
Abstract
Purpose:
We report a simple figure-of-eight tension adjustable suture to ligate the vascular pedicle (VP) during robot-assisted radical prostatectomy (RARP).
Materials and Methods:
During nerve-sparing RARP, after the rectum has been mobilized, the VP is isolated and prepared for transection. Previous reports describe placing of hemostatic clips (metallic or Hem-o-lok™) or laparoscopic bulldog clamps (30 mm) to control and oversew the VP; both techniques are quite assistant dependent. We present a bulldog clamp alternative by placing a figure-of-eight fashion, a 6-cm 3-0 poliglecaprone on an SH needle with a small loop tied in the suture end. After the needle has been placed through the VP, it is then threaded through the preformed loop and then a small Hem-o-lok clip is placed and cinched down to occlude the blood vessels. Next, the VPs are transected. The clip can be further cinched, mimicking the technique used in partial nephrectomy, to control bleeding when encountered. Data were collected prospectively to demonstrate safety.
Results:
We report on 74 men totaling 143 VPs using this new technique. The average operative time was reduced by 15 minutes compared with using bulldog clamps. In the initial 10 cases (20 attempts), inadvertent transection of the suture occurred three times. In these three cases, hemostasis was (easily) controlled with additional sutures.
Conclusions:
The pedicle stitch technique offers an assistant independent alternative for a simple and precise athermal means to control the VP.
Introduction
Based on the work of Ong and associates 2 and others, there has been much evidence that even with excellent preservation of adequate nerve volume, the use of thermal energy on the VPs and NVBs is injurious. In 2005. two groups described athermal techniques using bulldog clamps to control the VP based on experience with partial nephrectomy. 3 –5 A benefit of this technique is that once the bulldog is placed, the VP is sharply transected with essentially no traction issues. A popular alternative has been vascular clips. Placing vascular clips is athermal, but significant stretching and traction of tissue is needed to make space for the clips to be precisely placed.
Conceptually, one could accomplish hemostatic control of the VP with a suture, bypassing the need for the bulldog and subsequent suture ligatures. In practice, however, after placing the initial suture and as we proceeded to transect the VP, we encountered troublesome bleeding. We learned that the suture ligation was not adequately tight enough after transecting the VP. After a handful of cases, this approach was abandoned because of unacceptably poor hemostasis.
The suture ligation concept, however, resurfaced as a consequence of robot-assisted partial nephrectomy techniques. Recently, surgeons have introduced a hemostatic stitch along the cut edge after partial nephrectomy. 6 The central point is that a Hem-o-lok™ clip can be cinched tighter—multiple times, if needed. Hence, we introduce a technique in which the VP suture, placed for ligation, can be “recinched” during and after transecting the VP, as needed.
Materials and Methods
Patient population
One hundred and forty-eight consecutive cases were performed by a single surgeon (TEA), either by the new tension adjustable (TA) suture ligation (n=74) or by previously described bulldog methods (n=74). 3,4 Men were selected for excision of one or both NVBs if they had extensive involvement noted on biopsy cores (>50% by volume estimate and/or Gleason score >4+3), obvious palpable disease (with biopsy confirmation), inadequate sexual function (Sexual Health Inventory for Men <10), or patient preference; otherwise, bilateral nerve sparing was performed.
Standard clinical characteristics were recorded prospectively and entered into an electronic database. In particular, we focused on estimated blood loss (EBL), change in hemoglobin value, intraoperative and postoperative complications, and operative time. We also recorded in our electronic database whether additional sutures were needed to control the VP or if pedicle suture application failed; these data were also analyzed. A postoperative complication was defined as the need for emergent return to the operating room, prolonged hospitalization greater than 48 hours, or the need for reintervention or hospitalization within 30 days of surgery (Clavien classifications III–V). Operative complications attributable to the technique, such as bleeding, hematuria, pelvic hematoma, or abscess, etc., were also noted. All statistical comparisons were performed with the SAS 9.1 statistical package, with significance defined The as P≤0.05.
Operative technique
The Denonvillers fascia is incised and the rectum fully mobilized off the prostate. This delineates the prostatic VPs. Previously, laparoscopic bulldog clamps (30 mm) were placed on the VPs approximately 1 cm from the prostate. At this point, instead of applying a bulldog clamp, a pedicle stitch is placed in the same position. The suture is a 3-0 poliglecaprone on an SH needle with a small loop tied in the suture end (Fig. 1). The pedicle stitch is thrown approximately 5 to 8 mm from the base of the prostate from medial to lateral through the pedicle about 5 to 7 mm above the perirectal fat. It is then passed a second time at middepth (looking anterior to posterior) through the pedicle in a figure-of-eight fashion. The needle is then passed through the preformed loop in the end creating a slip-knot formation. Additional traction on the suture end will occlude the vascular pedicle just enough to stop venous and arterial bleeding. This figure-of-eight technique allows the suture to occlude any deep or superficial vessels that course through the VP as well (Figs. 2 and 3). A small Hem-o-lok clip is then applied, and this is used to cinch down, forming a TA suture tourniquet around the VP. (Supplementary videos depicting the placement of the tension adjustable pedicle stitches and transection of the vascular pedicles during robot-assisted, nerve-sparing radical prostatectomy are available at

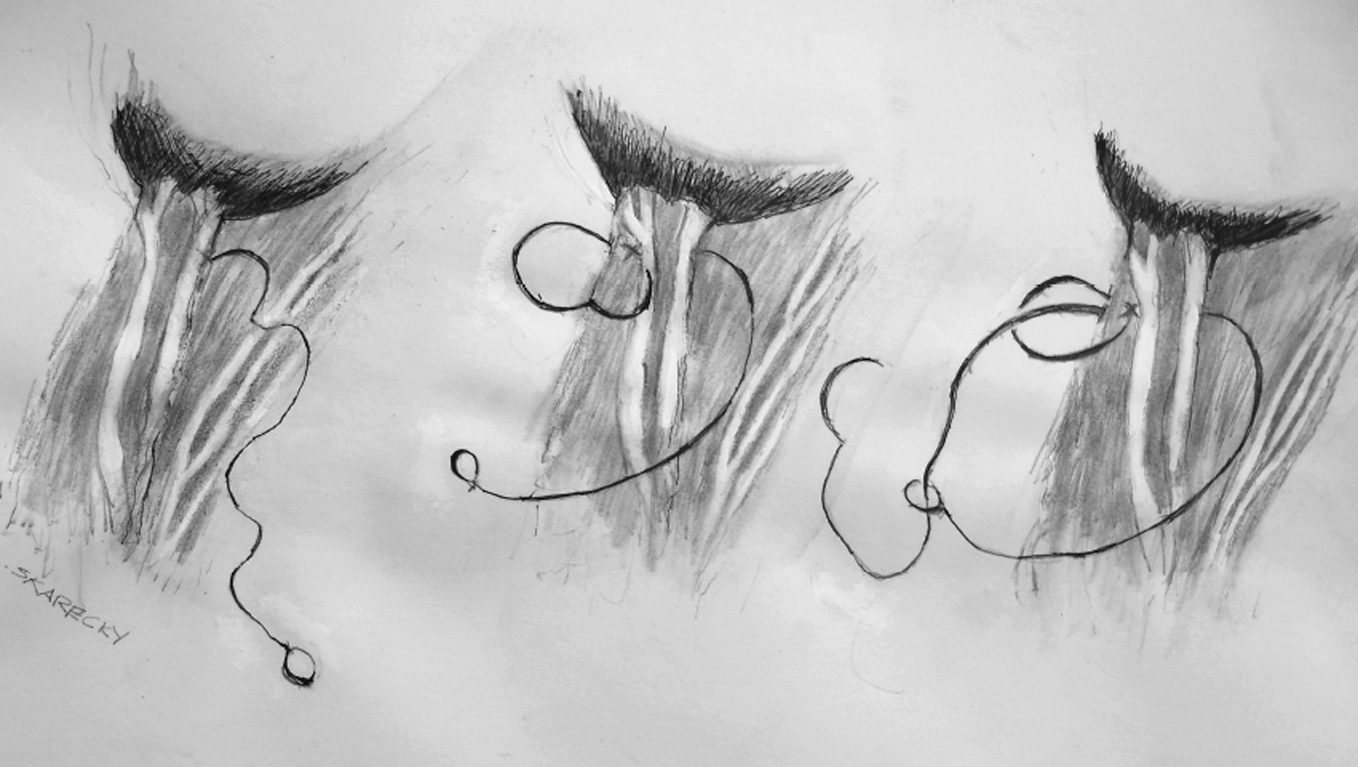
A distal loop is first created. The pedicle stitch is thrown through the vascular pedicle in a figure-of-eight fashion, then passed through the distal loop to create a tourniquet around the pedicle.
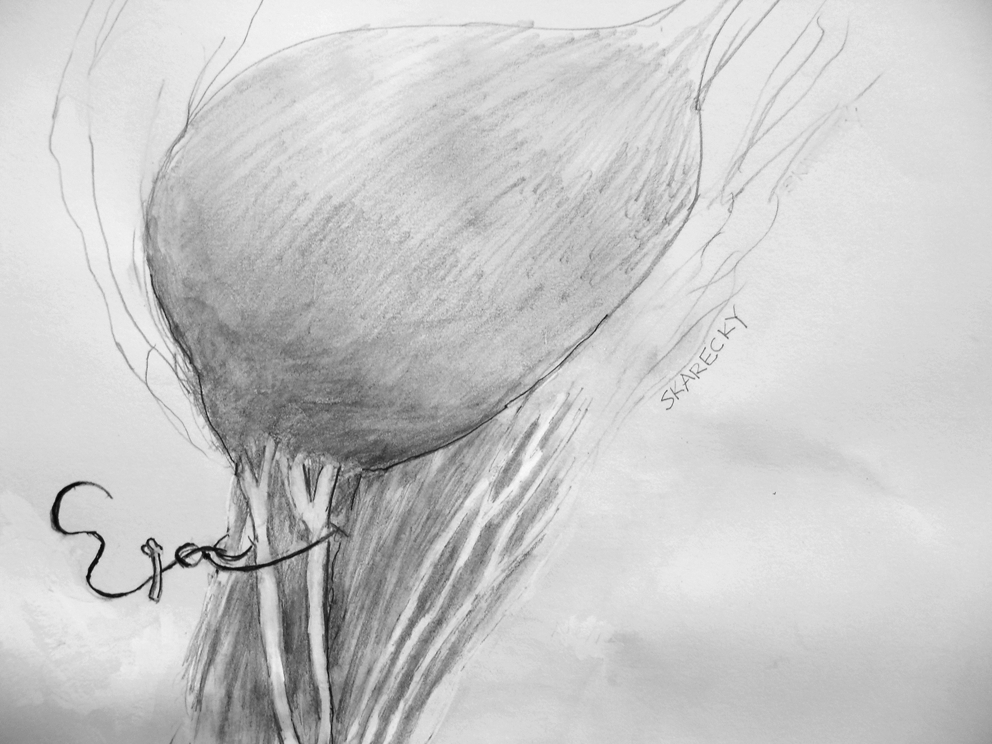
The completed pedicle stitch. A small Hem-o-lok is used to cinch down on the neurovascular bundle (NVB) loop to achieve cautery-free transaction of the NVB.
After the prostate has been removed and the VP and NVB demonstrate no arterial bleed, attention is directed to the anastomosis. If bleeding is encountered along the VP, the Hem-o-lok clip can be further cinched. If there is bleeding outside of the existing stitch, further throws can be placed as needed with additional sutures or with the pedicle stitch itself, which can save time. Although we have not found this necessary to alleviate concern for slippage or loosening of the stitch within the Hem-o-lok, with the potential for a postoperative bleeding event, a Lapra-Ty® clip can be placed just above the Hem-o-lok to prevent this from occurring with little additional cost or effort. In our early attempts at this pedicle stitch technique, when the stitch was cut inadvertently, we were easily able to replace a new pedicle stitch to the VP in a similar technique without difficulty or any significant time delay.
Results
The TA suture was applied to 143 vascular pedicles in 74 men. In 4 of the first 10 cases, the suture ligature was inadvertently cut, but with experience, this is now a rare event. In all four, bleeding was minimal but necessitated extra time to suture ligate the bleeding vessels before continuing. Looking only at these four patients, three had EBLs of 50 mL, and the EBL of the remaining patient was 150 mL.
We compared the TA suture group to the preceding 74 men controlled by the athermal bulldog clamp (Table 1), and both were similar in clinical features. Both groups are similar as far as Gleason, C-stage, P-stage and + margins. Three complications occurred in each group (4%): The TA group had two readmissions (ileus, spontaneous port-site bleed) and bilateral femoral nerve palsy, resolved after day 4, and the control group had one readmission (ileus), an infected lymphocele, and a venous bleed necessitating 2 units of blood. We reviewed surgical videos from a small subset of pedicle stitch patients, and the time from control of vessel to take down of the dorsal venous complex averaged 23 minutes. For the bulldog technique, video times were longer, averaging 39 minutes, partly for controlling the bleeding pedicle with 4-0 polyglactin after the prostate is removed. Our early limited findings of sexual function via the stitch method, for men of all ages with a International Index of Erectile Function-5≥15, potency was 24% at 9 months and 44% at 15 months. These results are similar to our earlier findings using the bulldog clamp.
Also known as Sexual Health Inventory for Men-5 (SHIM-5).
TA=tension adjustable; PSA=prostate-specific antigen; AUA=American Urological Association; IIEF=International Index of Erectile Function; Hgb=hemoglobin.
Discussion
The object of nerve-sparing radical prostatectomy is to remove the prostate and seminal vesicles without damaging the delicate NVBs. The mainstay to nerve preservation is avoidance of nerve transection followed by reduction of traumatic injury.
1
Monopolar and equally bipolar electrocautery cause significant thermal injury to adjacent tissue.
2,
Based on the concept of temporary vascular occlusion advocated in laparoscopic partial nephrectomy, 9,10 bulldog clamps were selected, testing the feasibility of temporary vascular occlusion of the prostatic vascular blood supply. 1 –3 Subsequent follow-up has shown a significant benefit of cautery-free technique on potency up to four-fold at 3 months, 11,12 and it retains a higher percentage of potent men at 2 years by 25%. 13,14
Bulldog clamps take a degree of laparoscopic skill to place correctly and remove, which practitioners may not feel comfortable at performing. The concept of suture ligation instead of the bulldog clamps was originally suggested in 2004 (Scott Miller, M.D., personal communication). During transection of the VP with simple ligation, however, the suture loosened, and as vessels retracted, bleeding was poorly controlled. Recently, based on videos of robot-assisted and or laparoscopic partial nephrectomy, the concept of adjustable tension with a Hem-o-lok offered a simple solution. When the VP is transected and vessels retract, additional tension can easily and quickly be applied, controlling bleeding, as nicely demonstrated in the video clip. The TA knot mimics the effectiveness of the bulldog method and is placed in the exact same location on the VP. With experience, one is more confident of this position, which, of course, varies from patient to patient based on oncologic issues.The suture is easier and quicker to apply and eliminates the time and effort of oversewing the VPs after removing the bulldogs.
We offer this as an alternative technique over the commonly used technique of applying multiple Hem-o-lok polymer clips during transection of the VP. To appropriately place Hem-o-lok clips, traction is needed to develop the windows for a skilled assistant to properly apply the clips. The squeezing of the Hem-o-lok applier to engage to clip administers a large amount of pressure just to engage the locking mechanism. When these clips are applied to too large a bundle, they often fall off or are misplaced, with resultant bleeding and subsequent use of electrocautery or reapplication of the clips. Another issue is that the surgeon does not place the clips and are again dependent on the assistant for placing them, which brings us back to the limitations of the bulldog technique. With the pedicle stitch, the surgeon places it exactly where wanted. We feel that the TA pedicle stitch technique offers another simple athermal means to control the VP with minimal traction.
Conclusion
This series represents the description of a simple alternative for athermal control of the VP. The technique is safe, because no postoperative bleeding events have been encountered, and is technically easier and faster than using bulldogs. It provides the surgeon with more control over ligation of the VP and is not assistant dependent.
Footnotes
Disclosure Statement
Dr. Ahlering is a consultant for Phillips and Astellas. For the remaining authors, no competing financial interests exist.