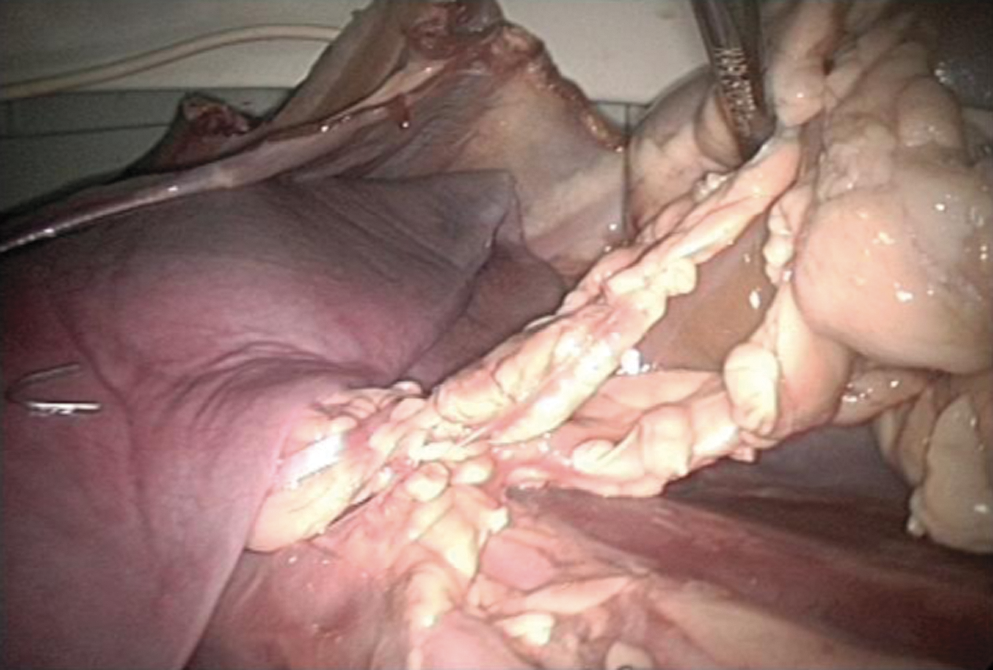
The calf model was used to teach the principles of laparoscopic nephrectomy in a stepwise approach (Fig. 2). During nephrectomy, the importance of proper orientation and identification of anatomic landmarks was stressed (Fig. 3). The peritoneum was opened medial to the kidney to identify the ureter (Fig. 4). The ureter was mobilized and retracted to allow dissection and elevation of the lower pole (Fig. 5). Dissection was continued to allow identification of the hilum (Fig. 6), with subsequent identification and skeletalization of the renal vein and artery (Fig. 7). The artery was then clipped and divided, followed by the vein (Figs. 8, 9). The ureter was then clipped and divided (Fig. 10). The upper pole and lateral aspect of the kidney was mobilized (Fig. 11) before the specimen was entrapped and delivered (Fig. 12).

Trainees using model.

Orientation.
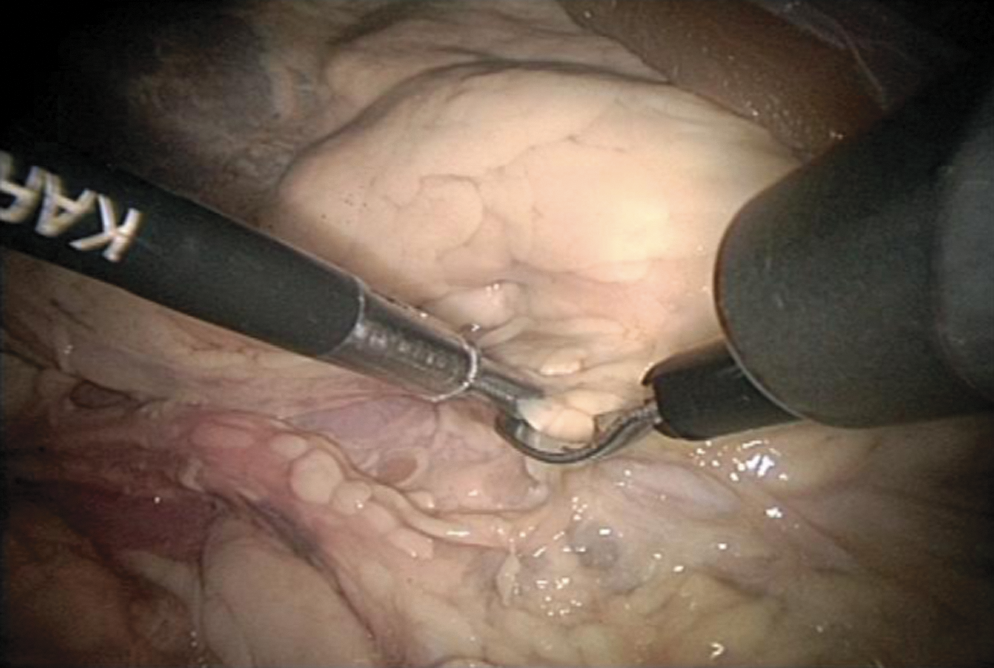
Dissection of peritoneum.
Elevation of ureter and lower pole.

Continued dissection to the hilum.

Identification and skeletonization of vessels.
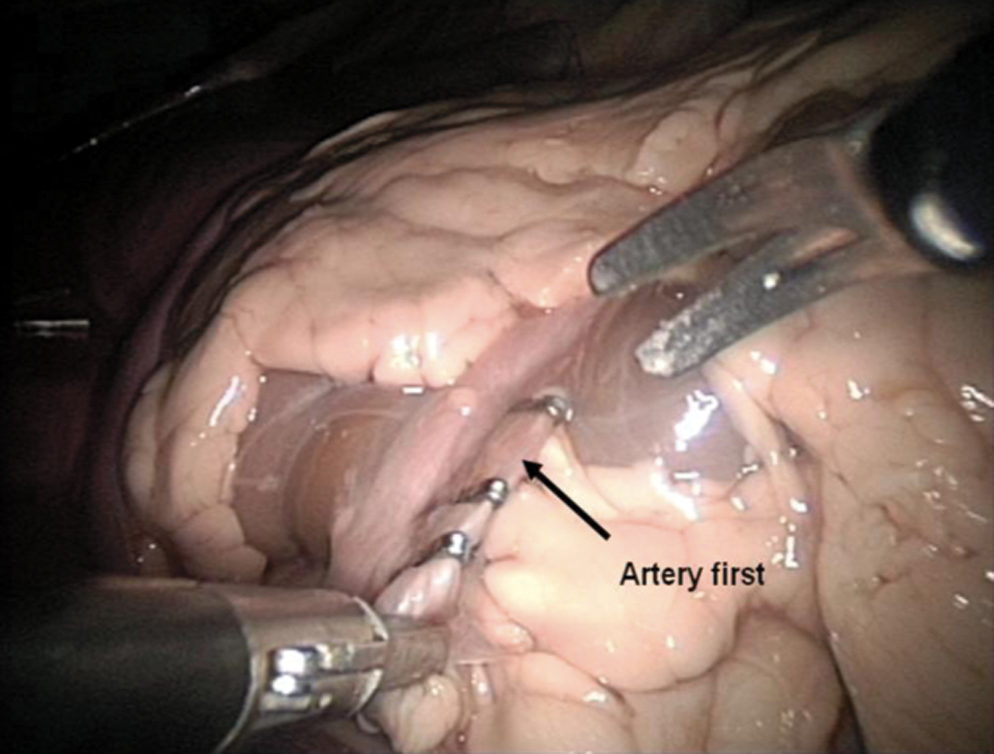
Clip and divide the artery first.
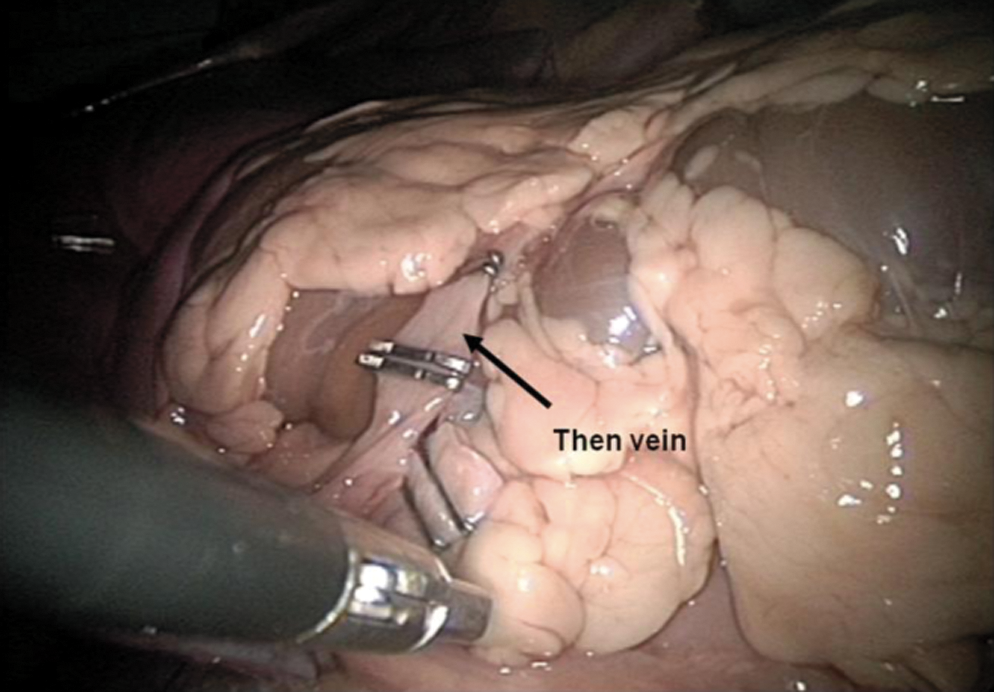
Clip and divide the vein.
Mobilize, clip and divide ureter.
Mobilize upper pole.

Specimen entrapment.
Data collection
At the end of the course, all attendees self-completed a structured, anonymized written questionnaire to assess the validity of the model and course as a whole for training. Data were collected using a Likert scale (1=strongly disagree; 2=disagree; 3=neither agree nor disagree; 4=agree; 5=strongly agree) on a standardized anonymous questionnaire. The feedback on the calf model for anatomic condition of the calf model, quality of the tissue and organ colour, quality of organ consistency, and operative tactility during the dissection was given by the delegates. Evaluation forms were completed by participants and analysis of the feedback was conducted.
Results
Over the last 6 years, from April 2005 to April 2010, 104 urologists have worked on this phantom. These participants included 92 specialist registrars (SpRs) and 12 consultant surgeons. All of the SpRs who attended were in years 2 to 4 of their training and had, as a minimum, assisted in laparoscopic nephrectomies. Of the consultants who attended the course, they were not yet independent in laparoscopic nephrectomy but had had some limited experience. Evaluation forms were completed by participants, and analysis of the feedback shows that the participants awarded the training phantom an overall mean score of 4.8 on a scale of 1 (unrealistic/poor) to 5 (realistic/useful) (Table 1).
All of the specific comments given by the urology trainees about the model were positive; for example. “excellent to get experience in nephrectomy” and “excellent practical opportunities.” Among the 104 participants, 96% of them thought that their laparoscopic skills had been improved significantly—in particular, the ability and knowledge to interpret crucial anatomic structures and their surroundings in laparoscopic view. They commented that there is a significant difference between operating as a main surgeon and as an assistant in laparoscopic nephrectomy, and this model helped bridge the gap. All of them agreed that the calf model was extremely useful for them to practice tissue handling skills, and they had made significant improvement.
Of the consultant subgroup, 8 of the 12 surgeons expressed that they would start performing this procedure with some initial help from experienced experts after attending the course. No negative feedback points were raised in any of the evaluation forms regarding the model.
Discussion
The British Association of Urological Surgeons recommends that trainee urologists learn best through a combination of laboratory based courses, as well as clinical coaching. 18 Laboratory training in laparoscopic skills is a sensible first step, and a number of techniques have been described including box trainers, virtual reality simulators, live animal models, and cadaveric models. The bovine model described here provides a novel, realistic training tool for laparoscopic nephrectomy teaching.
Each model has its own merits as well as limitations. Cadaveric models obviously provide anatomic specimens second to none. Preparation with formaldehyde, however, often degrades tactile feedback. Live animal models, such as porcine, canine, and bovine specimens, offer similar anatomic models to humans. They allow development of complex skills and completion of whole procedures with similar hemostatic qualities. Operating on live animals provides a similar overall experience to that of humans. Unfortunately, these models are expensive, necessitating appropriate preoperative and postoperative care with the necessary skills and expertise for anesthesia, making widespread use difficult.
The cost of such models has been said to reach $1460 (£900). 19 This is far greater than those costs incurred when constructing our model. The animal tissue can be purchased at a cost of £80 per unit, with little extra additional overheads after initial purchase of the box trainer. Our box trainers were purchased more than 10 years ago at a cost of £900 each and are used in a number of courses, both urological and others, throughout each year; thus, they prove very economical.
There are also ethical concerns over the use of such live animal models, and in many countries, including the UK, they are illegal. The animal tissue used for our model is handled ethically in accordance with those guidelines accepted by the meat industry.
Box trainers and virtual reality simulators are in more widespread use. They are equally effective in the attainment of laparoscopic skills. 20 Virtual reality simulators can be used for simple skill tasks as well as simulation of whole procedures with complications. They can be used to assess progress without the need for direct trainer input. They can be expensive, however. Simple box trainers are easily accessible and relatively cheap. They are reproducible and allow the development of instrument familiarity and basic hand-eye coordination. Box trainers, however, do not allow the development of more complex laparoscopic skills. Animal tissue can be incorporated into box trainers; this is thought to be a compromise between the simple box trainer and the live animal models. It allows for the development of more complex skills, such as tissue handling, dissection, and suturing, without the same ethical concerns, cost, and need for general anesthesia.
Porcine kidney is often used in these box trainers, because it is easily accessible and similar to that of a human with comparable vasculature. Other than in length, the porcine kidney is smaller than the human kidney, with a smaller thinner ureter. 17 As a result of the previously mentioned anatomical differences. we believe that porcine nephrectomy is artificially simple. There have been no studies directly comparing the calf kidney to the human or porcine kidney. During assessment of the calf for use as a model by our team, however, it was discovered that the anatomic conditions, quality of tissue, and operative tactility of the calf tissue was much better than that of the porcine model and more closely approximated human tissue. In particular, the perinephric tissue allows for dissection that more closely resembles the human nephrectomy than that offered by the porcine model. As such we believe it to be a superior model for training in laparoscopic nephrectomy.
Our course attendees, although not experienced laparoscopic surgeons, had all had some exposure to laparoscopic nephrectomy. As such, we think they had sufficient experience to compare this model with human laparoscopic nephrectomy. Questionnaire assessment of the quality of the calf model revealed that all attendees found the model to be very realistic in terms of anatomical conditions, tissue color and consistency, and organ tactility, compared with human nephrectomy. They found it useful for developing dissection techniques, electrosurgery, coagulation, and suturing skills. We do, however, accept that this model could be further validated by assessment by experienced laparoscopists, as well as a blinded comparison with porcine models, to prove superiority. Further testing could also be conducted to confirm whether the believed development of skills using this model was apparent objectively and whether these skills are transferable.
This course is one of only two endorsed by BAUS. There are, however, a number of other laparoscopic courses run throughout the UK. Attendance at any of these is optional but encouraged during training. Despite their slightly different methods, they all aim to prepare the trainee for clinical training in laparoscopic nephrectomy. Most SpRs attend during their intermediate training years. At the last manpower count, there were 248 SpRs in total throughout the UK, 21 and only 20 trainees can be taught on this course each year, on a “first-come, first served” basis. This model could be easily adopted by other units. The suggestion has also been made that this model could be further developed for robotic training, which should follow the same principle of safe structured training before patient contact.
Conclusion
The bovine laparoscopic nephrectomy model provides an anatomically realistic model that not only has comparable anatomic qualities for learning the key steps in laparoscopic radical nephrectomy but also provides opportunity for the development of advanced laparoscopic skills. This model can be used and is valuable as part of a multimodal training program for laparoscopy.
Footnotes
Disclosure Statement
No competing financial interests exist.